
Abstract
Background:
In the early months of the COVID-19 pandemic, frontline nurses faced unprecedented challenges and were often excluded from decision-making, creating a critical research gap as their valuable insights were not captured, hindering the development of effective public health strategies.
Objective:
This study aimed to explore lessons learned, recommendations, and pearls of wisdom from frontline nurses who cared for COVID-19-positive patients in the United States during the early phases of the pandemic.
Methods:
The study employed a descriptive qualitative approach. Data were collected via virtual semi-structured interviews with 30 frontline nurses between July 2020 and November 2020. Analysis utilized reflexive thematic analysis by a 3-member coding team. Rigor was maintained through frequent team debriefing, reflexive discussions, the inclusion of multiple quotation exemplars, a national recruitment strategy, and an audit trail. Reporting followed the Consolidated Criteria for Reporting Qualitative Research checklist for qualitative research.
Findings:
Codes relating to nurses’ lessons learned included leadership actions and visibility, innovations in patient care, teamwork and flexibility, and preparedness. Nurse recommendations encompassed soliciting nurses’ voices, leadership competencies and enhancing emergency response preparedness, mental health support, and ensuring sufficient resources. Pearls of wisdom for future generations emphasized self-care, mindfulness, effective communication, and engagement with colleagues and family.
Conclusions:
Effective pandemic preparedness must be managed as a systematic approach. Neglecting these actions risks repeating catastrophic mistakes in future health crises, compromising care quality and patient health outcomes. Improvements need to occur in nursing education, leadership training, and health care support for nurses.
The COVID-19 pandemic exposed significant gaps in the preparedness of health care systems worldwide, profoundly impacting nurses who served as the backbone of patient care during this crisis. Globally, nearly 7 million lives were lost, 1 and the United States faced distinct challenges due to its decentralized health care infrastructure and inconsistent public health responses. To enhance preparedness for future public health crises, it is critical to understand the insights and recommendations of frontline nurses in the United States, who bore the brunt of the pandemic’s early and uncertain phases.
As the pandemic unfolded, numerous publications highlighted broad lessons learned and future considerations. However, these works often provided generalized overviews without delving deeply into the firsthand perspectives of frontline nurses caring for COVID-19 patients during the early, speculative phase of the pandemic.2-6 This study aimed to fill that gap by capturing detailed recommendations expressed by US nurses in the height of the initial wave of the pandemic, a perspective largely absent in existing literature.
A systematic review by Temeng et al 7 identified how nurses coped with severe viral outbreaks globally, but it lacked real-time accounts of their lessons learned and recommendations for future generations of nurses. Similarly, studies from Italy and Canada conducted during the first wave of the pandemic provided insights into the impact of the early phase of the pandemic on nurses in universal health care systems.8,9 These studies describe themes like communication, leadership visibility, and psychological support but did not address the unique context of the United States, where health care infrastructure, policy responses, and resource availability varied greatly. The invaluable lessons learned and recommendations can improve the nursing profession’s pandemic responsiveness. It is important to capture not only what was done amid the catastrophe but what frontline nurses would recommend being done differently and their pearls of wisdom for the future.
Purpose
This study explored the insights and recommendations of US frontline nurses who cared for patients with COVID-19 infection during the pandemic’s first wave (March-May 2020). By capturing lessons learned, recommendations, and pearls of wisdom, this research offers critical guidance to strengthen the nursing profession, health care leadership, and policymaking in preparation for future crises.
Methods
A descriptive qualitative design was used with data collected from semi-structured interviews conducted virtually. Qualitative methods are fully described in our first publication of mixed methods findings 10 and summarized below.
Population, Sampling, and Recruitment
Registered nurses (RNs) were purposively sampled from across the United States and recruited through social media campaigns (Facebook and Instagram). Inclusion criteria were as follows: (a) RNs practicing in a hospital; (b) providing direct care to adult COVID patients hospitalized on an adult medical, surgical, obstetric, COVID, or critical care unit or emergency department; and (c) had a minimum of 3 years of RN experience. Three years of experience in Benner’s Novice to Expert theory can advance nurses from novice to proficient, allowing them to see the big picture and provide holistic care. 11 Nurses were informed of the study purpose, the roles of the research team, and the team’s interest in the topic during a screening call prior to participating. Participants were recruited until data saturation was reached as determined through ongoing team discussions.
Data Collection
One interview per participant was conducted from July 2020 to November 2020. On average, interviews lasted 60 minutes. A semi-structured interview guide was created to explore the participant’s personal and professional experiences during the first wave of the pandemic, focusing on lessons learned, recommendations, and pearls of wisdom for future generations of nurses. Demographic questions were included at the end. The guide was tested with 2 frontline nurses for feedback on content, flow, and cohesion. Two female authors (PhD and DNP prepared nurses) with training and expertise in qualitative research methods conducted the interviews via Zoom videoconferencing. Interviewers did not have any relationship with participants prior to study commencement. All interviews were audio-recorded, transcribed verbatim, redacted for identifying information, and stored on a password-protected server.
Data Analysis
Data were analyzed using Braun and Clark’s reflexive thematic analysis process 12 : (1) data familiarization from reading the transcripts several times to get an overall feeling of the content and patterns, (2) generation of initial codes, (3) collating codes into overarching themes, (4) identifying the supporting data for the themes, (5) defining and labeling themes, and (6) final analysis of codes and themes.
Analysis was carried out by a 3-member coding team (2 PhD and 1 DNP prepared nurses) who were all trained and experienced in qualitative analysis. Analysts reviewed all transcripts to familiarize themselves with the data. Two analysts then independently coded the first 5 transcripts to develop an initial codebook, which was audited by the third analyst. One analyst coded the remaining transcripts and iteratively modified the codebook. Regular team meetings were convened throughout the coding process. The 3 analysts independently grouped codes into overarching themes, which were finalized through discussions to reach consensus. All analysts participated in identifying supporting data for themes, defining and labeling themes, and finalizing the analysis. Major themes presented in this paper include nurses’ lessons learned, recommendations, and pearls of wisdom. Other major themes that emerged from these data are presented elsewhere. 10 ATLAS.ti was used to manage the data (ATLAS.ti GmbH, Berlin, Germany). 13
Rigor and Reflexivity
Multiple strategies were used to maintain rigor in the analysis. To promote credibility (confidence placed in the truth of the findings) and confirmability (representativeness of findings in relation to participants’ experience), reflexive field notes were taken after the interviews and discussed during debriefing and analysis meetings, an audit trail was maintained, multiple quotation exemplars were used to illustrate the experiences of most participants, and findings were compared to prior research. Feedback on findings was obtained during a poster discussion session at a regional nursing research conference. To ensure dependability (likelihood of replicability of findings) an audit trail and open dialogue among coders were maintained. To promote transferability (extent to which findings can be applied in other situations), a national recruitment strategy was used and thick description of findings with relevant quotes to support themes was provided. 14 Reporting of the study adheres to the Consolidated Criteria for Reporting Qualitative Research (COREQ). 15
Results
A total of 30 frontline RNs participated; the majority were female (90%) and white (n = 26; Hispanic = 1; Native American = 1; Asian = 1; African American = 1). All individuals who participated in the screening call chose to participate. Participants were between the ages of 25 and 62 years (mean = 40; SD = 10.6). All participants had a bachelor’s degree or higher and practiced between 3 and 33 years (mean = 13; SD = 9.3). Most participants were from large urban or academic medical centers (85%) with the remaining from community or critical access hospitals (15%). Nurses worked in Florida, Georgia, Illinois, Indiana, Michigan, New Jersey, New York, Ohio, and South Carolina. All states except Georgia and Florida had shelter in place orders at the time of data collection.
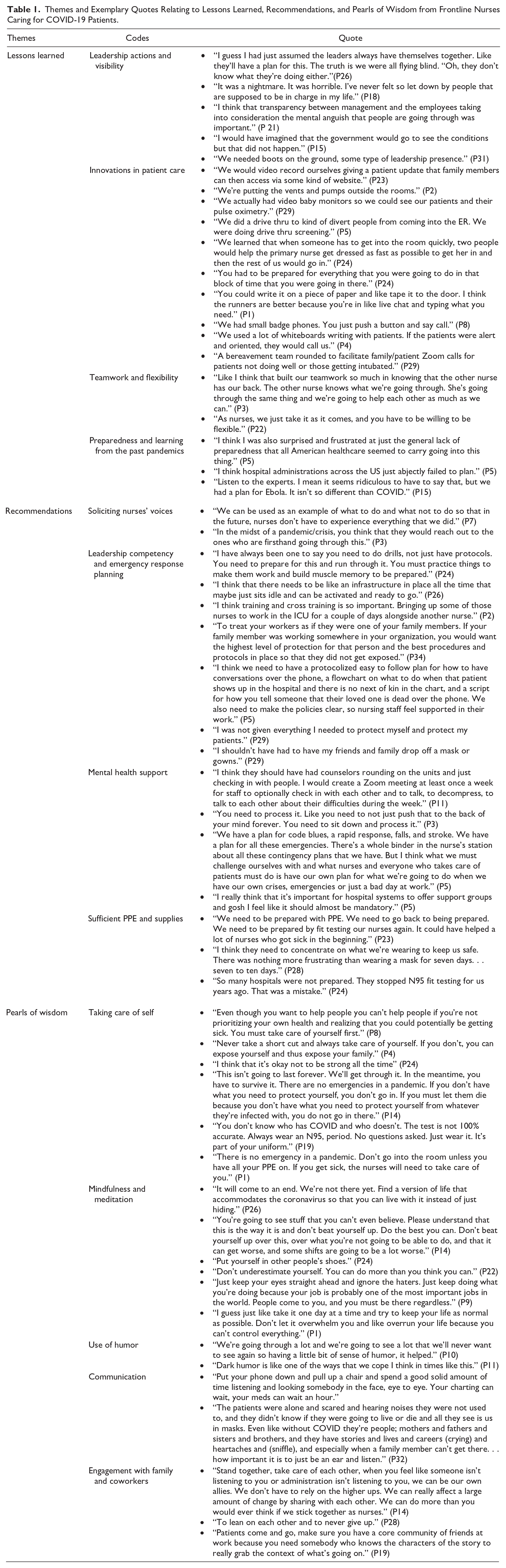
Codes supporting the themes of the lessons learned, recommendations, and pearls of wisdom are described in the narrative below, along with exemplary quotes to support each code. Additional quotes are provided in Table 1.
Themes and Exemplary Quotes Relating to Lessons Learned, Recommendations, and Pearls of Wisdom from Frontline Nurses Caring for COVID-19 Patients.
Lessons Learned
Lessons learned centered around leadership actions and visibility, innovations in patient care, teamwork and flexibility, and being prepared by learning from past pandemics.
Leadership actions and visibility
The absence of a cohesive national pandemic response plan and inconsistent leadership across states, hospitals, and units were key lessons for nurses, many of whom felt the lack of leadership visibility, particularly on units facing significant patient care challenges. One nurse shared the frustration of feeling unsupported: “Management never came around. . . nothing. They were just like, ‘Bye, we don’t need you.’ That’s how I felt” (P11).
The disconnect between leadership and frontline workers was particularly evident when leadership’s absence or lack of transparency intensified feelings of isolation and abandonment. As one nurse described, “The nurses are just left picking up the pieces of the rationality of the leadership as a whole” (P19). This signifies a need for stronger leadership engagement and clearer communication to avoid gaps between decision-makers and those directly providing patient care.
Innovations in patient care
Nurses developed inventive approaches to reconceptualize patient safety in response to the new threats posed by the pandemic. They faced challenges in minimizing COVID-19 exposure to patients, coworkers, the community, and themselves, which complicated care delivery and communication. As one nurse stated, “I felt that the nurses really had to drive the issues of safety” (P21). Examples of safety innovations included redesigning care delivery and physical spaces, such as placing ventilators and pumps outside of patient rooms and implementing drive-through care to reduce emergency room entries.
Despite their best efforts, the virus claimed many lives. “We had so many deaths. God, everyone was dying. I was a death coach for these family members” (P3). To address the emotional toll of large-scale death and dying, nurses introduced innovations to preserve human connection. One example was the creation of bereavement kits, as one nurse shared, “We created a bereavement kit that contained the patient’s hair and fingerprints so families could have a keepsake” (P37).
Teamwork and flexibility
Nurses recognized the importance of strong teamwork in navigating the challenges of the pandemic, often relying on one another when external support fell short. As one nurse reflected, “In the middle of the chaos, we realized that we were also each other’s patients” (P26). The support from colleagues became essential to coping with the overwhelming stress and isolation.
Flexibility also emerged as a vital lesson. Nurses learned to adapt quickly to the rapidly changing health care environment, adjusting to new information and evolving circumstances. One nurse summed it up by saying, “As nurses, we just take it as it comes, and you have to be willing to be flexible” (P22). This adaptability was key to maintaining resilience and delivering care during an unpredictable crisis.
Preparedness and learning from past pandemics
Nurses expressed frustration over the country’s lack of preparedness for the COVID-19 pandemic, particularly in planning, supply management, and personal protective equipment (PPE). As one nurse noted, “I was surprised and frustrated at just the general lack of preparedness in American healthcare” (P5). Despite warnings from past outbreaks like Ebola, the PPE shortage demonstrated a significant gap in readiness. One nurse reflected, “We had quite a lot of warning. . . Be prepared for the worst and have enough PPE” (P34).
Nurses pointed to failures at both the national and hospital levels, stressing that the lack of coordination affected worker safety and eroded public trust. As one nurse stated, “It would be nice if we had a preparedness plan. We didn’t have that set up” (P22). Ultimately, nurses stressed the importance of proactive planning. Reflecting on lessons learned, one nurse stated, “We had a plan for Ebola. It isn’t so different than COVID” (P15), while another concluded, “The lesson I learned is to be prepared” (P28).
Recommendations
Nurses offered many recommendations for future pandemics, disasters, and crises. These included soliciting nurses’ voices, the need for leadership competencies to address emergency response and preparedness, mental health support, and an adequate supply of PPE. They recommended that future disaster management plans address multidimensional issues. “When talking about taking care of an unknown disease and what it takes to do it—professionally, personally, spiritually, and mentally. I think that needs to be addressed even in school. It needs to be taught and not something that just magically pops up in our lives” (P8).
Soliciting nurses’ voices
Nurses expressed frustration over being excluded from decision-making despite providing direct care. They believed involving frontline nurses could improve care protocols, particularly regarding critical issues like PPE. One nurse noted, “These leadership administrators. . .are the ones making these decisions, and it just blows my mind how you don’t ask the people who are in it” (P3). Nurses indicated that their insights could enhance safety and care, as one stated, “We see these people every single day and we’re not sitting there at the same table with them about PPE standards” (P18).
Beyond local settings, nurses voiced concerns about exclusion from broader health policy discussions. One remarked, “At the highest level, it’s very interesting to know that the CDC and the World Health Organization don’t have frontline nurses on the group” (P18). Including nurses’ perspectives in decisions could better reflect care realities and improve health care system efficacy and public health outcomes.
Leadership competency and emergency response planning
Nurses described that effective leadership is critical for emergency preparedness. They recommended proactive, forward-thinking approaches, including dedicated teams for anticipating potential crises: “We need an office full of people who sit around dreaming up scenarios. Like military intelligence does. You can only prepare for what you expect” (P32). Such planning would enable health care systems to handle diverse emergencies.
Nurses also stressed the need for cross-training, adequate supplies, and robust infrastructure: “We should have the supplies, equipment, and the infrastructure to support our healthcare systems, we need to have ways that we can do that, and plans on how we’re going to do that” (P21). Leadership should oversee logistics, ensure clear communication, and foster a culture of readiness to avoid scrambling during crises. By prioritizing planning, coordination, and resource management, nurses believed health care systems could better protect staff and patients during public health emergencies.
Mental health support
Nurses described the urgent need for mental health resources to support their well-being in future crises. The intense physical, emotional, and mental demands of pandemic care led to burnout, with nurses emphasizing that self-care was crucial not only for their own health but also for the quality of patient care. As one nurse described, “This is unlike anything. . . the most physically, mentally, and emotionally exhausting work we’ve ever done” (P14). Nurses emphasized the importance of taking time off to rest, advising, “Take care of yourself, whatever that means” (P5), and stressed that showing up to work in a compromised state ultimately harms both the individual and the team.
Beyond individual self-care, nurses advocated for structural changes within health care settings to promote mental well-being. They suggested having counselors available to check in with staff regularly, creating spaces for reflection, and organizing debriefing sessions and support groups to allow staff to process their experiences. One nurse proposed, “We need to have a space to go to reflect and meditate. . . like a reflection room” (P22). Additionally, nurses recommended fostering a supportive work environment through strong peer networks: “Make sure you have a core community of friends at work” (P19). These suggestions demonstrate the need for both individual strategies and institutional support to protect the mental health of health care workers in high-stress environments.
Sufficient PPE and supplies
A major concern among nurses was the lack of adequate PPE, which significantly impacted their ability to safely care for patients. Nurses had to ration, reuse disposable supplies, and even rely on family and community members to bring in PPE. The absence of proper protection increased stress and compromised patient care. As one nurse pointed out, “I just feel like it needs to be a requirement to have the PPE to protect our nurses. Like soldiers don’t go to battle without their guns. Like their guns protect them” (P3).
Beyond the immediate shortage, long-term gaps in PPE preparedness, such as the halting of mask fit testing, further endangered frontline workers. Nurses recommended a return to proactive safety measures, including fit testing and regular training, to ensure protection during future crises.
Improved access to PPE would not only reduce stress but also enable better care delivery. One nurse stated, “If we had unlimited PPE, it would have been a lot less stressful. I think we would have provided better care for people” (P26). Ensuring proper PPE supplies and fit testing are crucial steps for supporting health care workers and improving patient care in future emergencies.
Pearls of Wisdom
Nurses shared pearls of wisdom from caring for COVID-19 patients: taking care of self, mindfulness and meditation, use of humor, communication, and engagement with family and coworkers.
Taking care of self
Nurses emphasized the critical need for self-care, particularly during the pandemic, recognizing their health and safety had to come first. As one nurse explained, “If we don’t take care of ourselves, we’re not going to be able to care for others” (P3). Self-care was essential to prevent physical exhaustion and maintain emotional well-being. Another nurse reflected, “If we just keep pushing our feelings to the back, we’re going to get PTSD” (P3).
Nurses stressed prioritizing health by recognizing exposure risks and taking precautions. One noted, “Even though you want to help people, you can’t help people if you’re not prioritizing your own health” (P8). Another reminded, “There’s no emergency here until you’re safe. If you get COVID, who’s going to take care of the patient?” (P16).
Adherence to safety protocols was also vital. “Always wear an N95, period. No questions asked. Just wear it. It’s part of your uniform” (P19). The core lesson was clear: Nurses must protect themselves—physically and emotionally—to effectively care for others.
Mindfulness and meditation
Nurses recommended mindfulness and meditation as essential practices to maintain emotional balance and resilience during the pandemic. One nurse stated: “Be mindful and meditate and try to do self-care techniques more” (P11). These practices helped nurses stay grounded amidst the chaos and uncertainty.
Another nurse reflected on the need for a mental shift to navigate the ongoing crisis, suggesting, “Find a version of life that accommodates the coronavirus so that you can live with it instead of just hiding” (P26). Nurses also shared the value of maintaining perspective and not internalizing every challenge, with one adding, “At the end of the day, you’re not alone” (P10).
Mindfulness was also framed as a way to maintain personal boundaries, avoid self-blame, and focus on the present moment. As one nurse advised, “Do the best you can. . . and some shifts are going to be a lot worse” (P14). This advice, alongside reminders to be patient with oneself, reinforced the importance of resilience through mindful awareness.
Use of humor
Nurses found humor essential for managing stress and maintaining emotional resilience during the pandemic. As one nurse shared, “Even as scared as we were, you must hide that. Humor works, it goes a long way” (P9). Another nurse explained, “We could have our dark humor moments in the hallway. . .dark humor is one of the ways that we cope” (P11). Humor not only provided emotional relief but also helped nurses process the traumatic experiences of the pandemic. This highlights the crucial role of humor in supporting nurses’ mental well-being in high-stress environments.
Communication
Communication was essential during the pandemic. Nurses emphasized clear, open communication for managing patient care and fostering connections among colleagues and patients. One nurse explained, “You’ve got to communicate. . . make sure everybody is working together in troubleshooting what comes up” (P4). This collaborative approach ensured safety and contributed to patient survival.
Beyond logistics, communication humanized patient care. One nurse shared, “I’ve spent a lot of time going in with patients that are really angry, and the reason is that they were lonely, secluded, and didn’t feel they were being heard” (P24). Nurses stressed the emotional power of listening, especially for isolated patients. “The patients were alone and scared. . .when a family member can’t get there. . .how important it is to just be an ear and listen” (P32). Effective communication, through active listening or problem-solving, was integral to patient care and emotional support.
Engagement with family and coworkers
Nurses described the essential role of coworker and family support during the pandemic. Colleagues provided critical strength, with one nurse noting, “We must take care of each other. That’s who we are” (P29), while another stated, “We can be our own allies. . . we can do more than you would ever think if we stick together as nurses” (P14).
Family support was equally important, with nurses advising, “Love and cherish your family now. Don’t think that you have time because you never know” (P36). In challenging moments, these connections helped nurses maintain resilience. Having a core group of supportive colleagues also allowed nurses to navigate the emotional toll of the pandemic, as one put it, “Make sure you have a core community of friends at work” (P19).
Discussion
Through this qualitative study, we sought frontline nurses’ perceptions about lessons learned, recommendations, and pearls of wisdom while caring for patients hospitalized with COVID-19 in the United States during the first wave of the pandemic. Although other investigators have reported the impact of COVID-19 on nurses mental and physical health,10,16-18 few have elicited specifically what nurses learned from the COVID-19 pandemic and how to address future pandemics. The prominent messages shared by nurses in this study that cut across the 3 categories (lessons learned, recommendations, and pearls of wisdom) were about (1) pandemic preparedness (past and future), (2) well-being of nurses, (3) patient care innovation, and (4) leadership.
Pandemic Preparedness
Nurses were surprised, alarmed, and frustrated by the lack of a national pandemic plan and lack of PPE to protect health care workers. Nurses were adamant that we must address emergency response and preparedness planning and that drills be routinely enacted to carry out the plan. Training of pre-licensure students, nurses, and leaders in preparedness competencies is critical. Our findings demonstrate a significant gap in pandemic preparedness and planning, demonstrating that lessons learned from past crises were not applied to the COVID-19 response. This gap stresses the importance of involving nurses in the early stages of planning and policy development. By capturing nurses’ perspectives on these shortcomings, our research contributes to the larger conversation on how we can better prepare for future pandemics by ensuring frontline workers are integral to the process. The focus on US nurses offers unique insights, particularly considering the complex structure of the US health care system, which has distinct challenges related to staffing, resource allocation, and federal versus state-level coordination that may not be as prevalent in other countries.
Well-Being of Nurses
Nurses in this study described strategies to address COVID’s impact on their well-being. Self-care, including self-protection and adherence to full PPE protocols, was emphasized even when it might negatively affect patients. Prioritizing nurses’ self-care to protect patients’ health must be central to training and the profession, addressing competing demands that force nurses to choose between self and others. Mindfulness, meditation, and humor were effective coping strategies. These findings align with research showing the positive impact of resilience strategies, such as acceptance and mindfulness, on reducing stress and promoting well-being. 19 Nurses also recommended organizational supports like support groups, therapy animals, and mental health rounding. These interventions are critical to addressing the mental health challenges nurses face. Communication with coworkers, patients, and leadership was central to safety and well-being. Nurses recommended camaraderie and mutual support, echoing other studies on the importance of connectivity and community among staff.8,20,21 These strategies are essential for promoting nurses’ resilience and long-term coping. While similar coping strategies may have been reported globally, the intense stressors experienced by US nurses—particularly in the context of widespread health care disparities and political tensions—offer important insights into the unique challenges of nursing in the United States.
Patient Care Innovation
Innovative approaches to patient care were used, including technical solutions like ventilators and IV pumps outside of patient rooms, and humanistic care through video calls, bereavement kits, and team rounds. These adaptations reflect the flexibility and teamwork necessary during a pandemic. Nurses described the importance of collaboration in providing safe, effective care, which aligns with other research that highlights teamwork and innovation in times of crisis.21,22 The innovation reported by US nurses, however, was often constrained by fragmented health care delivery systems and varying levels of preparedness across different states, which further demonstrates the need for coordinated, national-level planning to support frontline caregivers.
Leadership
Nurses expressed disappointment in leadership, citing a lack of presence, transparency, and effective pandemic plans. Pandemic leadership competencies were minimal, and nurses were frustrated by insufficient supplies and exclusion from decision-making. There was a clear need for leaders to be more present, communicative, and involved in developing response plans. The gaps in leadership competencies can be addressed through education, including simulation and interactive training. 23 Leadership must include task, people, and adaptive competencies to manage dynamic crisis situations. 24 Nurses identified the need for leadership that values their input and reflects a commitment to addressing workforce needs. The findings illustrate a distinct issue within the US health care system, where leadership often lacked coordination and consistent presence across the vast network of public and private health care facilities. This research underscores the necessity for strong, centralized leadership to guide local health care institutions during future crises.
Strengths and Limitations
This study focused on capturing nurses’ perspectives in the United States, which may limit the generalizability of findings to global health contexts. Participants from 9 states and diverse care settings were included, with comparisons made to international findings. Limitations include sample homogeneity in terms of race, ethnicity, and gender. No participants were recruited from the Western United States, posing a geographic limitation. Reliance on social media for recruitment may exclude individuals not active on these platforms. The authors, experienced nurses with over 100 combined years of clinical and leadership experience, aimed to represent nursing perspectives, though insights from other disciplines and public health stakeholders may have been overlooked.
Recommendations for Future Research
Future research should assess whether the recommendations made by nurses have been achieved. This includes evaluating whether frontline nurse training, health care leaders’ preparedness, and well-being initiatives have been implemented. Key questions should focus on whether nurses have been included in the development of pandemic strategies and whether leadership competencies are integrated into educational programs for future leaders. Nurses’ voices must remain central in research to avoid marginalization and ensure better preparedness in future crises.
Implications for Policy and Practice
This research supports 3 key implications for policy and practice: (1) enhancing pandemic planning and preparedness, (2) supporting coping strategies for nurse well-being, and (3) improving leadership competencies. Pandemic preparedness requires national, state, and local action. Education for both pre-licensure and practicing nurses on pandemic response is essential. 25 Plans must ensure safe working conditions, fair pay, and adequate resources. Training, communication, leadership competencies, and workforce protection should be prioritized.18,25,26
To support nurses’ well-being, system-level interventions are needed alongside individual resources. Mental health resources must be more accessible, with barriers like stigma and time constraints addressed.27,28 Health care organizations must ensure proper PPE and staffing for safe care delivery.
Leaders must collaborate with nurses to create and evaluate comprehensive pandemic response plans. While the pandemic has passed, it is crucial to reflect on the lessons learned from frontline staff. Health systems must engage in ongoing conversations to ensure that nurses are included in future preparedness planning, both to heal from the trauma of the pandemic and to prevent the “never looking back” mentality that could undermine future crisis responses.
This study captures the critical lessons frontline nurses in the United States learned during the COVID-19 pandemic, with a focus on pandemic preparedness, nurses’ well-being, patient care innovation, and leadership competencies. Unlike similar studies conducted globally, this research shows the distinct challenges and recommendations from US nurses, highlighting gaps in training, resources, and support within the American health care system. By amplifying these frontline voices, this study provides essential insights to strengthen health care resilience and preparedness for future public health crises.
Footnotes
Author Contributions
All authors contributed to the conceptualization, data collection, analysis, writing, review, and editing of this manuscript. Study conceptualization and data collection was conducted while lead author (MHG) was a PhD student at University of Michigan, while analysis and manuscript preparation were completed during her postdoctoral fellowship at Duke University and the Durham VA.
Data Availability Statement
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approvals
The University of Michigan Health Sciences and Behavioral Sciences IRB deemed this study exempt (HUM00183253).
Disclaimer
The contents do not represent the views of the University of Michigan, Duke University, the US Department of Veterans Affairs, or the United States Government.