
Abstract
Background:
Women with breast cancer are more prone to bone loss, joint pain, and other musculoskeletal symptoms, especially those receiving aromatase inhibitors and/or undergoing ovarian suppression therapy. Bone and joint problems can affect their quality of life and treatment adherence. Thus, the management of bone health is of clinical importance for this population.
Objective:
This study aimed to systematically develop a multicomponent bone health management intervention for women with breast cancer and assess the acceptability of the intervention program.
Methods:
The Rebuilding Osteo Strength with Exercise (ROSE) program for women with breast cancer was developed based on biological mechanisms, patient needs, evidence-based practices, theories, and stakeholder consensus using the Medical Research Council framework. An open-pilot study and post-intervention interviews were conducted to assess the acceptability of the ROSE program.
Results:
The ROSE program consisted of 6 modules, which integrated progressive exercise, bone health education, and behavior change strategies. Eight eligible patients were recruited during the open-pilot study, and all participants considered the program acceptable. Six patients accepted the post-intervention interview. Four themes emerged from the post-intervention interview: perceived benefits of participating, barriers to adherence, facilitators to adherence, and suggestions for optimization.
Conclusions:
The ROSE program is an acceptable bone health intervention program for women with breast cancer. Future refinements will be made before efficacy testing.
Trial registration:
The study was retrospectively registered with the Chinese Clinical Trial Registry, registration number ChiCTR2300072208.
Adjuvant endocrine therapies, such as aromatase inhibitors (AIs), goserelin, and leuprorelin, reduce estrogen levels to improve oncological outcomes in women with estrogen receptor-positive breast cancer. 1 However, these treatments negatively impact bone and joint health, increasing the risk of bone loss, joint pain, and other musculoskeletal symptoms.1,2 AI-associated arthralgia is a common adverse event, with a systematic review estimating its prevalence at 50% among women with breast cancer. 3 Moreover, a cross-sectional study of 1692 women with breast cancer found that women receiving endocrine therapy had a 2.91-fold higher cumulative incidence of osteoporosis than healthy women. 4
Bone and joint problems affect patients’ quality of life and treatment adherence. Osteoporotic fractures lead to long-term disability and reduced independence, placing a significant health burden on individuals and contributing to substantial health care costs. 5 Additionally, in a prospective study of 1976 patients, a 10% increase in arthralgia was associated with a 20% increase in the risk of nonadherence with endocrine therapy. 6 However, nonadherence and non-persistence to endocrine treatment negatively affect event-free and overall survival. 5 Thus, the management of bone health is of clinical importance in women with breast cancer.
Bone Health Management for Women With Breast Cancer
Impact and resistance training can stimulate bone formation and attenuate bone loss. As early as 2010, the American College of Sports Medicine specifically emphasized exercise as an intervention strategy to manage treatment-related musculoskeletal side effects such as bone loss and arthralgias, as well as other health problems faced by women with breast cancer. 7 Studies on resistance exercise and impact training have confirmed that a 12-week to 1-year exercise program combining medium- to high-intensity resistance training and impact training can reduce bone loss and improve body composition in women with breast cancer.8,9 Similarly, increased joint movement and muscle strength also help prevent cartilage degeneration, inhibit inflammation, and relieve osteoarthritis symptoms. 10 In 2019, the Hormones and Physical Exercise (HOPE) trial researchers observed that a year-long aerobic and resistance combined exercise significantly reduced joint pain in women with breast cancer receiving AIs. 11 However, exercise interventions that do not address other self-management strategies to improve bone health miss opportunities to promote bone health in women with breast cancer more holistically.
In addition to exercise, studies also demonstrated the role of diet, 12 vitamin D, 13 and pharmacological interventions 14 in bone health. Guidelines and expert consensus recommend that bone health management for women with breast cancer includes appropriate calcium and vitamin D supplements, a balanced diet, sufficient sun exposure, regular exercise, and timely pharmacological interventions. 15 Although several studies, such as those by Abdel-Razeq et al 16 and Tseng et al, 17 focused on various aspects of bone health management through comprehensive programs, their interventions primarily provided information rather than promoting actual behavior change. However, providing information is only one of the strategies for managing bone health. Effective bone health management also requires actual patient behavior changes to ensure that interventions are implemented. Therefore, developing a comprehensive intervention program that not only includes comprehensive bone health management but also effectively promotes behavior change has important application value.
Purpose
Our research team developed the Rebuilding Osteo Strength with Exercise (ROSE) program under the Medical Research Council (MRC) framework to promote bone health management in women with breast cancer. 18 The program will be described according to the TIDieR checklist and guide. 19 In this study, we aimed to (1) describe the process for developing the ROSE program and (2) evaluate its acceptability through metrics such as recruitment, retention, adherence, satisfaction, and participant feedback.
Methods
According to the MRC framework, developing complex interventions involves iterative and overlapping phases. In this study, the development phase included 5 steps: (1) identifying biological mechanisms, (2) identifying patient needs, (3) identifying evidence-based practices, (4) applying behavior change theories, and (5) modeling the program. Each step informed the next, ensuring the program was evidence-based, patient-centered, and practically implementable. Afterward, we conducted an open-pilot study along with post-intervention interviews with participants to test the program’s acceptability. The process of the study is presented in Figure 1.
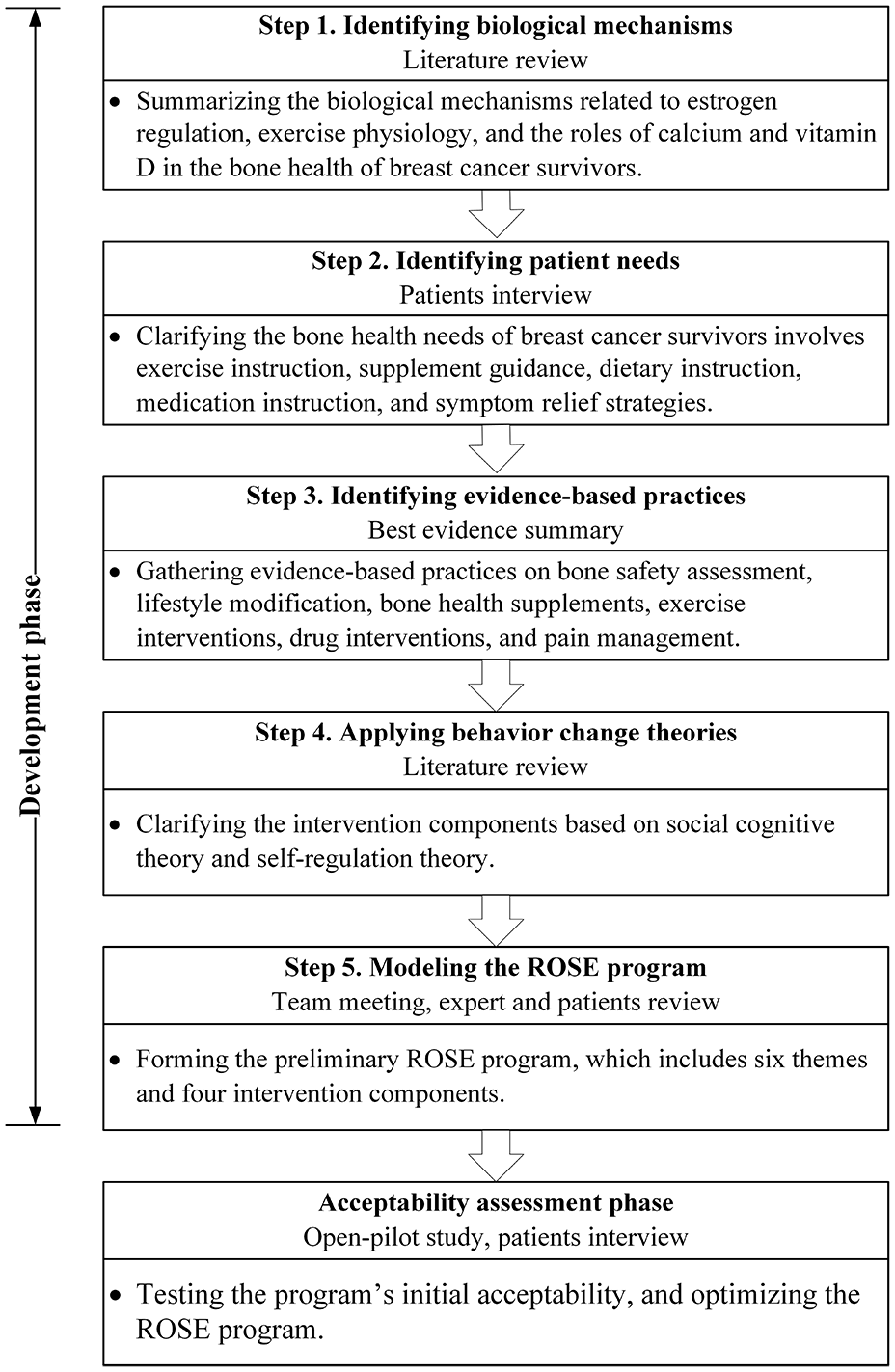
Process of the study design guided by the MRC framework.
Phase 1: Program Development
Phase 1.1: Identifying biological mechanisms
This phase focused on identifying key biological mechanisms to guide intervention design, providing a theoretical foundation for selecting intervention components tailored to women with breast cancer.
We conducted a targeted literature review in PubMed, Web of Science, and CNKI databases to identify studies published between 2011 and 2021. The search used Boolean combinations of keywords such as breast cancer, bone loss, joint pain, and biological mechanisms and included studies published in English or Chinese. Titles and abstracts were screened for relevance, focusing on systematic reviews and original studies examining bone loss or musculoskeletal symptoms in women with breast cancer. Studies addressing bone metastasis were excluded.
The review identified 3 key mechanisms: (1) estrogen regulation, highlighting its suppression during endocrine therapy as a primary driver of bone loss and joint pain, which guided the selection of women receiving endocrine therapy for breast cancer as the target population 20 ; (2) exercise physiology, showing resistance and impact exercises as effective in enhancing bone density and joint function by improving mechanical loading and muscle strength 21 ; and (3) calcium and vitamin D, identified as essential for bone mineralization and musculoskeletal function, form the foundational components of the program. 22 Based on these biological mechanisms, we further examined patients’ needs, synthesized evidence-based practices, and selected behavior change theories to address challenges faced by this patient population.
Phase 1.2: Identifying patients’ needs
To align biological mechanisms with patient-centered priorities, we conducted qualitative interviews to identify and characterize the needs of women with breast cancer. This ensured the intervention program was participant-centered and tailored to patients’ needs, characteristics, and cultural preferences. 23
Semi-structured, in-depth interviews were conducted with 13 patients experiencing treatment-induced musculoskeletal symptoms, averaging 49 minutes. Participants were recruited via convenience sampling from WeChat groups and a tertiary hospital. The interviews explored participants’ bone health needs, including their experiences seeking help, the support or information they had received, and their unmet needs for managing bone health. The data collection and analysis methods followed the same approach described in Phase 2. Five themes emerged regarding patients’ bone health needs: (1) exercise instruction, (2) guidance on bone health supplementation, (3) dietary guidance, (4) medication instructions, and (5) symptom relief modalities. The interview outline and patients’ quotations are shown in Supplemental Material. These findings highlighted the strong demand among women with breast cancer for a comprehensive, multicomponent bone health intervention.
Phase 1.3: Identifying evidence-based practices
To guide the design and implementation of the interventions, we conducted a best evidence summary to identify existing evidence-based practices. This synthesis focused on interventions aligned with biological mechanisms and patients’ needs, providing a foundation for selecting and applying specific strategies.
We systematically searched guideline networks, databases, and related Web sites for appropriate studies, which we then screened and assessed. After extracting, synthesizing, and grading the results of the studies, 24 evidence-based practices were generated on bone safety assessment, lifestyle modification, bone health supplements, exercise interventions, drug interventions, and pain management. 24 This informed the design of specific intervention content, format, and dosage. For example, lifestyle modification includes bone health dietary patterns and strategies to promote daily physical activity; the section on bone health supplements covers the dosage and precautions for calcium and vitamin D supplements.
Phase 1.4: Applying behavior change theories
To facilitate the program’s implementation and improve participants’ adherence, we adopted Social Cognitive Theory and Self-Regulation Theory.25,26 The core constructs of Social Cognitive Theory—knowledge of health risks and benefits, self-efficacy, outcome expectations, health goals, and perceived facilitators and barriers—have been proven effective in establishing motivation and confidence for health behavior change.25,27 Self-Regulation Theory, which emphasizes behavior change through self-monitoring, self-evaluation, and self-reaction, particularly applies to personalized exercise interventions.26,28 These theories guided the integration of evidence-based practices and the refinement of intervention details. For example, we addressed bone health risks and benefits in health education sessions. During exercise interventions, we set achievable goals, used sports wristbands for self-monitoring, and analyzed facilitators and barriers regularly. Furthermore, we adopted strategies like group discussions and experience sharing to enhance patients’ self-efficacy and foster positive self-responses to bone health behaviors.
Phase 1.5: Modeling the ROSE program
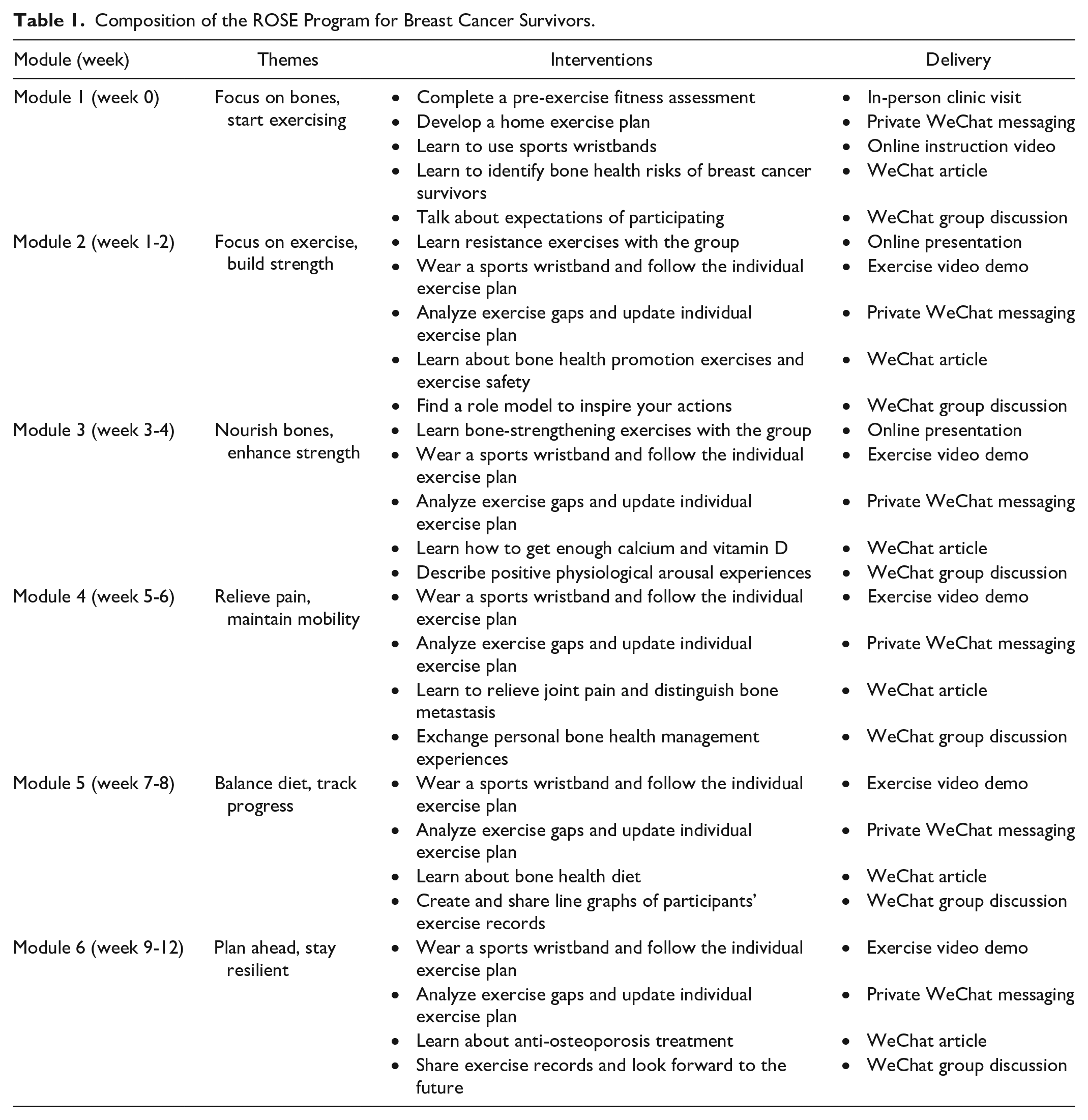
A preliminary version of the ROSE program was developed based on the findings from the previous steps, which included a 12-week progressive exercise plan, health education, and strategies to promote behavior change. We then invited a breast physician, an orthopedic surgeon, a sports medicine physician, 2 registered nurses specializing in breast oncology and orthopedics, and 2 breast cancer patients to participate in 2 rounds of review evaluating the program’s safety, feasibility, and applicability. Based on their feedback, we refined the program and finalized its content and delivery, as well as a standardized 12-week progressive exercise plan template (Table 1 and Figure 2).
Composition of the ROSE Program for Breast Cancer Survivors.
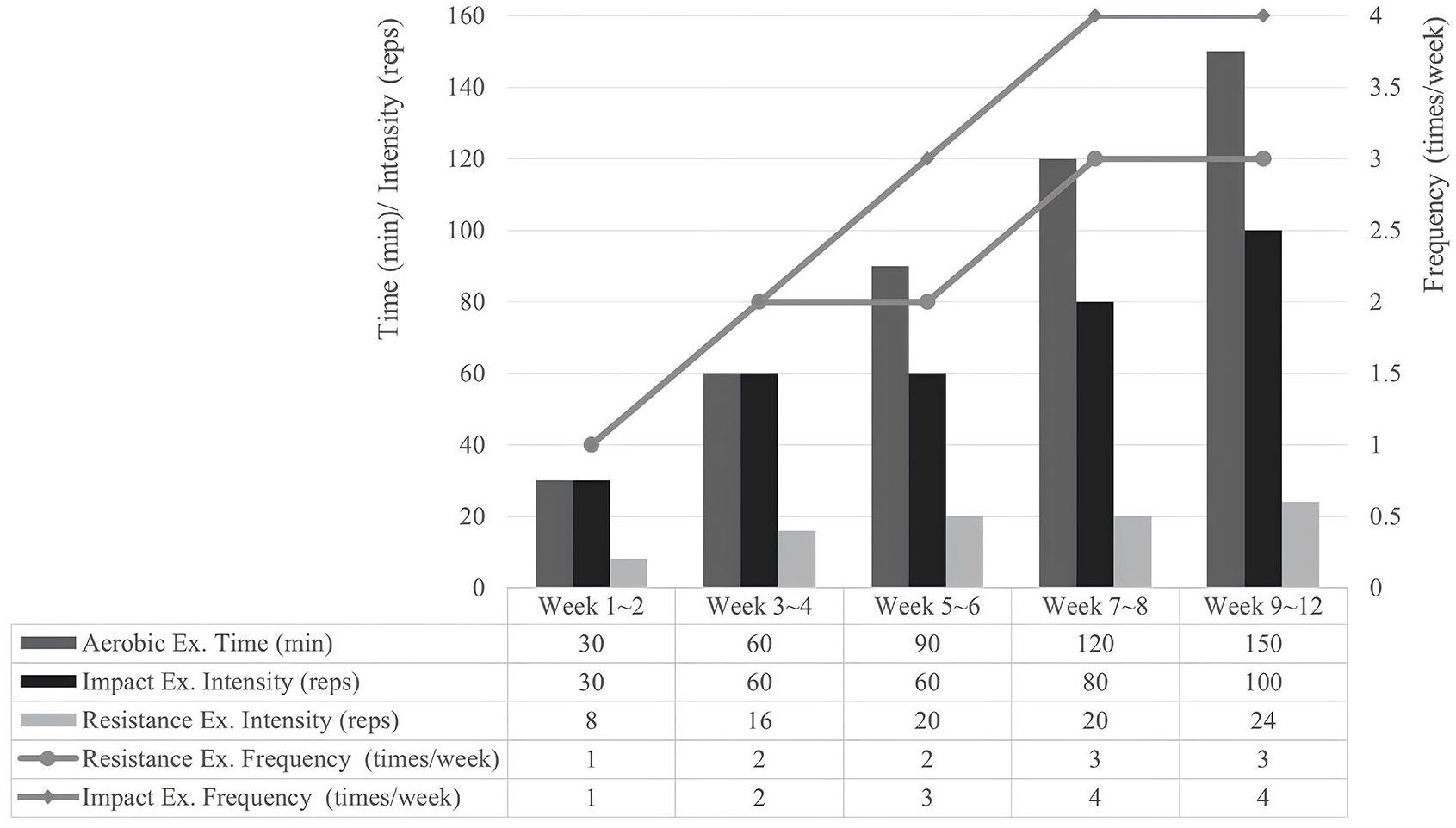
Standardized 12-week progressive exercise plan template.
Phase 2: Acceptability Assessment Phase
Design and participants
To test the program’s acceptability, we conducted a single-arm open-pilot study at the breast oncology clinics in a tertiary care hospital between December 2021 and March 2022. We approached patients during their routine visits. Women aged 18 to 65 years were eligible for this study if they were diagnosed with breast cancer (stages I-III), were undergoing endocrine therapy, were proficient in social media use, and had provided signed informed consent. Then, the 12-week ROSE program was delivered to enrolled participants. Implementation details are presented in the Results section.
Measures
Acceptability was assessed through recruitment rate, retention rate, adherence, a questionnaire, and semi-structured interviews. Sociodemographic information and preliminary outcomes were also collected solely to test the feasibility and acceptability of the data collection procedures.
The recruitment rate was calculated as the percentage of contacted participants who were successfully recruited into the study. The retention rate represented the percentage of participants who completed the study. The exercise adherence rate was calculated as the percentage of weeks each participant met the plan requirements, with data primarily collected from Lifesense sports wristbands and supplemented by weekly follow-ups for any missing data. The group exercise adherence was calculated based on attendance at these sessions. Health education adherence was measured through every WeChat article view record.
A satisfaction questionnaire was designed by our research team and consisted of 8 items: (1) This intervention is clearly targeted; (2) The content of this intervention is easy to understand; (3) I’m interested in this intervention; (4) This intervention works for me; (5) This intervention met my needs; (6) I am satisfied with this intervention; (7) I am willing to accept this intervention; (8) I would like to recommend this intervention to other patients. Each item was scored from 1 (strongly disagree) to 5 (strongly agree). A higher score indicated better satisfaction with the ROSE program.
The semi-structured interviews were conducted after the program. The interview outline, developed based on a similar study, 29 included 12 questions designed to elicit discussion about (1) preferences and suggestions for the program (eg, “Are you satisfied with the project? Which part appealed most to you? What was your least favorite part?”); (2) perceived changes (eg, “What impact has participating in this intervention had on you?”); and (3) barriers and facilitators for program completion (eg, “What made it easier or harder for you to complete all the tasks?”).
Data analysis
Quantitative data were analyzed using descriptive statistics, including means, standard deviations (SD), frequencies, and percentages. Data were managed using the SPSS analytic software (version 26.0; IBM Corp, Armonk, NY, USA). The qualitative data were analyzed using Colaizzi’s method of analysis. 30 Audio recordings were transcribed verbatim and uploaded into MAXQDA Analytics Pro 2020 for coding and analysis. Two researchers (LC and YW) independently coded the data, identifying units of meaning, assigning initial codes, and organizing codes into categories. These categories were then grouped into themes. Discrepancies in coding were resolved through discussion in team meetings, ensuring consensus, and reliability in the analysis. All authors reviewed the final themes and organizational structure to confirm consistency and validity.
Results
The ROSE Program
The 12-week ROSE program consisted of 6 modules, each centered on a specific theme and delivered over a 2-week period. Each module integrated exercise intervention, health education, and behavior change strategies tailored to the module’s theme (Table 1). All interventions were delivered online via WeChat (a messaging and social media app) and Tencent Meeting (a video conferencing platform).
Exercise intervention
The exercise intervention was implemented by a researcher trained through a 20-hour exercise course, with the support of Lifesense sports wristbands (MAMBO5). Participants used the wristbands daily, which provided real-time heart rate feedback to help them adjust their exercise intensity during workouts. Additionally, the wristbands automatically uploaded participants’ physical activity data (ie, exercise type, duration, frequency, and intensity) to a complementary Lifesense app. The app synchronized these data with a researcher-accessible terminal, enabling both participants and researchers to review and monitor progress.
The intervention comprised both group and individual exercise sessions. Group exercises, offered only in modules 2 and 3, focused on teaching participants the movements necessary for their exercise plans. In these individual sessions, patients were required to complete their weekly exercise plans independently. The plan included aerobic, resistance, and impact exercises tailored to individual preferences and capabilities. Aerobic exercises, such as jogging, brisk walking, swimming, or bicycling, were performed at moderate intensity (40%-60% reserve heart rate), gradually increasing to at least 150 min/week, with intensity monitored using the Borg scale and sports wristbands. Resistance exercises consisted of 8 functional movements (ie, forearm abduction, hip adduction and abduction, hip anteflexion and retroflection, glute bridge, scissor kick, and superman) performed with body weight or a 15-lb resistance band, with intensity adjusted by repetitions and sets. Impact exercises, customized to participants’ abilities, progressed from heel bouncing to jumping, with volume and frequency increasing over time.
The initial exercise plan was developed based on a pre-designed exercise progression template (Figure 2) and tailored to each participant’s fitness assessment results. Researchers reviewed and analyzed participants’ exercise data weekly, providing feedback and support to guide their progress. Every 2 weeks, the plan was updated collaboratively, with adjustments to intensity, repetitions, or sets to ensure gradual progression.
Health education
Researchers sent health education articles to all participants, aligning with each module’s themes. These articles covered topics such as risk identification and mitigation, exercise and safety, calcium and vitamin D supplementation, pain management, diet and nutrition, and medication instructions. Researchers monitored participants’ reading records and followed them to ensure they comprehended the educational content.
Behavior change strategies
Researchers organized group activities within the WeChat group for each module to facilitate behavior change. These activities included (1) discussing expectations for participating in the program; (2) sharing role models that inspire action; (3) exchanging bone health self-management experiences; (4) describing positive physiological arousal during exercise (eg, enjoyable music, scenic views, or personal achievements); (5) reviewing individual exercise trends; and (6) discussing future plans.
Program Acceptability
Enrollment and retention
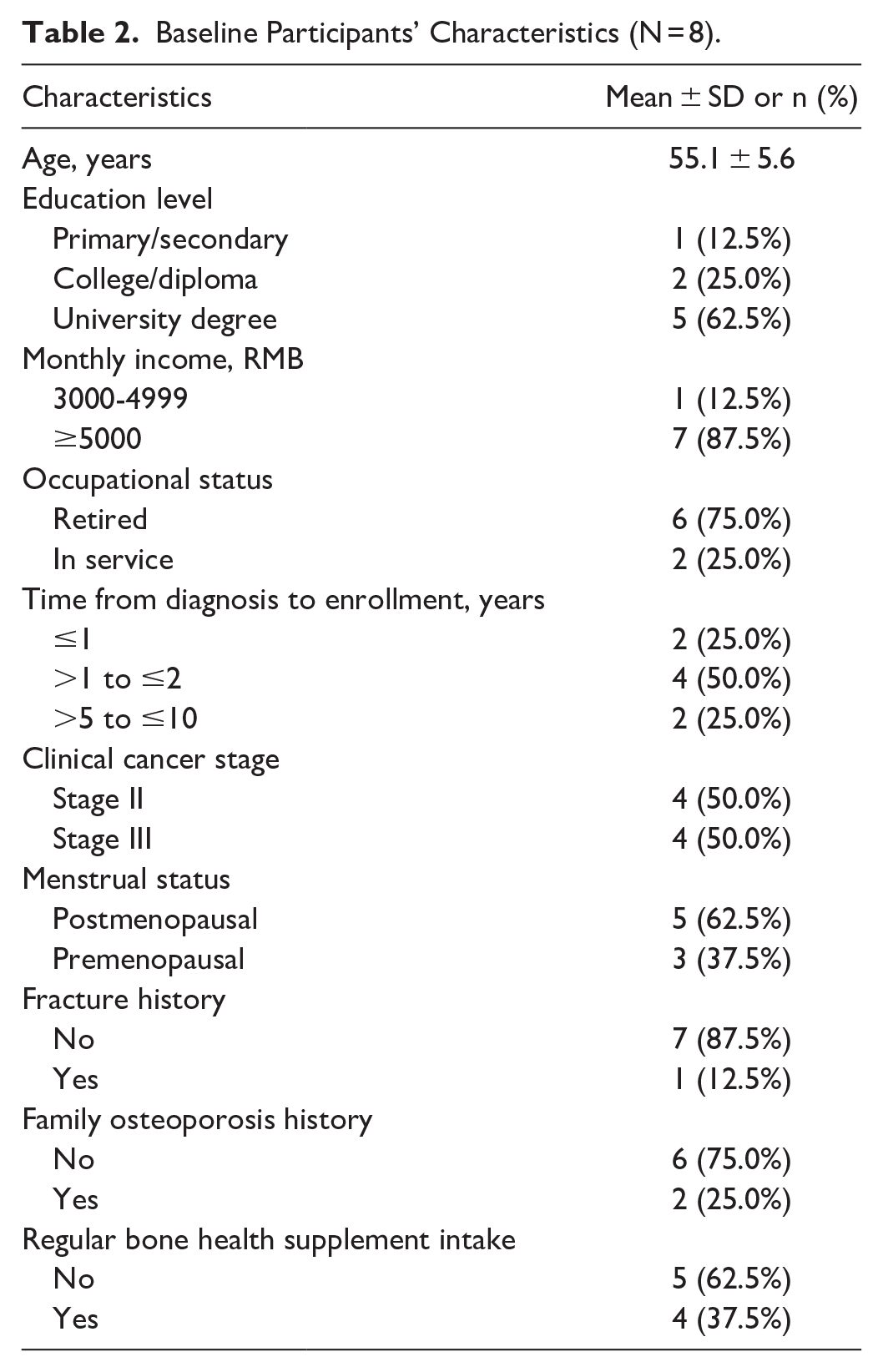
We approached 20 patients, among whom 12 were excluded and 8 (40%) women enrolled in the program. Three did not meet the inclusion criteria, and 9 declined participation due to long distance (n = 2), work demands (n = 4), and lack of interest (n = 3). Patient characteristics are provided in Table 2. Among the 8 participants, 1 dropped out near the end of the intervention due to busy housework and missed the post-intervention assessment, resulting in a retention rate of 87.5%.
Baseline Participants’ Characteristics (N = 8).
Adherence
For individual exercise sessions, adherence rates ranged from 75% to 100%, with an average of 92.9%. For group exercise sessions, all participants except one attended both sessions, resulting in an average adherence rate of 87.5%. All participants completed the health education component by reading all WeChat articles.
Satisfaction and feedback
The questionnaires showed that participants were highly satisfied with the ROSE program, with 100% of responses ranging from agree to strongly agree. After the program, 1 participant was not interviewed due to a time conflict; we finally collected feedback from 6 participants who completed the intervention. The mean duration of the interviews was 43 minutes (ranging from 27 to 71 minutes). Four themes emerged from the post-intervention interviews: perceived benefits of participating, facilitators to adherence, barriers to adherence, and suggestions for optimization.
Effects of participating
The most noticeable change felt by participants was an improvement in physical fitness. “I feel that after I exercise my legs with the elastic band, my leg muscles are well-developed and stronger. Now I can run 5 km,” one participant said (ID3, Wu, age 62 years). All participants also mentioned that they adopted a healthier lifestyle during the program. One participant said, “I used to walk as exercise, but now I know I need to exercise with some intensity. Now I make sure to exercise for no less than half an hour every day. Additionally, when I go out, I try to walk as much as possible instead of taking a car” (ID4, Xu, age 59 years). Participants also reported that the program could help them relieve joint pain and provide them with a positive emotional feeling. One said, “I feel that since joining this group, I’ve been in a better mood and more self-confident” (ID 6, Cui, age 48 years).
Facilitators to adherence
The most commonly mentioned facilitators to adherence with the interventions were the interventionist’s instructions and the sports bracelet’s monitoring. One participant said, “I knew exercise was good but didn’t know how to do it. Your guidance and supervision make me exercise” (ID4, Xu, age 59 years). Another participant said, “I used to have no compulsion to exercise, but now because I can see my exercise with this bracelet, I know I have to get to at least 2000 steps per day and I have to reach a certain level of intensity. I wear this bracelet every day; it’s a constant reminder that I must reach the target” (ID1, Dong, age 54 years). Three participants also emphasized the importance of motivation from other people, such as the actions of other participants in the group and inspiring stories of others. Dong (ID1, age 54 years) said, “I have so little self-discipline that I only want to lie down when I get home from work. But when I see everyone in the group exercising consistently, I force myself to move too.” Wu (ID3, age 62 years) said, “I once watched a mini-marathon with a man in his 80s or 90s, and it particularly touched me. Then I thought, I am only 60 years old and can run too.” In addition, the positive changes participants perceived were the most direct facilitators and the available amenities near their home or workplace were also mentioned as objective conditions for maintaining exercise and sun exposure.
Barriers to adherence
Most participants thought the program was easy to comply with. But sometimes participants’ physical conditions would affect their adherence with exercise. One admitted, “My PICC line is still in place, so I did fewer exercises that require raising my arms. And I am afraid that exercise may bring lymphedema” (ID6, Cui, age 48 years). Another participant who had trouble with resistance exercises said, “I have a bad back, and my knees hurt badly, I can’t use the elastic band to do exercise” (ID1, Dong, age 54 years).
Suggestions for optimization
Participants made some suggestions on the content, delivery, and measurements. Two participants hoped to get more dietary guidance; one said “Diet is still one of my confusions. I know that soya products are high in calcium that I should take, but I have high uric acid, so I cannot eat any soya products. If you can give more diet instructions for people like me, that will be great” (ID2, Sun, age 48 years). Participants also wanted more solutions to reduce joint symptoms. One reported, “I feel better now, but my knee hurts when I move it. There seems to be a bone spur. Is there any other way to relieve it?” (ID1, Dong, age 54 years). As for delivery, participants expressed a desire to increase the number of group exercise interventions and have offline demonstrations for more direct instruction: “It would be nice to have offline group exercises to help us correct the wrong movements directly” (ID5, Zhang, age 52 years). Two participants also suggested enlarging the font size of the WeChat articles and using audio or video to promote health education. In the end, some participants felt that there were too many tests and that the balance tests were not accurate; one said, “I’ve had poor balance since I was young and can’t just stand on one leg with my eyes closed” (ID6, Cui, age 48 years).
Discussion
The ROSE program was developed based on patients’ needs, evidence-based practices, theories, and stakeholder consensus, according to a rigorous, systematic development process of the MRC framework. It integrated progressive exercise, bone health education, and behavior change strategies. Evidence suggests that multicomponent exercise interventions that incorporate education and behavior change techniques can increase the knowledge of osteoporosis, improve the initiation and adherence to bone-healthy lifestyles, and lead to better clinical outcomes. 31 Compared to studies that only provided informational support,16,17 this program more effectively addressed the holistic needs of patients in bone health management and maximized participant adherence to bone-healthy lifestyles.
The ROSE program demonstrated reasonable acceptability. The recruitment, retention, and exercise adherence rates were comparable to similar studies.32,33 Most participants completed the intervention without adverse events or health problems, and many expressed interest in continuing or recommending the program to others. These findings highlight the program’s acceptability and appeal to women with breast cancer, suggesting it has the potential for broader application. Participants maintained a largely progressive level of activity over 12 weeks, demonstrating high adherence to the program. The use of sports wristbands and interventionist guidance played a crucial role in fostering adherence by enabling self-regulation, real-time monitoring, and timely feedback. These tools, combined with group discussions and peer support, were highlighted in interviews as key motivators. Similar strategies have been effective in other cancer recovery interventions, 34 reinforcing their value for exercise-based programs. However, individual concerns about physical limitations, such as knee osteoarthritis or lymphedema, impacted participation for some patients. This suggests that we should further tailor the intervention to patients’ concerns about exercise safety and increase supervision during exercise interventions.
Patient feedback highlighted the program’s ability to promote bone-healthy lifestyles, alleviate joint pain, and improve physical fitness and emotional well-being. The suggestions provided by participants have already informed program refinements. For example, 2 new group exercise sessions were added: “pain relief exercises” for targeted joint symptom management and “outdoor walking” to foster peer support and communication. Health education content was also revised to address the needs of specific populations, such as those with high uric acid or lactose intolerance, while interactive online lectures with playback options were introduced to improve accessibility. Lastly, the evaluation process was streamlined to reduce participant burden by focusing on the most relevant and reflective metrics of bone health.
Limitations
This study had certain limitations. One is its small sample size. Due to the exploratory nature of this research, the small sample size was suitable for evaluating the program’s acceptability. However, this may restrict the depth of feedback gathered from participants. Another limitation is that we did not assess participants’ baseline physical activity levels or self-management behaviors, nor did we implement strict exclusion criteria to control for these factors. As this study was an initial acceptability test, our primary goal was to include a diverse range of participants to gather comprehensive feedback. However, the lack of baseline assessments and the broad inclusion criteria may have introduced variability in participants’ engagement and outcomes. Future studies should include baseline assessments and apply more stringent inclusion and exclusion criteria to enhance comparability and provide more consistent insights into the program’s effectiveness.
Conclusion
We developed the ROSE program based on the MRC framework, which integrated exercise intervention, health education, and behavior change strategies. The ROSE program is acceptable and potentially relieves musculoskeletal symptoms in women with breast cancer. Further research is worthwhile after refining the intervention program on this basis.
Supplemental Material
sj-pdf-1-wjn-10.1177_01939459251331793 – Supplemental material for Development and Acceptability of a Rebuilding Osteo Strength With Exercise (ROSE) Program for Women With Breast Cancer
Supplemental material, sj-pdf-1-wjn-10.1177_01939459251331793 for Development and Acceptability of a Rebuilding Osteo Strength With Exercise (ROSE) Program for Women With Breast Cancer by Lu Chen, Ying Wang, Fuyun Zhao, Pengjuan Song, Juan Liu, Liu Sun, Jiagui Liang, Jun-E Liu and Teresa Hagan Thomas in Western Journal of Nursing Research
Footnotes
Acknowledgements
The authors thank the patients who participated in the study and the tertiary hospitals for their participation and cooperation. Funding from the Beijing Natural Science Foundation is gratefully acknowledged as well. Additionally, the authors extend their gratitude to Lynne Sunderman, a tutor at the University of Pittsburgh Writing Center, for her meticulous line-by-line revisions of the article.
Author Contributions
All authors were involved in the study.
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Data Availability
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Beijing Natural Science Foundation (grant number 7222008).
Ethical Considerations
The Institutional Review Board of Capital Medical University (Beijing, China) approved the study protocol (No. 2021SY122) covering all study phases. The study is also registered with the Chinese Clinical Trial Registry (ChiCTR2300072208), which specifically pertains to the interventional component of the research. All study procedures complied with institutional ethical standards for human subject research and the principles outlined in the Helsinki Declaration.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.