
Abstract
Background:
Parents of a child with autism spectrum disorder (ASD) often continue providing care for their children across the lifespan until they are no longer able, which can cause caregiver burden and affect their quality of life (QOL). To date, most of the research focuses on parents of young children with ASD, with only a small body of research on older parents of adults with ASD.
Objective:
The purpose of this study was to determine whether perceived caregiver health, QOL, availability of informal support, and number of formal supports differed by 3 levels of caregiver burden.
Methods:
A total of 320 older parents (age ≥50 years) of adults with ASD participated in this cross-sectional survey research study that used multiple analysis of variance (MANOVA) to understand the challenges of caregivers when compared by the perceived levels of caregiver burden.
Results:
MANOVA indicated that better health, positive QOL, more availability of informal support, and use of fewer formal supports were associated with lower levels of caregiver burden (F8,614 = 18.48, P < .001,
Conclusion:
Given that high caregiver burden was associated with lower caregiver health, QOL, decreased availability of informal support, and greater use of formal supports, nurses and other health professionals should be cognizant that older parents need specialized attention.
Keywords
Autism spectrum disorder (ASD) is a neurodevelopmental disorder characterized by social communication impairments and restricted, repetitive behaviors. 1 Treatment options include a range of pharmacologic and nonpharmacologic interventions, including behavioral interventions focused on the core symptoms of ASD. 2 Parent-mediated interventions are gaining traction due to their ability to build on the natural parent-child interaction and occur in a naturalistic setting, as well as their feasibility and sustainability. 3 Parents of children with ASD can face increases in caregiver responsibilities as their children transition from childhood to adulthood.4,5 To date, most research on caregivers of individuals with ASD has focused on caring for children instead of adults with ASD;6,7 thus, more research is needed on caregiver burden in families of adults with ASD.
Given the lack of exploration on caregiver burden among parents of adults with ASD, this study focuses on this specific population. To set the stage, the purpose of this study was to determine whether caregivers’ perceptions of health, quality of life (QOL), availability of informal social support, and number of formal social supports used differed by 3 levels of caregiver burden (high, moderate, and low). This research study specifically focused on caregiver burden, social support (both informal and formal), QOL, and caregiver health. Information pertaining to each of these variables is described in each of the respective paragraphs below.
Caregiver Burden in Caregivers of Individuals With ASD
Parenting children with ASD has been associated with caregiver stress, mental health challenges, and high levels of burden.8,9 Caregiver burden is the perceived negative impact resulting from caregiving demands. 10 In this study, caregiver burden of older parents of adults with ASD was conceptualized to consist of 4 domains: time dependence, developmental, emotional, and financial burden.10,11 The time dependence domain is the extent to which burden results from time restrictions placed on caregivers that contribute to missing time with family and friends along with restricted time for career and leisure activities. 11 The developmental domain refers to parents’ feelings of being “off-time” in personal development compared with their peers of the same-age.11(p800) Parents report feelings of social disconnectedness and missing out on a normal way of life. 12 The emotional domain refers to types of emotions parents experience (eg, anxiety, depression, and grief).13,14 Parents of individuals with ASD often report feelings of anxiety and depression.15,16 The financial burden domain refers to the economic costs associated with ensuring the family has access to health care, educational, and career opportunities. Caregiving demands often require parents to reduce hours worked, decline promotions, and forego or delay higher education pursuits.17,18 High rates of caregiver burden are seen in caregivers of children, adolescents, and adults with ASD. 19
Caregiver Burden and Social Support
One factor associated with caregiver burden levels is formal and informal social support.20,21 Formal social support consists of paid or fee-for-service support from professionals (eg, physicians, social workers), governments, community groups, and nonprofit organizations. Although formal social support can be helpful at decreasing stress for parents, it can also be a source of stress. 22 In one study on families of children with ASD, nearly half of participants did not feel respected by health care professionals. 23 Additionally, navigating formal support and accessing each available service could be another source of stress.24,25 Informal social support typically includes unpaid social support provided by family and close friends. 21 Informal support is important in early childhood for parents’ well-being, with this form of social support remaining important across the lifespan.26 -28 In a longitudinal study, Schiltz et al found that caregivers of adolescents and young adults with ASD and other developmental disabilities rated family support as the most helpful, used, and valued source of support compared with formal support and other forms of informal support. 27 Further identifying how informal and formal support relate to caregiver burden perceived by older parents could help to shed light on social support interventions for this population.
Caregiver Burden, Social Support, and QOL
Another factor associated with caregiver burden levels is QOL of the parents. QOL is “an individual’s perception of their position in life in context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns.”29(p1405) In a study comparing parents of children with ASD to a control group, parents of children with ASD had significantly lower QOL scores. 30 In another study that examined predictors of QOL of caregivers of adults with ASD, Sonido et al 31 found that high caregiver burden was a predictor of reduced QOL. Interestingly, they also examined social support and found that formal social support did not predict QOL, but caregiver satisfaction with informal support and size of the support circle predicted QOL. Given the limited evidence on the relationship between these variables for aging families, there is a need to continue to study these relationships, which could inform best practices to support older caregivers of adults with ASD.
Caregiver Health and Influence on Caregiver Burden
Caregivers, particularly as they age, can experience normative and nonnormative health changes and declines that have an adverse impact on their health and well-being. 32 There is a gradual deterioration of the immune system that happens to people as they age, called immunosenescence, that usually starts at age 55 and can have a negative impact on one’s health.33,34 Long-term stress from providing care can worsen these changes and can negatively impact one’s health over time. 35 Parents of adults with ASD might have health problems like high blood pressure, diabetes, heart disease, cognitive decline, and mobility issues.36,37 Parents of children with ASD often report that they feel overwhelmed, and previous research has found that these caregivers can experience health issues connected to stress. 38 Family caregivers often have time constraints and emotional and physical demands from their caregiving role that cause the caregiver to overlook their own health. In addition to this, caregivers of adults with ASD often face challenges accessing programs to support their loved ones and their own needs, which may play a role in the existence of health issues among caregivers. 39 It has been found that caregiver burden is predicted by health issues. For example, in a study by Chen et al, caregivers of older adults with disabilities with better perceptions of health had lower levels of caregiver burden. 40
Theoretical Framework
The stress process model, used as a framework for this study, examines how stressors influence health outcomes. 41 The model includes 3 elements of stress: sources (eg, chronic stressors), outcomes (eg, mental health), and mediators (eg, social support, coping skills). The theory posits that a primary objective stressor has an impact on the caregiver’s life. For example, a primary stressor of caring for an adult with ASD could negatively impact the caregiver’s life by increasing their stress levels, decreasing their mental and physical health, and reducing their QOL. Social support could act as a mechanism to reduce these negative outcomes.
Purpose
To date, the majority of research on caregivers of persons with ASD focuses on caregivers of young children with ASD, with only a small body of research on older parents of adult children with ASD.6,7 The lack of research in this area is concerning as the predominance of individuals with ASD are in adulthood 42 and typically supported in some capacity by their aging parents. 43 To begin to address the gap of research in understanding, the purpose of this study was to determine whether older parents’ perceptions of health, QOL, and informal and formal social support varied by 3 levels of caregiver burden (high, moderate, and low). The hypotheses for this study are as follows:
H1: Caregivers’ health will not be associated with their perceptions of burden associated with providing care for their adult child with ASD.
H2: QOL will not vary relative to caregivers’ perceptions of burden associated with providing care for their adult child with ASD.
H3: Caregivers’ perceptions of the availability of informal support will differ relative to the level of caregiver burden associated with providing care for their adult child with ASD.
H4: The use of formal support will vary relative to caregiver burden associated with providing care for their adult child with ASD.
Methods
Research Design
A nonexperimental cross-sectional design was used to determine whether older parents (age ≥50 years) of adults with ASD differ in terms of their self-reported health, levels of QOL, and formal and informal supports relative to their level of caregiver burden. In this study, parents’ composite burden scores were divided into thirds at the 33rd and 67th percentiles to form 3 groups: high (n = 108), moderate (n = 107), and low (n = 103). Previous research has grouped caregiver burden in a similar manner to test for differences in sleep quality. 44 These groupings were used to compare the scores for caregiver health, QOL, number of formal social supports, and perceptions of availability of informal social support.
Recruitment
The principal investigator (PI) used organization networks, support groups, professional contacts, word-of-mouth, and snowball sampling to recruit a sample of convenience comprising older parents of adults with ASD. Distribution of study materials, such as the study flyers and links, were assisted by organizations and groups (eg, state autism organizations, regional autism organizations) that serve adults with intellectual and/or developmental disorders (eg, ASD) and their family caregivers. To share study information with its affiliates, material was disseminated via newsletters, e-mails, and posting on organization Web sites. The locations of all organizations were in the United States. The PI reached out to professional networks and provided study details at local events and face-to-face support groups. Consent was obtained prior to participants completing the online survey. The first page of the survey included an information sheet with all components of the informed consent form. Participants agreeing with the information sheet indicated their consent to participate. After consenting, participants could complete the online survey on the Qualtrics platform. Given the diverse methods of survey dissemination coupled with recruitment efforts, it was not possible to compute a survey response rate, which is based on knowing how many people received the survey.
Participants were not asked to include their names when completing the survey to protect their anonymity. In addition, study data and information were secured on a password-protected computer. At the end of the survey, participants had the option to elect to be included in a drawing for one of the three $25 gift cards. Gift cards were distributed to participants whose names were drawn that had indicated interest in the raffle and had provided contact information. Contact information obtained was destroyed following the drawing of raffle winners.
Participants
The survey responses were screened to ensure participants met the inclusion and exclusion criteria for the study. To be included in the study, participants had to be a parent of an adult child (aged ≥18 years) with ASD, 50 years of age or older, and able to read and understand English. Internet access was needed to complete the online survey. The minimum caregiver age of 50 years was chosen as an inclusion criterion because the focus of this research was to understand the challenges faced by older parents of adults with ASD. This age was intentionally chosen as it coincides with the minimum age that the American Association of Retired Persons targets. 45
Of the 353 downloaded surveys, 10 participants failed to meet the inclusion criteria, and 23 participants were eliminated because the surveys were not completed adequately. After the removal of the disqualified cases, a total sample of 320 participants remained.
Instruments
The survey used in this study consisted of a researcher-developed tool to gather participant demographics and the number of formal social supports. Several different response formats were employed, including forced-choice, fill-in-the-blank, and multiple responses. The survey also contained scales from the World Health Organization’s Quality of Life-BREF (WHOQOL-BREF) to measure caregiver QOL and self-reported caregiver health; ENRICHD Social Support Instrument (ESSI) to measure informal social support; the Caregiver Burden Inventory (CBI) to measure 3 domains of burden (time dependence burden, developmental, and emotional); and the Caregiver Reaction Assessment (CRA) to measure financial burden. The survey was pilot-tested for content validity and revised based on professional feedback before it was used for data collection in this study. Participants had the option to add explanations to any questions for which there was no preset response that fit their situation. If they chose to not answer any question, they could leave the response blank. The participants were informed that all responses were private and confidential and that no specific person could be identified in the final report.
Sociodemographic variables
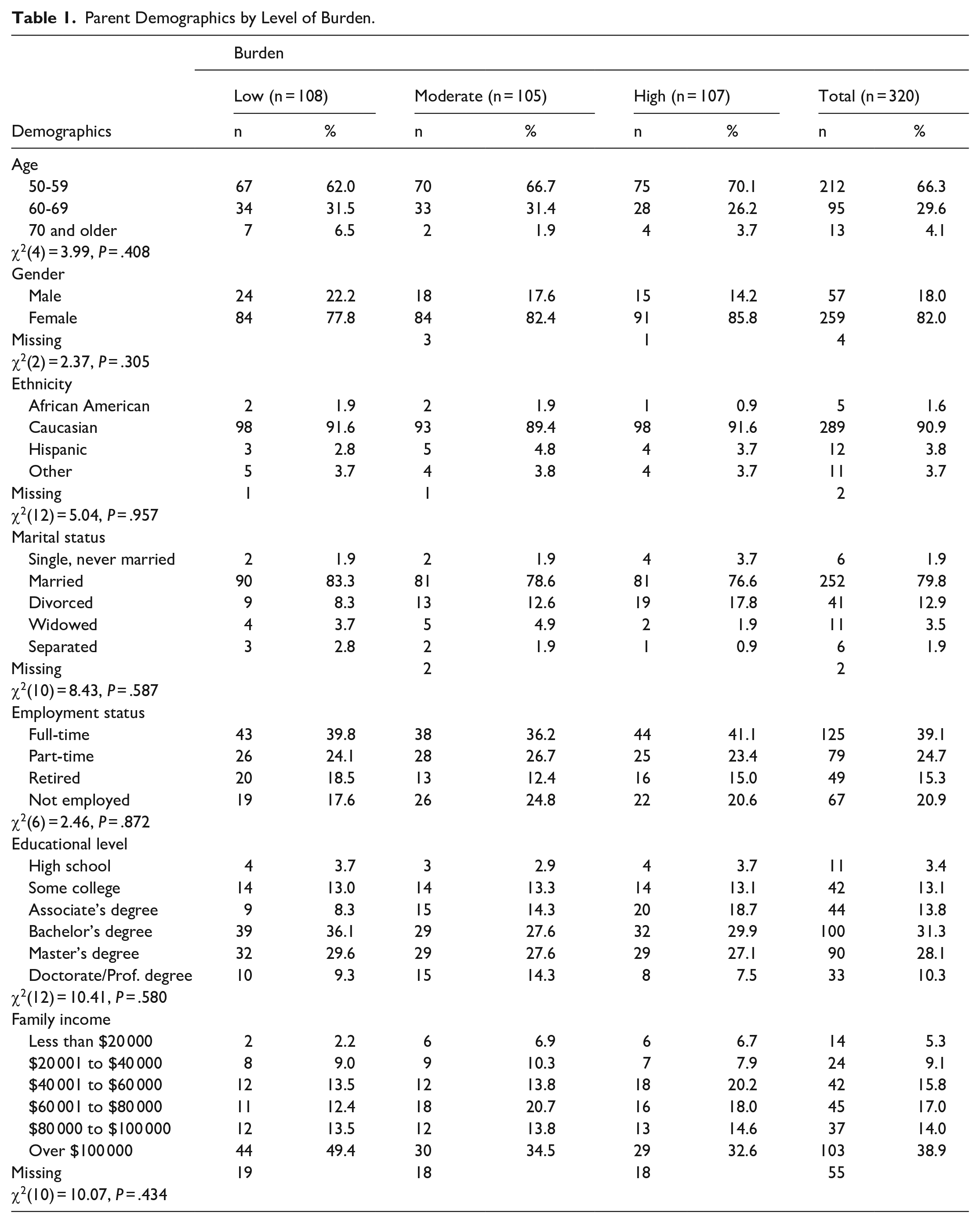
Data on annual family income and age of the respondents and the adult children with ASD were gathered using ordinal scales with prefixed categories as summarized in Table 1. In addition, sex (ie, male, female), race and ethnicity (ie, African American/black, American Indian/Alaskan Native, Hispanic, Middle Eastern, multiethnic, white, other), marital status (ie, married, divorced, widowed), employment status (ie, full-time, part time, retired), and educational level (eg, high school, some college, associate’s degree) were measured at the nominal level from questions included in the survey’s demographic portion.
Parent Demographics by Level of Burden.
Quality of life
The 6 items of the WHOQOL-BREF’s psychological well-being subscale were used to measure caregiver QOL in this study. 46 Each of these items was rated on a 5-point ordinal scale, with “1” indicating poor attitude and “5” positive attitude toward their caregiving roles. One of the 6 items was reverse-coded before creating a mean score that reflected the direction of the original 5-point scale, where higher scores indicate better QOL. Past research with family caregivers of individuals with developmental disabilities, including autism spectrum disorders, indicates that the WHOQOL-BREF possesses good reliability and validity.47,48 The standardized Cronbach alpha coefficient of 0.86 for the current sample indicated that the QOL tool used in this study had good internal consistency as an indicator of reliability.
Caregiver health
Caregivers self-reported their health status using a single-item question from the WHOQOL-BREF 46 that asked study participants, “Would you say your health is: excellent = 1, very good = 2, good = 3, fair = 4, poor = 5.” The scores on this 5-point ordinal scale were reverse-coded so that higher scores indicated better health.
Informal social support
The availability of informal social support from caregivers’ networks (such as family and friends) was assessed using 6 questions from the ESSI. 49 The ESSI was originally developed to measure the social support available for individuals recovering from cardiovascular conditions. 49 After reviewing the extant literature for valid and reliable tools to measure informal social support, the PI identified the ESSI to be relevant to determine the availability of informal caregiving help. The items were measured using a 5-point ordinal scale (1 = none of the time to 5 = all of the time) to quantify parents’ perceptions of the availability of informal support. Participants were asked to rate the 6 items such as “Is there someone available to whom you can count on to listen to you when you need to talk?” and “Can you count on anyone to provide you with emotional support (talking over problems or helping you make a difficult decision)?” Past research shows that the ESSI possesses the sensitivity to be used to measure the availability of informal social support of parents of children with autism.26,27 The ESSI’s strong internal consistency as a measure of reliability is indicated by the obtained Cronbach alpha coefficient of 0.85 for the current investigation.
Formal social support
A researcher-developed 15-item checklist was used to ask participants whether they had ever used formal social support services (ie, respite care, social work, psychiatric services). The checklist included different social supports used by caregivers for themselves or their adult child with ASD. The 15 included options were obtained from an extensive review of the literature,50 -54 clinical experiences of the PI, and professional feedback. Participants could indicate “yes” or “no” for each type of support and another service received that was not listed by typing in text. Depending on the number of social supports selected by the caregivers, the formal social support scale’s ratings could range from 0 to 15.
Caregiver burden
Caregiver burden was assessed using 3 CBI subscales (time dependence burden, developmental burden, and emotional burden) and the financial subscale from the CRA.10,11 Specifically, composite caregiver burden was computed using an 18-item scale with 15 CBI items and 3 CRA items. Both the CBI and the CRA were originally designed for caregivers of aging adults with individuals with Alzheimer’s disease and other chronic conditions; 55 however, there is ample evidence that both of these tools have been used with other caregiver populations, including parents of children with ASD.56,57 Each of the items in both scales were measured on 5-point ordinal scales, where higher scores indicate greater burden. Each CBI item was measured using the following response categories: 1 = never, 2 = rarely, 3 = sometimes, 4 = quite frequently, 5 = nearly always, which was similar to the original CBI response scale that used 0 to 4 ratings to represent “never” to “nearly always” in the same direction, where higher scores indicated greater burden. Similarly, each CRA item was measured using a 5-point Likert scale: 1 = strongly disagree, 2 = disagree, 3 = neither agree nor disagree, 4 = agree, 5 = strongly agree, where higher scores represented higher burden after reverse-coding one of the CRA items. Examples of items include “He/she needs my help to perform many daily tasks” (time dependence burden), “I feel that I am missing out on life” (developmental burden), “I feel angry about my interactions with him/her” (emotional burden), and “It is difficult to pay for my adult child with ASD” (financial burden).
Past research indicates that both the CBI and the CRA possess excellent internal consistency and validity when used with diverse caregivers.11,58 -61 The Cronbach α coefficients as indicators of internal consistency for the burden subscales in this study were as follows: α = 0.91 for the 5-item time dependence burden subscale, α = 0.91 for the 5-item developmental burden subscale, α = 0.88 for the 5-item emotional burden subscale, and α = 0.87 for the 3-item financial burden subscale. The composite caregiver burden scale was created by summing the ratings and then dividing by 18 (total number of subscale items) to obtain a mean score. The Cronbach α coefficient for this composite burden scale for the current sample was 0.91 (based on standardized items). These Cronbach α values indicate that the burden scales used in this study possessed strong internal consistency as an indicator of reliability.
Data Analysis
IBM SPSS version 29 (IBM Corp, Armonk, NY, USA) was used to analyze the data. As part of the data cleaning process, 33 completed surveys were deleted due to missing information (23 had less than 50% of the survey completed) or eligibility criteria (1 was a sibling caregiver, 9 were parents below the age of 50). Missing values analysis indicated that the percent of missing values of the key variables examined ranged from 0% to 1.6%. The highest number of missing values was for financial burden (n = 5, 1.6%), followed by QOL and informal social support (n = 3, 0.9%); time dependence, emotional, and developmental burden (n = 0.3%), with no missing values for formal social supports. Based on these results, we limited analyses to cases with valid responses in all questions.
The data were checked to assure that all assumptions associated with correlation analysis and multivariate analysis of variance (MANOVA) had been met. A correlation matrix was completed to determine the extent to which the variables were related (Table 2). As the assumptions were met, a MANOVA procedure was used to determine whether differences existed in caregiver health, QOL, and informal and formal social support by degree of caregiver burden reported by the participants. An a priori power analysis using the G*Power 3.1 software (Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany) was conducted to determine the minimal sample size required for a MANOVA with 3 categories and 4 dependent variables. Results indicated that a sample size of 57 was required to obtain a power of 0.80, with an effect size of 0.15, and an alpha level of .05. Further, group differences were identified using Scheffé’s post hoc tests of all possible pairwise comparisons. All decisions on the significance of the findings were made using a criterion alpha level of .05.
Correlation Matrix of Variables of Interest.
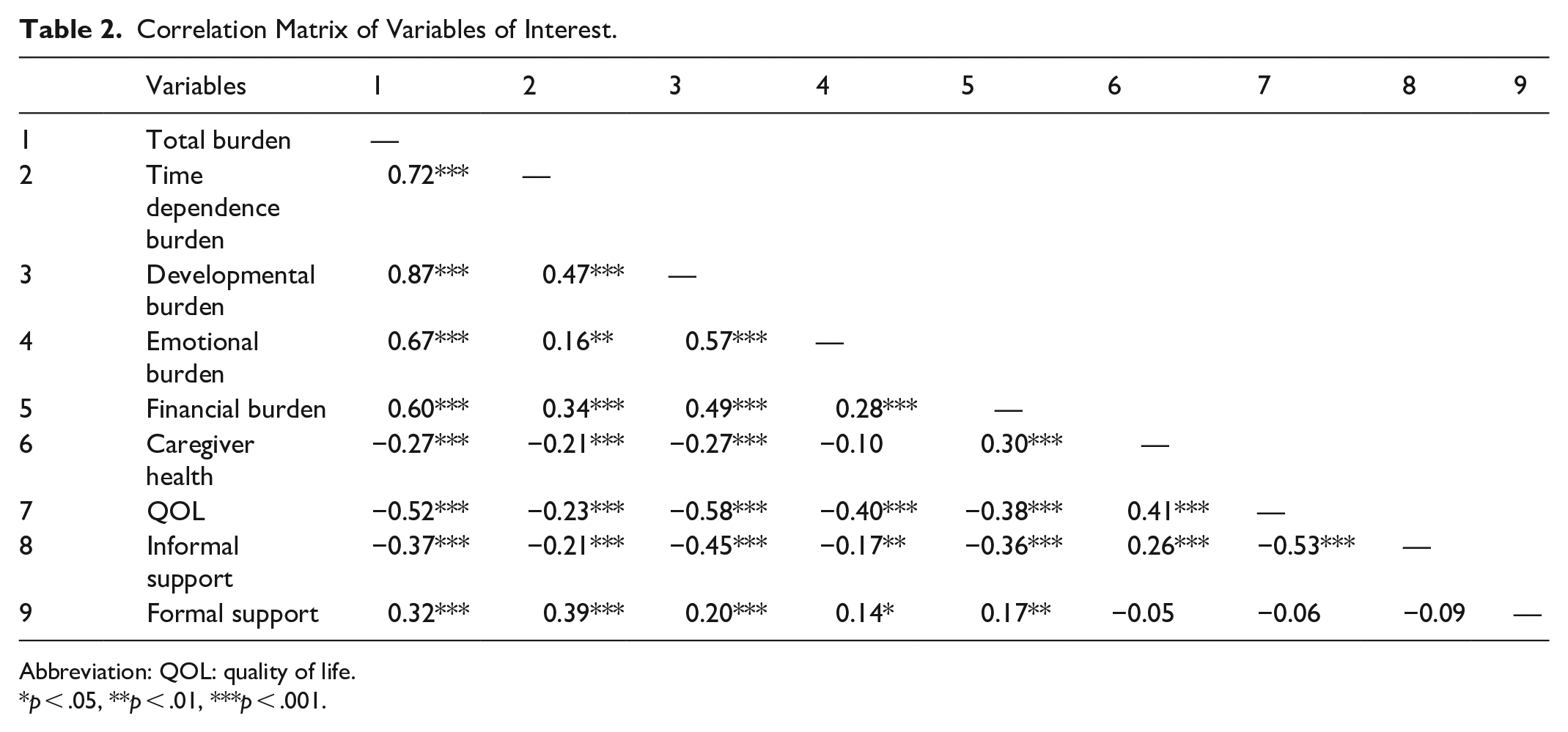
Abbreviation: QOL: quality of life.
p < .05, **p < .01, ***p < .001.
Results
Table 1 summarizes the participant characteristics as indicated in the demographic part of the survey. Most participants were female (n = 259, 80.9%) and between the ages of 50 and 59 years of age and married. The race identified by the majority of mothers and fathers was white. Most of the participants indicated completion of at least a bachelor’s degree and had family incomes that exceeded $80 000 annually. The results of chi-squared tests for independence provided support that demographic characteristics did not differ by the level of burden.
Table 2 provides a summary of the bivariate intercorrelation matrix created to determine the relationships between the variables of interest. Total burden was significantly associated with the 4 domains of burden. The strongest correlation was with developmental burden (r = 0.87, P < .001), followed by time dependence burden (r = 0.72, P < .001), emotional burden (r = 0.67, P < .001), and financial burden (r = 0.60, P < .001). Total burden was negatively correlated with QOL (r = −0.52, P < .001), informal social support (r = −0.37, P < .001), and caregiver health (r = −0.27, P < .001). A statistically significant positive correlation was found between total burden and the number of formal social supports used (r = 0.32, P ≤ .001).
A one-way MANOVA was used to determine whether the 4 dependent variables (caregiver health, QOL, availability of informal support, and number of formal supports used) differed by level of caregiver burden. Caregiver burden was divided into 3 groups (high, moderate, and low) using a three-way split at the 33rd and 66th percentiles. The valid cases included in this analysis were 103 (high burden), 103 (moderate burden), and 107 (low burden). The results of the MANOVA were statistically significant (F8,614 = 18.48, P < .001, partial eta-squared
Multivariate Analysis of Variance: Comparing Levels of Burden.
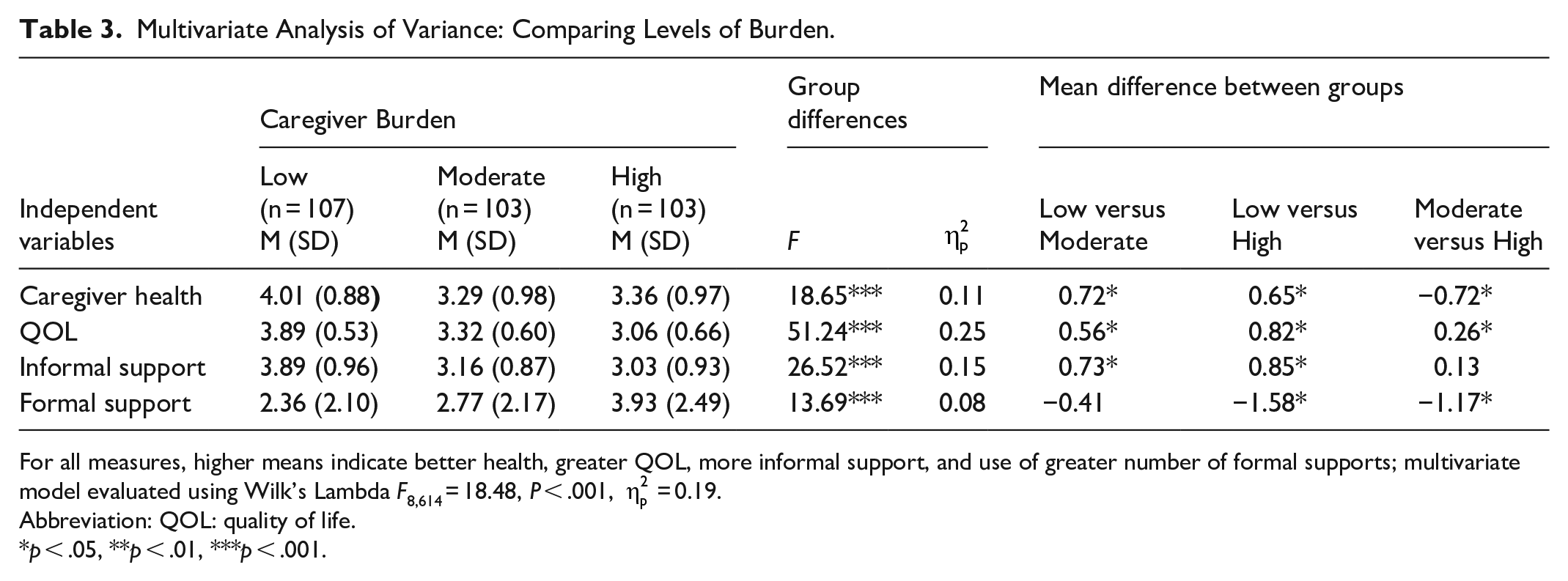
For all measures, higher means indicate better health, greater QOL, more informal support, and use of greater number of formal supports; multivariate model evaluated using Wilk’s Lambda F8,614 = 18.48, P < .001,
Abbreviation: QOL: quality of life.
p < .05, **p < .01, ***p < .001.
The ANOVA model comparing caregiver health by the level of caregiver burden was statistically significant (F2,310 = 18.65, P < .001,
The ANOVA model comparing QOL of caregivers by the level of caregiver burden was also statistically significant (F2,310 = 51.24, P < .001,
The ANOVA model comparing the perceived availability of informal supports by levels of burden was also statistically significant (F2,310 = 26.52, P < .001,
A statistically significant difference was found when the number of social supports used by parents was compared by levels of caregiver burden (F2,310 = 13.69, P < .001,
Discussion
The purpose of this study was to determine whether perceived caregiver health, QOL, availability of informal support, and number of formal supports vary among older parents who experience different (high, moderate, and low) levels of caregiver burden. The findings supported the hypothesis that better health, more positive QOL, availability of informal support, and the use of fewer formal supports were associated with lower levels of caregiver burden. Additionally, the study adds further insight into the health of older parents of adults with ASD, filling a gap in research in this population.6,7
As one might expect, parents with lower caregiver burden tended to self-report better health. These findings are intuitive and aligned with previous published literature indicating negative impact on parents’ health resulting from caregiving demands.62 -65 The scores for QOL using a 5-point scale ranging from strongly disagree (1) to strongly agree (5) ranged from 3.00 to 3.89 for the 3 groups, indicating that none of the participants had extreme scores of very low or very high QOL. Scores for availability of informal social support ranged from 3.00 to 4.00, indicating that most participants perceived the availability of moderate levels of informal support. The number of formal social supports used by the older parents in caring for the adult with ASD ranged from 2 to nearly 4. As many types of formal social support were available, the expectation was that their parents would be using more than was reported.
QOL includes perceptions of an individual’s position in life within their culture and value systems that are related to their aims, expectations, standards, and concerns. 29 Parental QOL can be affected by the severity of the adult child’s ASD, strength of the informal social support system, parental health, and the burden associated with caregiving. 66 The finding that QOL differed among the 3 levels of caregiver burden was not unexpected. However, the extent of differences among the 3 levels indicated that the greater the burden, the more likely the QOL of the caregiver would be negatively impacted. Sonido and colleagues found similar results with high caregiver burden associated with reduced QOL. 31 In a scoping review of QOL interventions for primary caregivers of children with ASD, Fewster et al found that interventions that focused on how caregivers could care for themselves, such as by learning stress management strategies and setting goals, are beneficial at improving QOL. 67 Although this scoping review focused on children with ASD instead of adults, similar interventions could be tested in adult caregivers of individuals with ASD.
The finding that greater availability of informal social support is associated with low burden appears intuitive and follows logic that parents who have a robust informal support network typically have lower levels of caregiver burden. Past research indicates that lower levels of informal social support was associated with high caregiver burden among caregivers of young children, adolescents, and adults with ASD.68 -70 These findings align with previous research, which demonstrated that caregivers with more nurturing informal social support networks reported lower levels of caregiver burden. 31 Interestingly, even interventions aimed at educating caregivers and offering formal support could help to increase informal support and could be a potential avenue to explore in future research. 68 Interventions could be targeted at improving access to meaningful informal social support networks to benefit parental caregivers of adults with ASD.
Parents who were using a higher number of formal social supports reported higher levels of caregiver burden. The number of formal social supports used could be related to other factors, such as the severity of symptoms of ASD exhibited by the adult child. A study identified trajectories of perceived negative impact (eg, caregiver burden) related to parents of individuals with ASD from childhood through emerging adulthood. 8 They found that parents reported restricted, repetitive, and externalizing behaviors were associated with higher caregiver burden. Individuals with ASD with these behavioral manifestations could require more formal support. In another study on mechanisms of formal and informal social support in parents of children with ASD, Shepherd et al discussed a similar idea whereby symptom severity could influence the need for, or access to, formal social supports. 71
Practice Implications
Older parents of adults with ASD who report high levels of burden also reported poor health. More attention should be devoted to enhancing the physical and mental health of aging parents of adults with ASD. These parents are noted to be a health disparate population, warranting continued attention and focus to support them in their daily caregiving roles and general life. 72 Because of the interconnection between adult children with ASD and their parental caregivers, better caregiver health equates to more effective care for their care recipients. 63 Nursing and other health care professionals should be cognizant of the toll on their personal health that caregivers may face due to the ongoing demands of caregiving over time. Attention and support should be directed to assist parents in focusing on their own physical and psychological health needs. Future research should investigate the needs and effectiveness of interventions to support caregiver health.
Given that QOL was poorer among those with high caregiver burden, professionals should be cognizant that these caregivers need specialized attention to reduce the demands associated with caregiving. Special attention should be paid to caregivers who convey characteristics of high caregiver burden, as well as those at risk of having high caregiver burden. Caregiver burden is perception based, and the cognitive appraisal of burden is important. Providers should develop awareness to assess the level and extent of caregiver burden based on what is tacitly inferred or explicitly stated by caregivers, as well as personal characteristics (eg, behavioral symptomatology, care needs, severity of ASD and other co-occurring conditions, level of caregiving supports). Nurses and other health professionals should work with all caregivers, particularly those at risk of high caregiver burden, to put support in place to alleviate the caregiving demands when possible. Based on previous findings, when appropriate support is received, caregivers have demonstrated improved QOL. 69
Although there was a positive association between formal supports and caregiver burden, the inverse association of informal supports with caregiver burden implies that interventions targeted at improving informal support networks can be beneficial for parents. Given the many years that parents can expect to care for their child with ASD, parents should be encouraged to ask for and receive help from family, friends, and neighbors willing to lend a helping hand. The positive association between formal support and burden is mostly due to it being related to other factors such as the severity of disability of the care recipient. Therefore, nurses and other health professionals working with aging parents should encourage the development of informal support networks through their families, neighborhoods, communities, and faith-based organizations. As people age, informal social support networks typically change due to several factors. Efforts should be made to help families develop and use informal social support networks without draining and exhausting these networks.
Limitations
Despite the merit of this study, some limitations should be considered. Participant recruitment relied heavily on recruiting individuals connected with organizations and/or support groups. Parental caregivers who lacked stable access to the internet may likely have been excluded from the current study. Given this recruitment strategy, individuals who were not connected with such organizations and groups or those who lacked internet access may have been excluded from the present study. The sample is relatively homogeneous, comprised mainly of participants who identify as being white, female, and having higher educational and family income levels. The sample was recruited to include individuals across the United States. Data on participants’ geographical location was not collected, nor does this study include information for those living in other countries; thus, the sample may lack generalizability. Another limitation is the use of self-report, which may contribute to participants answering in socially desirable ways. Future research should seek to recruit a more heterogeneous sample, reflecting the diversity in caregiver composition across the United States. As the current sample was primarily female, efforts should be made to include more fathers in future studies. Additionally, the data were collected at one point in time, so a cause-and-effect relationship cannot be confirmed. A longitudinal study could provide information on the changes in caregiver burden as the parental caregiver and care recipient progress across the lifespan.
Conclusions
Older parents of adults with ASD who experienced more burden were more likely to report worse health and QOL, with significant differences in all 3 burden groups. Older parents who had more informal social support available to them reported lower levels of burden, although there was no difference between those who reported moderate and high burden. Older parents who were using more formal social support reported higher levels of caregiver burden, although there were no differences between those who reported low and moderate burden. In summary, high caregiver burden was associated with poor caregiver health, poor QOL, decreased availability of informal support, and greater use of formal supports. Nurses and other health professionals should be cognizant of the support needs of older parents of adults with ASD. More research and professional attention should be devoted to aging families of adults with autism.
Footnotes
Acknowledgements
None.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
Approval to complete this research study was granted to the principal investigator by Wayne State University’s Institutional Review Board (IRB # 012615B3X) before starting this study. Participants provided electronic informed consent at the start of the online survey.