
Abstract
Background:
Sleep is an important determinant of health and well-being. Poor sleep among nurses is associated with medical errors, poor decision-making, and decreased patient safety. National research priorities have underscored the need to understand the impact of nursing job characteristics on sleep health and mitigation strategies.
Objective:
We aimed to test whether sleep hygiene behaviors moderated the association between job characteristics and sleep health among nurses.
Methods:
A cross-sectional analysis was conducted on data from the Nurses’ Health Study 3 (N = 1272). Logistic regression analysis tested the modifying effect of sleep hygiene behaviors when examining the association between job characteristics and sleep health among nurses practicing in various care settings and specialties.
Results:
Sleep hygiene behaviors were associated with increased odds of healthy sleep on workdays and work-free days; however, sleep hygiene did not moderate associations between job characteristics and sleep health. Working 12-hour or longer shifts was not associated with decreased odds of healthy sleep compared with working <12-hour shifts on workdays or work-free days. Working in schools and critical care was associated with 50% or higher odds of unhealthy sleep compared with working in the operating room and oncology on work-free days.
Discussion:
Findings suggest sleep hygiene behaviors cannot fully mitigate the effect of job characteristics on sleep health. Study results indicate sleep health may vary by nursing care setting and specialties. Future research should consider factors that may impact sleep health such as short staffing, commuting during work, and time off between shifts.
An estimated 70 million adults in the United States suffer from poor sleep health, manifesting in inadequate sleep duration, poor quality sleep, irregularity in sleep timing, and daytime sleepiness. 1 Poor sleep is associated with hypertension, diabetes, obesity, and poorer cognitive, emotional, and social functioning. Sleep health is of particular importance in the nursing workforce because inadequate and poor quality sleep is associated with fatigue and daytime impairments (eg, sleepiness, reduced attention, vigilance, poor decision-making)2-4 that in turn result in decreased work productivity, increased medical errors, workplace injuries, and poor patient safety.5,6 Prior studies in nursing show that job factors such as shift work, exposure to blue light, long work hours, and short staffing contribute to poor sleep health.6-9 Sleep hygiene strategies such as blocking blue light waveforms before bed and dim light at bedtime have shown some promise in improving the disrupted sleep-wake cycle associated with shift work in nurses.7,9 However, it is unknown whether enacting these sleep hygiene behaviors fully mitigates the adverse impacts of nursing job characteristics associated with poor sleep health. 9
Poor Sleep Health Among Nurses
Sleep is an important determinant of overall health and is required to support well-being and cognition. 10 The negative consequences of poor sleep health are particularly relevant for nurses who spend a considerable amount of time at the bedside and in the community (schools, community clinics). An estimated 58% to 68% of the nursing workforce has poor sleep health; this is concerning given nurses are the largest health care workforce and provide essential health care for individuals, families, and communities.8,11-15 Nursing involves highly specialized skills such as administering medications and treatments, performing medical procedures, and coordinating care and health care services that are demanding and require attention and vigilance to inform good decision-making and safe quality care.5,15 Moreover, shift work, long work hours, and short staffing are common in nursing and contribute to poor well-being, decreased delivery of safe and effective nursing care, and poor sleep health.5,6,16 Several studies among nurses report inadequate sleep duration and poor quality sleep lead to increased fatigue, impaired cognition, and poor decision-making when providing nursing care.2,3,5,17
Inadequate sleep duration, poor quality sleep, irregular sleep timing, and daytime sleepiness is a public health and nursing workforce concern given the associations with increased medical errors, poor patient outcomes, workplace injuries, job turnover, nursing shortages, and rising health care costs.2,3,5,17
Sleep hygiene includes activities and routines prior to sleep and at bedtime; unhealthy activities (eg, media use, caffeine, exercise prior to bed) contribute to inadequate sleep, poor quality sleep, and irregularity in sleep timing. 9 In nursing, shift work and shift length (8, 10, or 12 hours) is common and likely contributes to poor sleep habits that in turn negatively impact sleep duration, quality, and timing of sleep.5,6,15 Prior studies in nurses have shown working longer than 12 h/shift is associated with short sleep duration and poor sleep quality.5,6,9 However, the mechanism of association between extended shift length and poor sleep health is not fully understood. 5 Further, the focus on shift length in the hospital setting does not take into account nurses practicing in other settings such as schools. Current research on improving sleep health among nurses has focused on reducing blue light, individual sleep hygiene behavioral strategies, shifts, naps during work, and schedule modification.7,9,18 Research has not examined the modifying effect of blue light reduction on nursing job characteristics including working long or irregular shifts and its effect on sleep health.5,11 National research priorities have underscored the importance of sleep health and the need to better understand nursing job characteristics including impact on sleep health and effective strategies to improve sleep among the nursing workforce.5,11
Purpose
The purpose of the current study is to examine the association between shift work, shift length, average hours per week, and job setting/specialty among nursing workforces. We hypothesized a high prevalence of poor sleep health, anxiety, and depression in the study population and a negative association between working night shifts and in the hospital setting and sleep health.
Methods
Participants and Study Design
Beginning in 2010, the Nurses’ Health Study 3 (NHS3) started the ongoing recruitment and enrollment of nurses living in the United States or Canada born in 1965 or later. 19 Approximately 40 000 nurses are currently enrolled in the NHS3 study. The NHS3 collects data every 6 months via web-based questionnaires, including one that asks participants to self-report job characteristics, health behaviors, and health indicators. In 2017, the NHS3 questionnaire included questions related to sleep health. Additional information and details about NHS3 are reported elsewhere. 19
Measures
The 5 Dimensions of Sleep Health
Sleep health was measured by self-report and included 5 dimensions: sleep duration, insomnia, timing (chronotype), snoring, and daytime function.
Sleep duration was the average number of hours of sleep over a 24-hour period on workdays and work-free days. Short sleep duration was defined as fewer than 7 hours, adequate sleep as 7 to 9 hours, and prolonged sleep as more than 9 hours 18 based on the joint consensus of the American Academy of Sleep Medicine and the Sleep Research Society. Participants identified as having adequate sleep duration were given a score of 1; all others were scored 0.
Insomnia symptoms were assessed using a validated insomnia rating scale 20 based on frequency of occurrence of the following over the last 4 weeks: (1) trouble falling asleep, (2) waking up at night, (3) waking up earlier than planned, and (4) trouble falling back asleep following early waking. Frequency ranged from 1 to 5 or more times per week. The scores of each of the 4 questions were then summed with a maximum score of 4. Total scores of 3 or 4 were scored as 1, consistent with infrequent insomnia symptoms (ie, healthier sleep); total scores <3 were scored as 0, suggesting frequent insomnia symptoms.
Chronotype was assessed by participants identifying themselves as one of the following: “definitely morning type,” “more of a morning type,” “more of an evening type,” “definitely evening type,” or “neither.” This measure has been validated as a surrogate measure for circadian rhythm. 21 “Definitely a morning type” and “more of a morning type” were scored as 1, indicating a healthier sleep-wake cycle; all others were scored as 0.
Snoring was measured by asking participants to report the average frequency of snoring ranging from “every night” to “almost never.” This measure is a validated predictive measure for detecting sleep apnea. 22 Responses of “almost never” and “occasional” were scored as 1; responses ranging from “a few nights a week” to “every night” were scored as 0.
Daytime dysfunction is a validated subjective measure used to assess the impact of insomnia. The daytime dysfunction question asks participants to rate the impact of not being well rested over the past 4 weeks on the following: fatigue, mood, ability to work, concentration, and memory. 23 Responses are selected from the following 5 options: “not at all,” “a little,” “a moderate amount,” “quite a bit,” and “very much.” Responses of “not at all” and “a little” were scored as 1. Responses of “a moderate amount,” “quite a bit,” and “very much” were scored as 0, indicating more daytime dysfunction.
Total sleep health scores were computed by summing the 5 dimensions of sleep health for a maximum score of 5, with higher scores indicating better sleep. The composite scoring developed by the NHS3 is used to reduce measurement errors and account for interrelatedness among the 5 dimensions of sleep health. 24 Based on the precedent that NHS studies used these sleep measures, which were validated within the nursing population, 24 “healthy sleep” was defined as total sleep scores of 4 or 5, and “intermediate or poor sleep” was defined as scores ≤3.
Sleep Hygiene
Sleep hygiene behaviors were assessed by: (a) regularity of falling asleep with light on, (b) brightness of bedroom ambient light while sleeping, (c) installation of application on electronic device that controls the color of the display to minimize bright light exposure during the night, and (d) electronics use prior to sleep. Answers were scored as 0 or 1, with 1 indicating healthier sleep hygiene behaviors. Falling asleep with a light on 3 or more nights per week9,19 was scored as 1; all others were scored as 0. 8 Bright ambient light during sleep was scored as 0, and instillation of application that minimizes light on electronics 7 was scored as 1. Sleep hygiene behaviors were treated as a count ranging from 0 to 4; scoring a 1 on all sleep hygiene behaviors resulted in a count of 4, suggesting healthy sleep hygiene; scoring a 1 on 3 sleep hygiene behaviors resulted in a count of 3; and a 0 on 1 behavior results in a count of 3, and so forth.
Job Characteristics
Job characteristics included (a) shift type, (b) shift length, (c) average hours worked per week, and (d) nurse type (described below). These categories were selected based on their relevance to sleep health.5,6,9,10,21,25,26
Shift type was assessed by asking participants to select the shifts they worked in the past year: (1) early morning, (2) days, (3) evening, and (4) nights. Participants who selected more than 1 shift type were coded and reported as multiple for shift type. Related to small cell size and unclear parameters, those who answered “early morning” were excluded from the analysis.
Shift length included the average hours worked per month over the last year of each schedule. Shift length in hours was calculated based on shift start time-shift end time in 30-minute increments. Responses were dichotomized as (1) ≥12 hours and (2) <12 h/shift.
Average hours worked per week included the average hours participants worked per week over the last year and were categorized as follows: 0, 1 to 20, 21 to 40, 41 to 60, and >60 h/week. Participants who reported 0 were excluded from the analytical sample. Response categories were collapsed into full-time or less (1-40 h/week) or more than full-time (≥41 h/week).
Nurse specialty/setting asked participants to identify their current primary job and refers to the specialties(s) or setting(s) nurses worked in: (1) emergency room (ER), (2) home health, (3) intensive care unit (ICU), (4) nonhospital, (5) oncology, (6) operating room, (7) other-hospital, (8) other-inpatient, (9) outpatient, and (10) school nurse. Participants who selected more than one of the above were coded as multiple for nurse specialty/setting. Based on a conceptual understanding of nurse practice environments, nurse setting/specialty was collapsed into 7 specialties/areas of practice: (1) outpatient and nonhospital; (2) ICU and ER; (3) oncology and operating room; (4) other inpatient and other hospital; (5) school nurse; (6) multiple nurse roles (eg, ICU and outpatient); and (7) home health.
Demographic Characteristics
Demographic characteristics included age in years at time of survey, race (American Indian or Alaskan Native; White; Black or African American; Asian, Native Hawaiian or other Pacific Islander; Middle Eastern or North African; or multiple races), ethnicity (eg, white non-Hispanic and Latin(0,a)/Hispanic), and gender (eg, female, male, neither male nor female). Participants self-reported clinical diagnoses of anxiety, depression, and sleep apnea as yes or no.
Data Analysis
Participants who answered the NHS3 sleep health questionnaire were included in the analytical sample (N = 1272). Participants with missing responses for any of the independent, dependent, or covariate variables of interest were excluded from the analytical sample. Participants excluded based on missing data were examined for systematic nonresponses and differences in demographic characteristics, and pattern differences were not found.
Percentages and counts were calculated for demographic variables (race, ethnicity, immigration status), health-related diagnosis (anxiety, depression, sleep apnea), job characteristics (shift type and nurse setting/specialty), sleep health, and sleep hygiene. Means and ranges were calculated for age, shift length, and average hours worked in nursing per week. For the logistic regression analysis, the variable race was collapsed to White and non-White (Asian American, Black or African American, multiple races, Native American Indian or Alaskan Native, Native Hawaiian, or other Pacific Islander). Nonresponses and nonconditional missing responses were excluded.
Total Sleep Health Scores were computed by summing the 5 dimensions of sleep health (duration, insomnia, timing [chronotype], snoring, and daytime function) for a maximum score of 5, with higher scores indicating better sleep. The composite scoring developed by the NHS3 is used to reduce measurement errors and account for interrelatedness of the 5 dimensions of sleep health. 24 Healthy sleep was defined as total sleep scores of ≥4 and poor sleep was defined as scores ≤3. 24
Multivariate logistic regression analysis was conducted to estimate odds ratios of a healthy sleep score (≥4) on workdays and work-free days relative to sleep hygiene behaviors and job characteristics among currently-practicing registered nurses. Separate models were used for workdays and work-free days to assess the primary outcome—healthy sleep—for workdays and work-free days.
Final multivariate models for workdays and work-free days included sleep hygiene behaviors and job characteristics: (a) shift type: days, evenings, nights, multiple; (b) shift length: >12 and ≤12 hours; (c) average hours worked per week: ≥41 and 1 to 40 h/week; and (d) nurse setting/specialty: (1) oncology and operating room, (2) outpatient and nonhospital, (3) other inpatient and other hospital, (4) school nurse, (5) ICU and ER, (6) home health, and (7) multiple roles. There were no significant interactions between sleep hygiene behaviors and job characteristics. Accordingly, no interaction terms were included in statistical models.
The workday model included the covariates (eg, gender, race, ethnicity, depression, anxiety) based on scientific and statistical significance.5,10,27 The work-free days model included the following statistically and scientifically relevant covariates: race, age, and medical diagnosis of depression.5,10,27
Results
Sample Characteristics
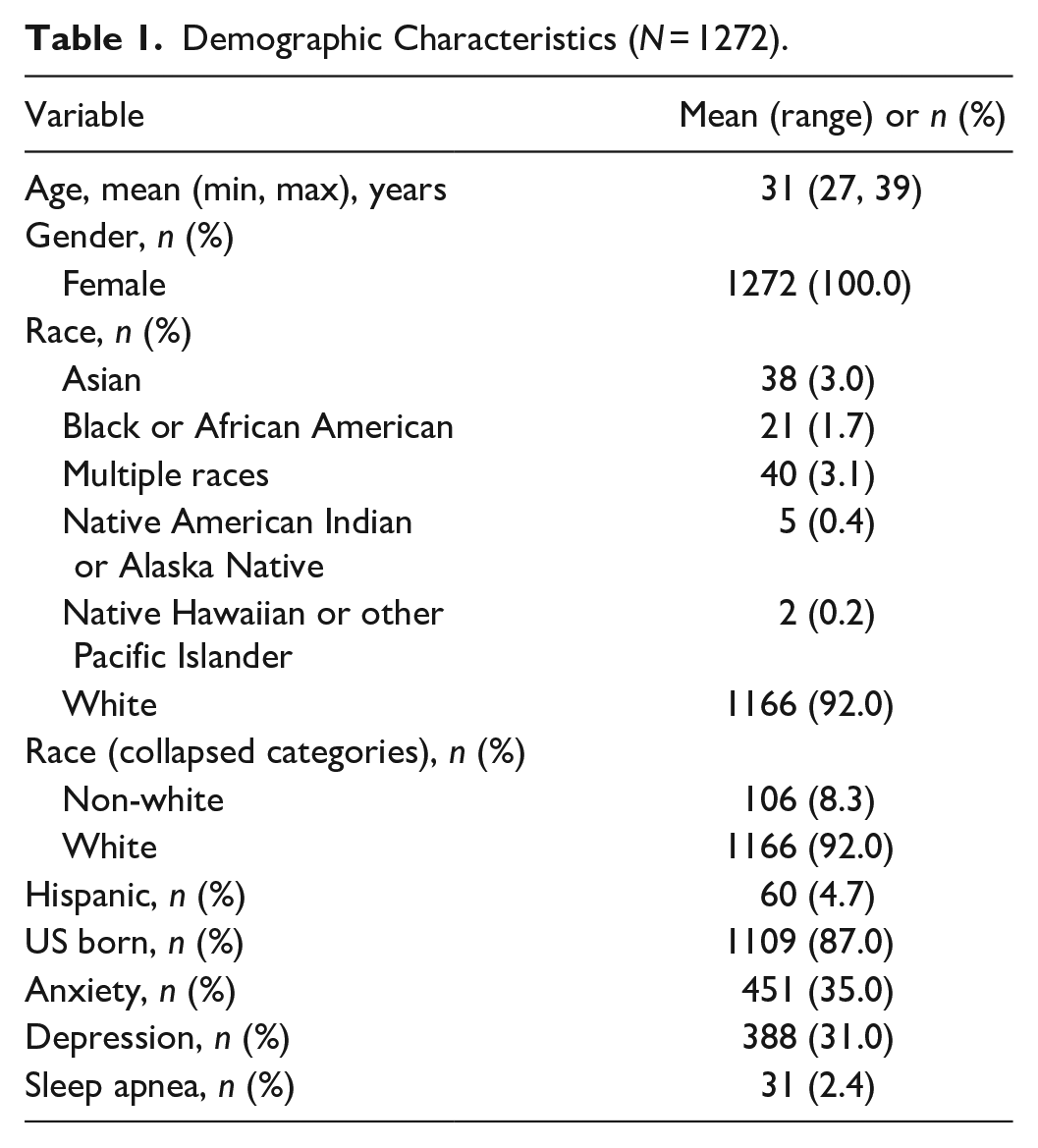
The mean age of the sample was 31 years, 100% were female-identifying, 92% white, and 87% were born in the United States. Participants reported medical diagnoses of anxiety, depression, and sleep apnea at 35%, 31%, and 2.4%, respectively (Table 1). Of the sample, approximately half worked day shift, with mean shift length of 12 hours, and the majority worked on average 21 to 40 h/week and in a hospital setting (Table 2). Nearly half of participants reported healthy sleep on workdays and most reported healthy sleep on work-free days (Table 2). Most participants reported falling asleep with the light off, sleeping with low ambient light, and having a light-blocking application on an electronic device (Table 2).
Demographic Characteristics (N = 1272).
Job Characteristics, Sleep Health, and Sleep Hygiene (N = 1272).
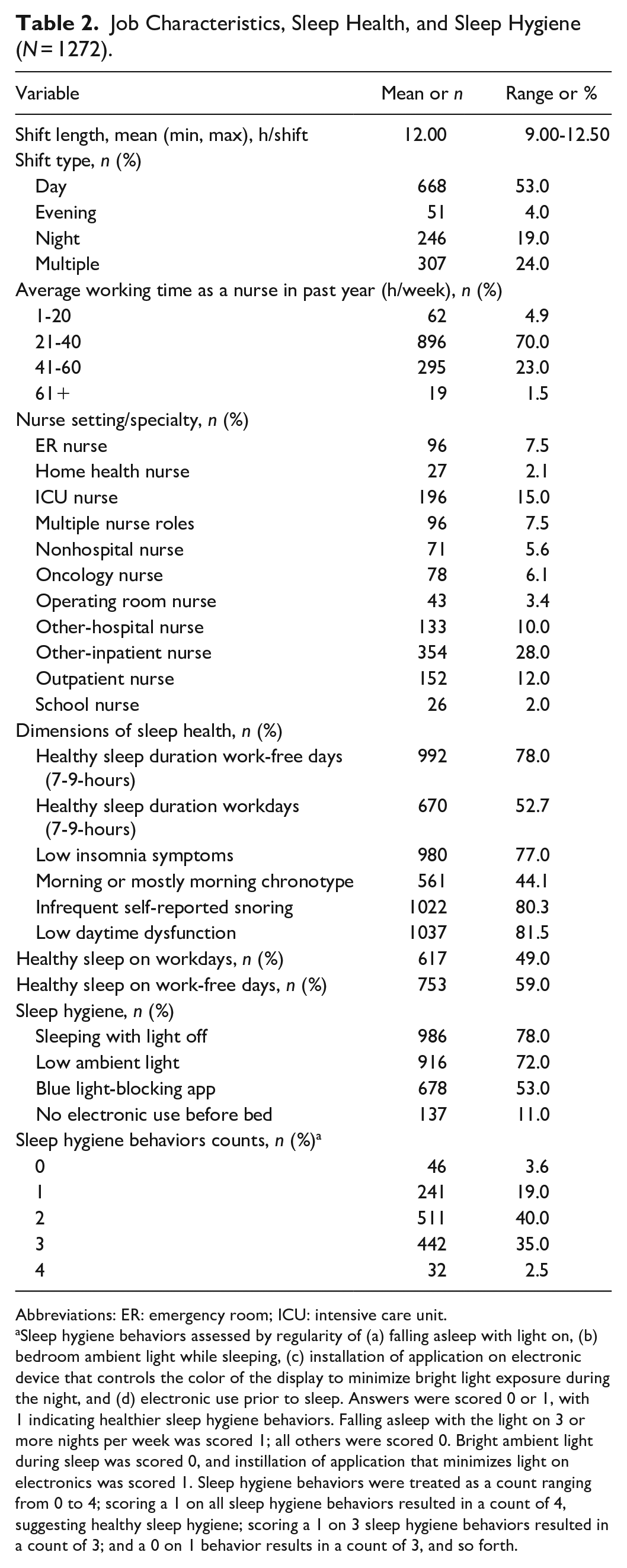
Abbreviations: ER: emergency room; ICU: intensive care unit.
Sleep hygiene behaviors assessed by regularity of (a) falling asleep with light on, (b) bedroom ambient light while sleeping, (c) installation of application on electronic device that controls the color of the display to minimize bright light exposure during the night, and (d) electronic use prior to sleep. Answers were scored 0 or 1, with 1 indicating healthier sleep hygiene behaviors. Falling asleep with the light on 3 or more nights per week was scored 1; all others were scored 0. Bright ambient light during sleep was scored 0, and instillation of application that minimizes light on electronics was scored 1. Sleep hygiene behaviors were treated as a count ranging from 0 to 4; scoring a 1 on all sleep hygiene behaviors resulted in a count of 4, suggesting healthy sleep hygiene; scoring a 1 on 3 sleep hygiene behaviors resulted in a count of 3; and a 0 on 1 behavior results in a count of 3, and so forth.
Sleep Health on Workdays
Table 3 shows the adjusted multivariate model for sleep health on workdays. Sleep hygiene behaviors were associated with increased odds of healthy sleep on workdays while holding shift type, shift length, average hours worked per week, and nurse specialty/setting constant.
Bivariate and Multivariate Logistic Regression Models for Odds of Healthy Sleep (N = 1272).
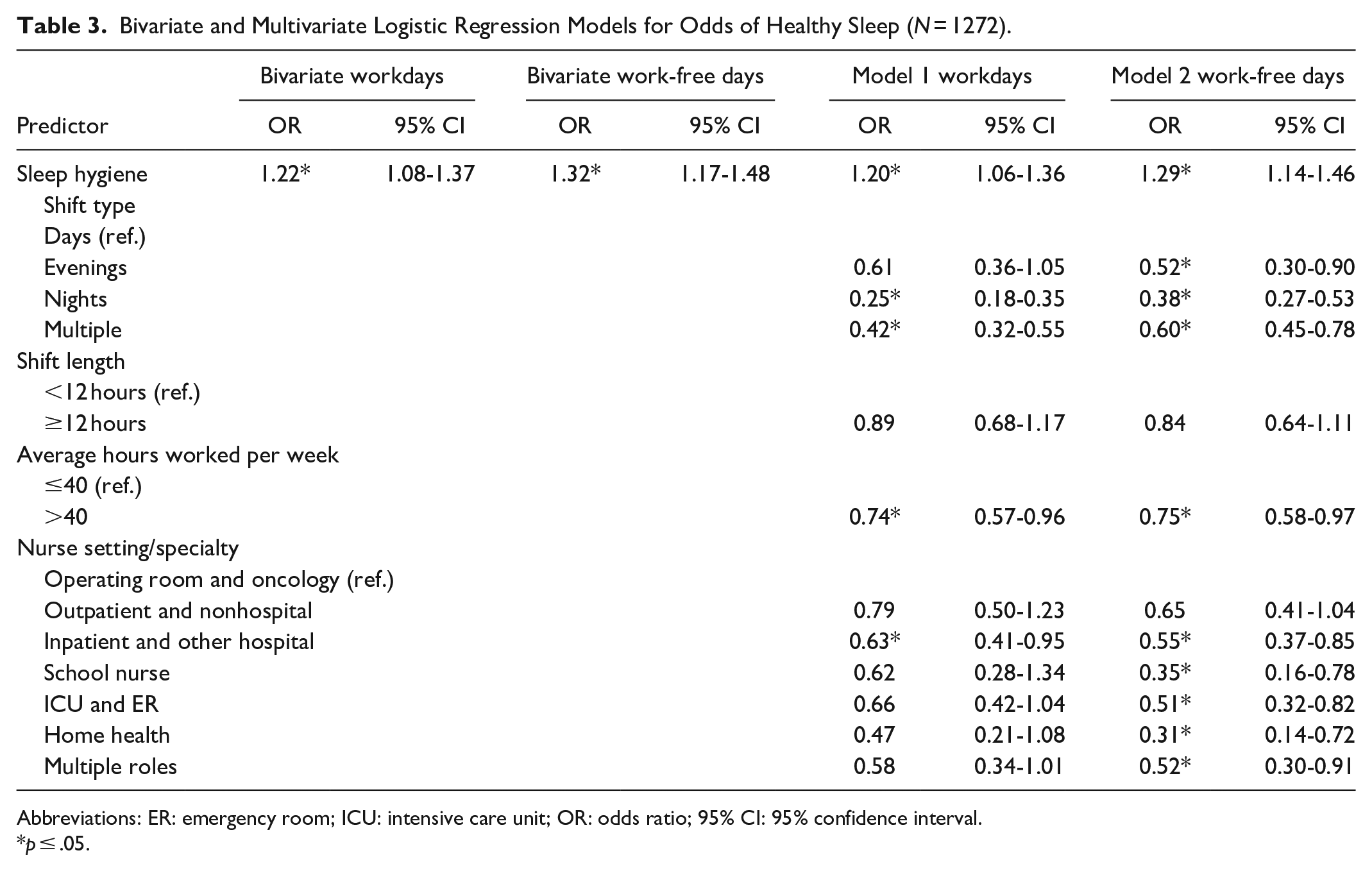
Abbreviations: ER: emergency room; ICU: intensive care unit; OR: odds ratio; 95% CI: 95% confidence interval.
p ≤ .05.
In the adjusted multivariate model for sleep health on workdays, night shift and multiple shifts were both associated with decreased odds of healthy sleep in comparison with those working day shift. Working 12-hour or longer shifts was not associated with decreased odds of healthy sleep in comparison with those working <12-hour shifts. None of the nurse practice settings/specialties other than inpatient or other hospital, were associated with a significantly decreased odds of healthy sleep in comparison with working in the operating room and oncology setting/specialty.
Sleep Health on Work-Free Days
In the adjusted multivariate model for sleep health on workdays (Table 3), sleep hygiene behaviors were associated with increased odds of healthy sleep on workdays while holding shift type, shift length, average hours worked per week, and nurse specialty/setting constant. Working nights and multiple shifts was associated with decreased odds of healthy sleep compared with those working day shift. Working 12-hour or longer shifts was not associated with decreased odds of healthy sleep compared with those working <12-hour shifts. Working as other inpatient or other hospital, ICU/ER, school nurse, home health, and multiple roles were all associated with a statistically significant decrease in the odds of healthy sleep compared with working in the operating room and oncology setting/specialty (referent group) on work-free days. School nurses, ICU, and ER nurses were associated with 50% or higher odds of having unhealthy sleep in comparison with the referent group.
Discussion
Consistent with national estimates, more than half of the sample had poor sleep health scores on workdays and work-free days.8,11,12,16 As expected and consistent with prior studies, falling asleep with the light off, low ambient light while sleeping, installation of an application on an electronic device that controls the color of the display to minimize bright light exposure during the night, and electronic use prior to sleep were positively associated with sleep health on workdays and work-free days.7,9,28 Individual behaviors before initiating sleep, such as limiting light exposure, have been associated with improving sleep health among nurses.7,9,28
There were no statistically significant interactions between sleep hygiene behaviors and job characteristics on sleep health. Our findings suggest that individual sleep hygiene behaviors alone are not effective at mitigating the adverse effect that nursing shift work (working different schedules or shifts or working night shifts) has on sleep health. Our finding differs from prior studies in nurses that report sleep hygiene can mitigate the adverse effects of shift work on nurses’ sleep health.7,9,28 These results suggest that programs and policies aimed at improving sleep health among nurses should not rely on individual-level behavior change alone. Rather, a combination of individual (age, chronic health, mental health, family characteristics) and environmental (home, neighborhood, hospital characteristics) factors need to be studied simultaneously to better understand what work factors can be modified to improve nurses’ health and well-being.
As expected, nurses who worked night shifts reported decreased odds of healthy sleep compared with those who worked day shifts. These findings are consistent with prior studies that report working outside of daylight hours disrupts circadian rhythms and, as a result, sleep health.3,5,6,21 Our finding underscores the critical need for research in the optimization of nursing work schedules that promote sleep health while balancing patient care needs. Strategies such as health organizational policies that promote increased time off in between shifts; consistent work schedule timing; improved staffing to increase support and decrease fatigue; and employee sleep spaces that promote napping for nurses working nights have shown promise. 28
Nurses who work in the hospital setting, schools, and home health all reported decreased odds of healthy sleep on work-free days. These results support that exposure to characteristics of work such as short staffing, commuting during work, and time off between shifts may impact sleep health on work-free days.5,6 The school nurse specialty schedule is characterized by working five 8-h shifts/week during daylight hours. 29 Markedly, the results indicate that school nurses report a higher proportion of healthy sleep on workdays and a lower proportion on work-free days. These results suggest that there may not be adequate time off between nursing shifts to recover from work stressors that adversely impact sleep health. 28 Working multiple shift types was associated with decreased odds of healthy sleep on both workdays and work-free days. Studies in other populations of workers have found that unpredictable and inconsistent work is associated with poor sleep. 30 This was found to be particularly true of female-identifying workers who are primary caregivers for other family members. 30
In contrast to prior studies that show an association between shift length and poor sleep health, we did not find a significant difference in the odds of healthy sleep on workdays or work-free days for nurses working ≥12-hour shifts compared with those working <12-hour shifts. Importantly, nurses have cited 12-hour shifts as optimizing their work-life balance, ability to recover from work stress, and attending to their own medical care needs. Future research is needed to explore the interactions between work schedules, time off, work-life balance, job characteristics, and sleep health among nurses.
On work-free days, nurses who work in the hospital setting, critical care specialties, schools, and home health reported decreased odds of healthy sleep. Some of these specialties do not involve shift work or extended shifts outside of daytime hours, which is typically associated with poor sleep health among nurses. This further supports the idea that shift work alone cannot fully account for poor sleep health among nurses. These findings support an expanded focus that includes characteristics of work such as stress, intensity, role strain, and consistency of shift work, which may have a residual or cumulative effect that adversely impacts sleep health on work-free days.
Limitations
This current study is limited by the cross-sectional design, which cannot account for variation of job characteristics and sleep hygiene behaviors on sleep health. All study measures were self-report, which introduces recall bias. In addition, study measures did not address factors in nursing specialties, such as short staffing that adversely impacts sleep health. Sleep hygiene measures did not account for other behaviors known to influence sleep, such as consistency of times initiating sleep. This validates the need for future research that includes objective measures of job stressors such as staffing support, work schedules, multifaceted sleep hygiene measures, and sleep measurement using technology such as actigraphy. Lastly, the study sample was 100% female-identifying. Gender identity likely influences sleep health, which limits the generalizability of the findings to the larger population including male-identifying and gender-diverse nurses. Future studies will require more inclusive sampling techniques that include outreach to men, nonbinary individuals, and those from other genders not represented in this sample.
Implications
The results from the current study as well as the large body of evidence surrounding sleep health in the general population suggest future programs, policies, and research aimed at improving sleep health among nurses should consider an implementation science approach. This approach would support policymakers, hospitals, and researchers’ engagement of nurses across care settings and specialties as part of the program development, decision-making process, implementation, and evaluation. This method could take into account external factors such as budget constraints and patient care needs to adapt sleep hygiene strategies and work schedules to meet public health needs while promoting a healthy nursing workforce. Such workplace policies would include providing consistent timing of shifts and adequate staffing that supports breaks during shifts and workload handoff at the end of nursing shifts.
Conclusions
The current study describes nursing job characteristics, sleep hygiene behaviors, and their association with sleep health among a national cohort of nurses practicing across distinct care settings and specialties. These study findings provide important insight about the essential need for hospital policies to address and optimize sleep health among nurses, which can then improve job retention and patient outcomes. Nursing workforces are disproportionately negatively impacted by poor sleep health, which can certainly have adverse impacts on the health of the nurses and on the care they deliver. The current study expands our understanding of sleep health on workdays and work-free days among nursing workforces across care settings and specialties.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The University of Washington Hester McLaws Nursing Dissertation Scholarship provided the funds for data access fees. Research reported in this paper was supported by the National Institute for Occupational Safety and Health (NIOSH) under Federal Training Grant T42OH008433. The content is solely the responsibility of the authors and does not necessarily represent the official views of NIOSH. The study sponsors were not involved in the study design, analysis, data interpretation, or the writing of this dissertation. The Nurses’ Health Study 3 was supported by grants U01-HL145386 from the US National Institutes of Health. This work was supported, in part, by the National Institutes of Health, National Institute of Nursing Research Training Program in Global Health Nursing at the University of Washington (T32 NR019761).
Ethical Approval
The NHS3 parent study protocol is approved by the Brigham and Woman’s Hospital and Harvard T.H. Channing School of Public Health Institution Review Boards. The current study was reviewed by the University of Washington Institution Review Boards and deemed exempt as a Not Human Subjects determination.