
Abstract
Background:
Training and education may benefit nurses whose nonstandard work hours put them at risk of poor sleep, fatigue, and ensuing adverse health and safety outcomes. The National Institute for Occupational Safety and Health (NIOSH) published “Training for Nurses on Shift Work and Long Work Hours” in 2015 as a free online resource which remains one of the few trainings available on this topic. However, the extent to which nurses have completed the program and the characteristics of current learners have not been examined.
Objective:
We aimed to describe the potential reach of the NIOSH Training for Nurses between May 2015 through December 2020.
Methods:
Data were obtained on learners who received continuing education credits upon completion of the NIOSH Training for Nurses. We applied a widely used implementation and evaluation framework, RE-AIM (Reach, Effectiveness, Adoption, Implementation, Maintenance), to describe the potential reach of the nurses’ training and provide descriptive statistics of learners.
Results:
From 2015 to 2020, 7899 learners from different occupations received continuing education credits for completing the training. Approximately 60% of learners were nurses and 30% were students. Among nurses, most were Registered Nurses (93%), with few Licensed Practical Nurses (6%) and Advanced Practice Nurses (2%). In 2020, the number of learners who were nurses represented only 0.09% of all licensed US nurses.
Conclusion:
A renewed dissemination plan may help extend training reach to the larger population of licensed US nurses. The NIOSH training remains a seminal, freely available, online resource for nurses, filling a critical gap in training to manage work-related fatigue.
The nursing profession often requires exposure to nonstandard schedules involving long and irregular work hours (eg, overnight shifts, early start times), which increase the risk for adverse health and safety outcomes.1-5 Additionally, these work hours often affect nurses’ ability to obtain adequate sleep.6,7 Recent studies and meta-analyses have reported that due to shift work and long work hours, nurses commonly experience poor sleep quality and less than the recommended minimum of 7 hours of sleep per 24 hours.8-10 Nurses who experience sleep impairment may exhibit symptoms of cognitive decrements and/or fatigue that can be compounded by high levels of physical and/or mental exertion,11-13 potentially furthering risks for safety critical events such as patient errors and work injuries.14,15 Despite the increased risks, there are few opportunities during nursing education or employment where nurses are offered the training or support needed to mitigate risks associated with irregular work hours, poor sleep, and fatigue. 16
One method to increase nurses’ awareness and knowledge about working nonstandard hours is to offer training and education on the risks and consequences of irregular work hours, such as sleep impairment, and provide information on effective mitigation strategies. Training for workers with nonstandard schedules has been found to improve sleep outcomes, reduce acute fatigue, and decrease stress and burnout. 17 While such training is federally mandated in some industries with high public safety risks, such as aviation, 18 training is not required in the high-stakes field of healthcare, despite the potential harm to patients and healthcare workers. In addition, a recent scoping review reported a limited number of programs are available to nurses on how to support their health and safety while engaging in nonstandard work schedules. 16
To address this knowledge gap, the Centers for Disease Control and Prevention (CDC) and National Institute for Occupational Safety and Health (NIOSH) published “Training for Nurses on Shift Work and Long Work Hours” in 2015. 19 The goal of this free, publicly available online training is to “educate nurses and their managers about the health and safety risks associated with shift work, long work hours, and related workplace fatigue issues and to relay strategies in the workplace and in the nurse’s personal life to reduce these risks.”19(para 1) This comprehensive, evidence-based training was developed by experts in the fields of nursing, occupational safety and health, sleep, and fatigue. Prior to publication, it was tested with several nurse focus groups and revised accordingly. 19 The training is presented in 2 parts, which can be completed independently, and takes approximately 3.5 hours to finish. Part 1 includes information about how shift work and long work hours contribute to sleep loss, poor quality sleep, cognitive impairment, fatigue, and other health and safety risks. Part 2 contains personal and workplace strategies for nurses and managers to enhance sleep and reduce risks associated with nonstandard work schedules. Short quizzes are included throughout to reinforce learning objectives. Upon completion, learners can obtain continuing education (CE) certificates from the CDC for either one or both parts of the training.
Since its publication, the training has been shared nationally and internationally through multiple channels and partnering organizations. Some groups and organizations promoting the training included the Agency for Healthcare Research and Quality, the American Nurses Association, the Harvard School of Public Health, the Occupational Safety and Health Administration, nursing unions, and members of the NIOSH Healthcare and Social Assistance Sector Council (C. Caruso, personal communication, September 28, 2024). These organizations recommended the training in several of their articles and on their websites.20,21 The training was also promoted in English and Spanish within scientific articles published in nursing, sleep medicine, and women’s health journals,22-27 during conference presentations, and via CDC/NIOSH science blogs and social media platforms.28-30 NIOSH continues to promote the training annually on social media platforms during National Nurses Week in May 28 and at the beginning and end of Daylight Savings Time.29,31 CDC Training and Continuing Education Online also periodically highlights the training on their website. However, there is limited information about the potential reach of these dissemination efforts and learners who have taken this training. Identifying attributes of learners (eg, profession and nurse licensure) may help identify nursing populations who may be exposed to and benefit from the training but are not accessing the content.
Purpose
The purpose of this study is to describe the potential reach of the NIOSH Training for Nurses on Shift Work and Long Work Hours between May 2015 through December 2020 and to describe the characteristics of current learners. Determining training reach may help identify areas to improve awareness about, and uptake of, this and future workplace sleep and fatigue programs.
Study Framework
This study was guided by the RE-AIM (Reach, Effectiveness, Adoption, Implementation, Maintenance) Framework, developed in 1999 to assist public health researchers and practitioners in identifying, assessing, and reporting key implementation outcomes. 32 RE-AIM is a multilevel framework that considers individual-level program outcomes (reach, effectiveness, and maintenance) as well as setting- and staff-level outcomes (adoption, implementation, and maintenance) leading to program impact. RE-AIM asks: Who is the program reaching (Reach)? How effective is the program (Effectiveness)? What is the setting and who are the providers adopting the program and delivering it (Adoption)? How was the program implemented (Implementation)? Can it be maintained and if so, how (Maintenance)?33,34 RE-AIM can be used across all phases of a program including in planning, delivery, and evaluation and can be assessed collectively or individually. The RE-AIM framework has been applied by researchers and public health practitioners to a variety of contexts, populations and health and safety issues across diverse clinical and community settings. 34 However, the literature suggests not only modest uptake but also significant potential, of RE-AIM to enhance the quality, efficiency, and impact of occupational safety and health practices and programs. 35
In the current study, we assess the reach dimension of the RE-AIM framework to better understand the characteristics of learners who completed the NIOSH Training for Nurses. Reach is defined as the absolute number, proportion, and representativeness of eligible individuals (eg, workers, students, patients) who receive an intervention, and their representativeness compared to the total population who could receive it (often compared to those who are invited to participate but decline).33,34 Describing program reach can inform where additional dissemination strategies may be needed to enhance the awareness about and uptake of the training.
Ethics
This activity was reviewed by CDC, deemed not research, and was conducted consistent with applicable federal law and CDC policy.§
Methods
Data
Data were provided by CDC of all CE credit recipients of the Training for Nurses on Shift Work and Long Work Hours from 2015 through 2020. As part of receiving CE credits, learners were required to provide information about their highest level of educational attainment, region of residency, and occupational characteristics (Supplemental File). Occupational characteristics were ascertained with open-ended questions and multiple-choice options. Characteristics included profession and work setting (eg, hospital, clinic, long term care facility). Nurse licensure and detailed professions (eg, Nurse Anesthetist, Midwife, Clinical Nurse, Educator) were also included. To reduce the risk for subject identification, we followed minimum reporting guidelines from the National Center for Health Statistics and did not report any categories with 30 or fewer responses. 36
Study Definitions: Learner Characteristics
We first described characteristics for all learners and followed with a more detailed analysis of nurse learners. Among all learners, we reported geographical location, educational level, and profession. Geographical region was determined using residency information. Learners living in the United States were grouped into Northeast, Midwest, South, or West regions following definitions from the United States Census Bureau. 37 Learners living outside the United States were categorized as International. Educational level was self-reported from 12 categories ranging from postsecondary to less than high school. We combined these into 4 categories (High school or less, Some college [including Associate and technical degrees], Baccalaureate degree, and Post-Baccalaureate graduate degree), to align with the educational levels required in the nursing workforce. 38 For profession, CDC provides learners with 38 options from which to choose (Supplemental File). After consulting with nursing researchers and occupational health experts, we combined these into 9 categories. Decisions on combining professional categories were based on similar job tasks and required skill levels. For example, all professions (eg, K-12 educators, secondary education faculty) who spend a majority of their time teaching were categorized as “educators.”
Among nurse respondents, we further described licensure and work setting. Licensure was self-reported as “Advanced Practice Nurse” (APRN), “Licensed Practical or Vocational Nurse” (LPN/LVN) and “Registered Nurse” (RN). While all include the title of “nurse,” APRNs, LPN/LVNs, and RNs require different education requirements and state licensing that allows them to provide distinct levels of care. Scope of practice broadens with each type of nursing, with LPN/LVNs giving basic patient care, RNs providing more complex care, assessments, and coordination of care, and APRNs assessing, diagnosing, and prescribing medications to patients. 39 We consulted with nursing experts to combine self-reported “Work setting” responses from 15 to 8 categories (ie, Behavioral/Mental Health Facility, Educational Institution, Government Institution, Home Healthcare/Hospice/Long-Term Care, Hospital, Other Healthcare-related, Other Work Setting, Outpatient Care Center) aligning with category groupings from the 2020 National Nursing Workforce Survey. 38 More information on what type of worksites were included in each group can be found in the Supplemental File.
Analyses
We examined training usage from 2015 to 2020, for both Parts 1 and 2 separately, as CE credits were issued independently for completion of each part. The data did not allow for linkage of CE credits to determine which learners completed both parts. We report descriptive statistics (frequencies, percentages) for year, geographical region, education level, profession, licensure, and work setting for nurse learners. Inferential statistics were not required, as the data collected represents the complete population of learners, and not a representative sample. To assess the potential reach of the training among nurses, we compared the population of licensed nurses who received CE certificates with the eligible population of licensed US nurses reported in the National Council of State Boards of Nursing 2020 Nursing Workforce Data Reports. 38
Data were analyzed using SPSS Statistics version 29 (IBM Corp., Armonk, NY, USA). Results were reported following the RE-AIM Reach quantitative reporting recommendations. 40
Results
Between 2015 and 2020, a total of 7899 individuals completed and obtained a CE certificate for Part 1 (Shift Work Health and Safety Risks; Figure 1). For Part 2 (Personal and Workplace Mitigation Strategies), a total of 7747 individuals received CE certificates upon completion of the training (Figure 1). This small difference in CEs issued for both parts of the training (n = 152) possibly suggests most learners completed the entire course.
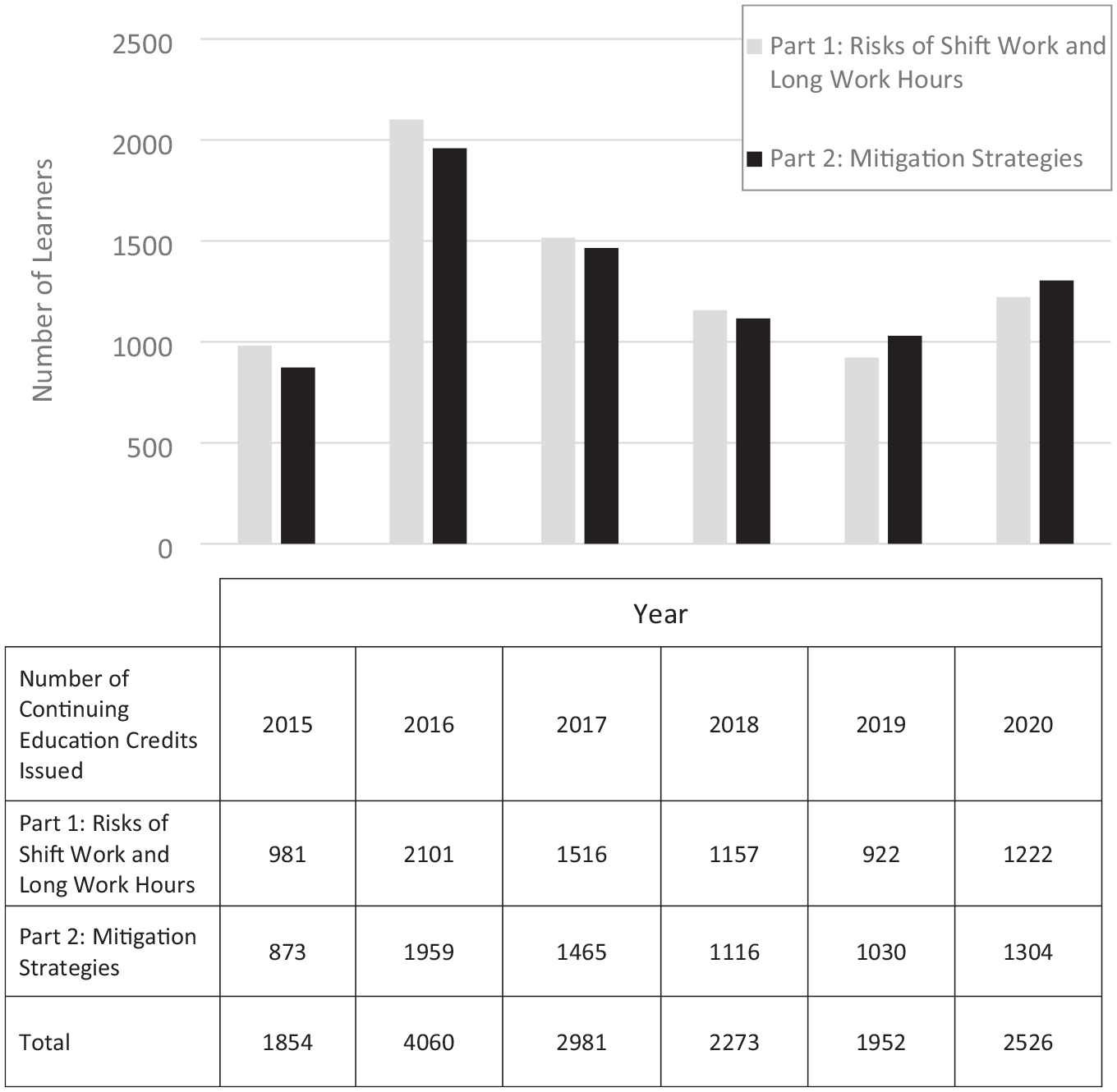
Number of learners receiving CE training for completing the NIOSH Training for Nurses on Shift Work and Long Work Hours, by training part and year (Part 1 N = 7899, Part 2 N = 7747). The NIOSH Training for Nurses on Shift Work and Long Work Hours is offered in 2 parts. Learners have an option to complete one or both parts of the training. CE credits are issued independently for completion of Parts 1 and 2. Part 1 contains information about how shift work and long work hours contribute to fatigue and other health and safety risks. Part 2 includes strategies nurses and their managers can employ to reduce the risks for adverse outcomes when working irregular work hours.
Our analyses of the trend in training usage show a peak usage in 2016, followed by a decreasing trend until 2019 (Figure 1). However, in 2020, there was a slight increase in CE credits issued for both parts of the training. When examining usage of Parts 1 and 2 separately, it appears that between 2015 and 2018, there were slightly more CE credits issued for Part 1 (ie, risks) compared to Part 2 (ie, mitigation strategies). In 2019, this trend shifted, with more Part 2 (ie, strategies) CE credits issued than Part 1 (ie, risks).
Due to the small difference (n = 152) between the number of CEs issued for completion of Parts 1 and 2, we hypothesize that most learners may have completed both parts of the training. Therefore, for the remainder of this analysis, we report only on the number of learners who received credit for Part 1 (N = 7899).
Most US learners reported living in the Midwest region (n = 2943, 37.3%), followed by the South (n = 2097, 26.5%), Northeast (n = 1392, 17.6%), and Western regions (n = 1224, 15.5%) (Figure 2). International learners made up the smallest portion at 3% (n = 239). Across education levels, a majority of learners reported completing a Baccalaureate degree (n = 4402, 56.2%) or some college (including Associate degrees and technical degrees) (n = 2439, 31.1%) (Table 1).
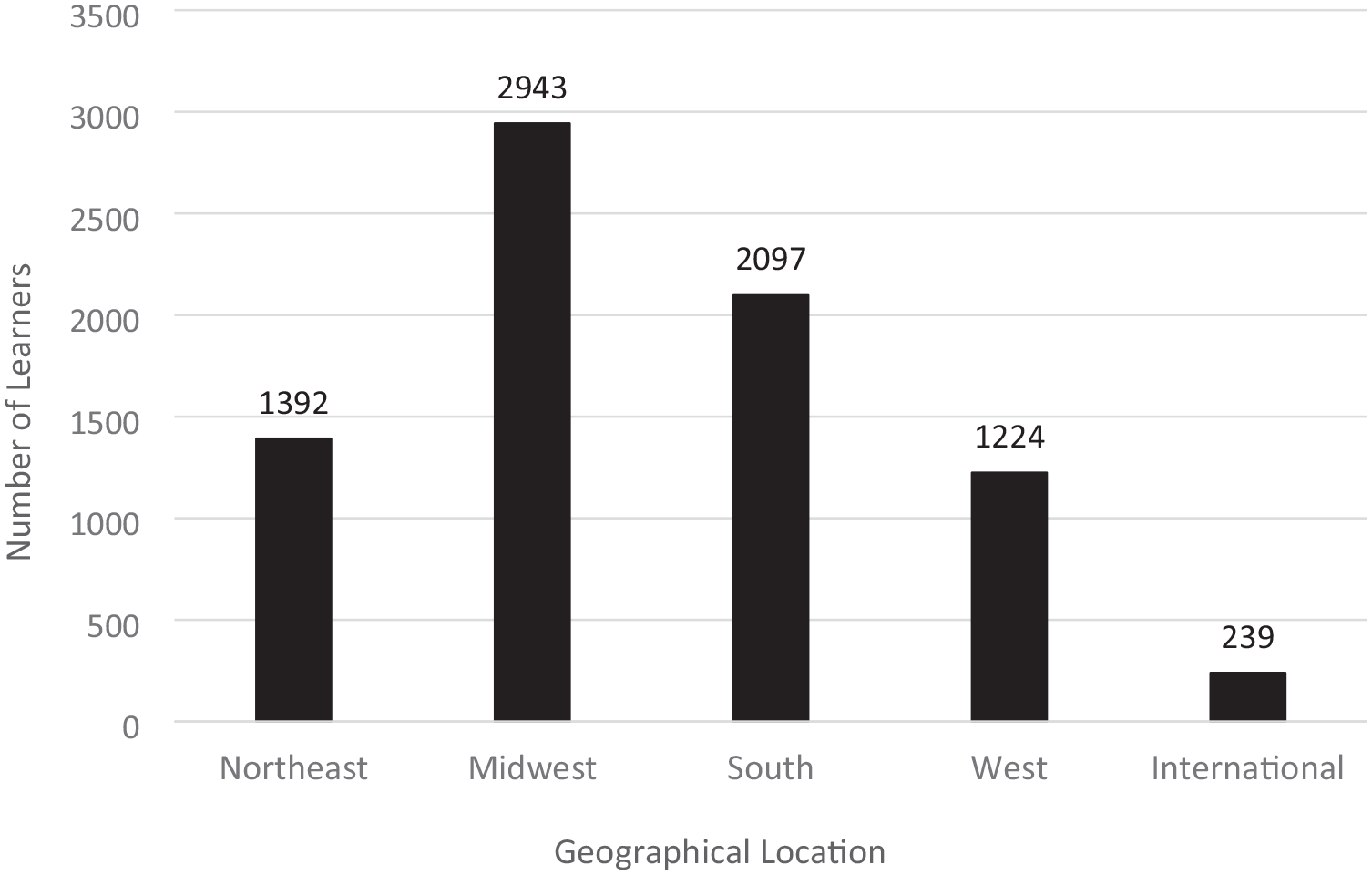
Number of learners completing Part 1 of continuing education training by geographical location, 2015 to 2020 (N = 7899).a The NIOSH Training for Nurses on Shift Work and Long Work Hours Part 1 includes information on health and safety risks associated with shift work and long work hours.
Characteristics of All Learners Issued Continuing Education Certificates for Part 1 Training by Education and Profession, 2015 to 2020 (N = 7899).
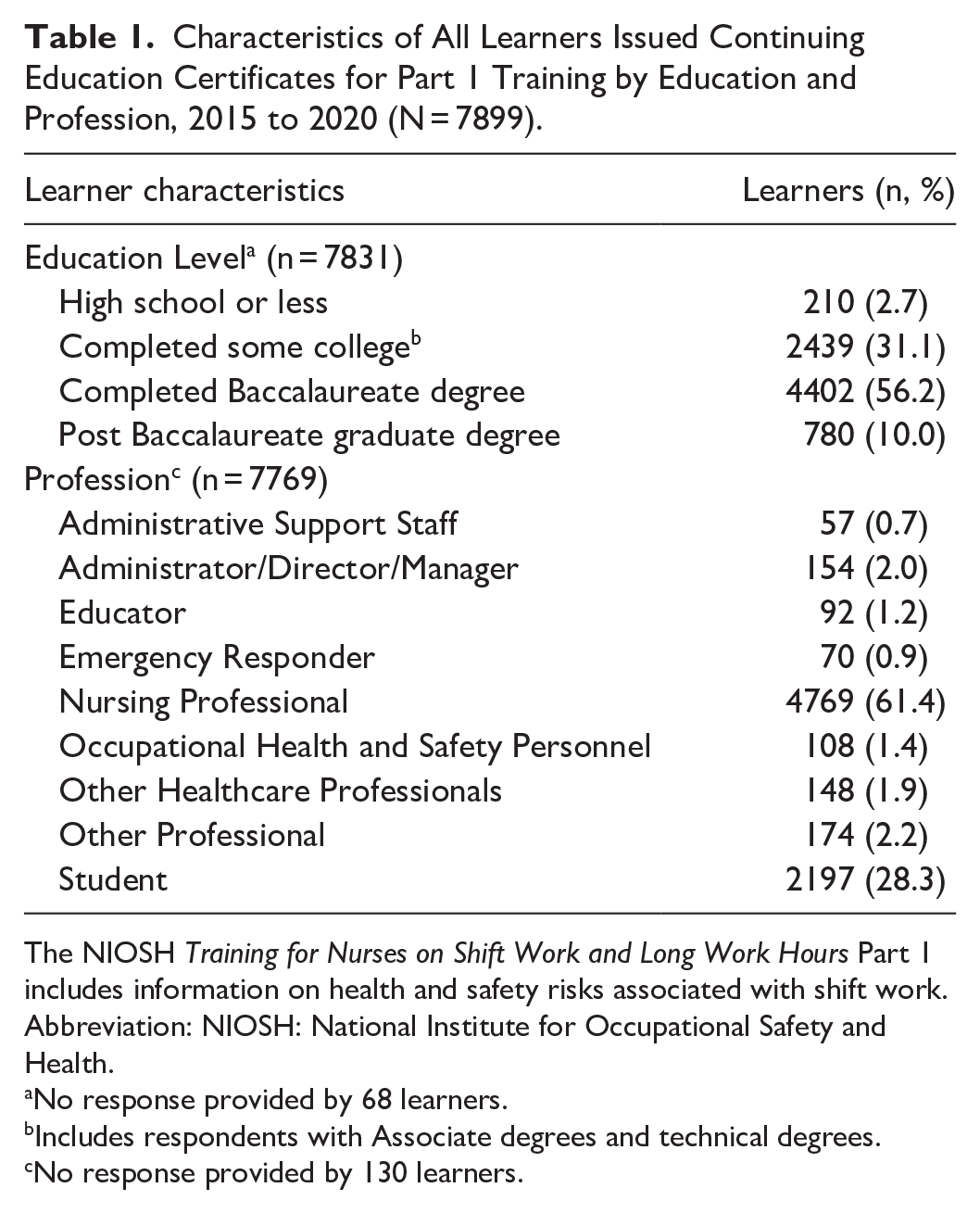
The NIOSH Training for Nurses on Shift Work and Long Work Hours Part 1 includes information on health and safety risks associated with shift work.
Abbreviation: NIOSH: National Institute for Occupational Safety and Health.
No response provided by 68 learners.
Includes respondents with Associate degrees and technical degrees.
No response provided by 130 learners.
While most learners were nurses (n = 4769, 61.4%), the second largest group of learners comprised students (n = 2197, 28.3%) (Table 1). However, not all student respondents provided details of the type of education they were taking, so it is unclear how many might be nursing students. Other health professionals included were emergency responders (n = 70, 0.9%), occupational health and safety personnel (n = 108, 1.4%), and other healthcare professionals (n = 148, 1.9%) such as physicians and certified nursing assistants. Nonhealthcare groups included administrative support staff (n = 57, 0.7%), administrator/director/managers (n = 154, 2.0%), educators (n = 92, 1.2%), and other professionals (n = 174, 2.2%).
Nursing-Specific Reach and Characteristics
Among nursing professionals (Table 2), RNs made up the majority of learners (n = 4431, 92.9%), followed by LPN/LVNs (n = 244, 5.5%) and APRNs (n = 94, 2.0%). We estimated the reach of the NIOSH “Training for Nurses” in 2020 among US nurses who were eligible and potentially exposed to the training was 0.09%. The basis for this estimate is on a total of 5 142 844 nurses licensed the United States in 2020, per the National Council of State Boards of Nursing. 38 Nurse learners reported working in a variety of settings (Table 2). The largest percentage of nurses reported working in hospital settings (n = 3146, 66%), followed by healthcare/hospice/long-term care work settings (n = 387, 8.1%) and outpatient care centers (n = 350, 7.3%). Other worksites identified by nurse learners included other (non-healthcare-related) work settings, other healthcare-related settings, behavioral/mental health facilities, and government institutions.
Characteristics of Nurses Issued Continuing Education Certificates for Part 1 Training by Licensure and Work Setting, 2015 to 2020 (n = 4769).
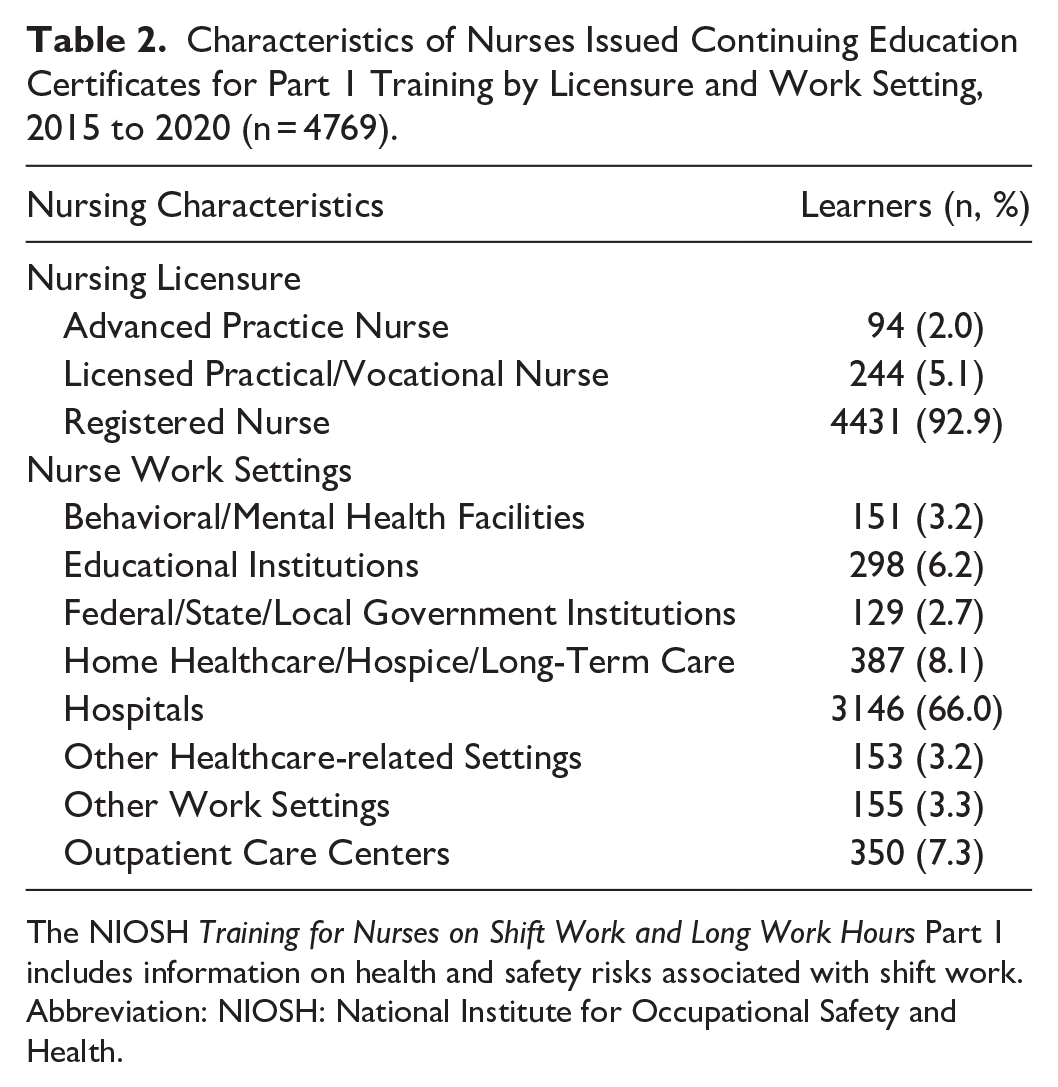
The NIOSH Training for Nurses on Shift Work and Long Work Hours Part 1 includes information on health and safety risks associated with shift work.
Abbreviation: NIOSH: National Institute for Occupational Safety and Health.
Discussion
This study aimed to describe the population of learners who obtained CEs between 2015 and 2020 for completion of the NIOSH “Training for Nurses in Shift Work and Long Work Hours,” one of the only freely accessible educational offerings on shift work and fatigue tailored for the nursing workforce.16,19 Characterizing the user population can assist in establishing the potential reach of the training among eligible learners.
When examining the trend in usage, almost 7900 individuals registered and completed this CE offering during the first 5 years of publication, 60% of whom identified as nursing professionals. We observed a peak in training completion in 2016, which may reflect the results of dissemination efforts following publication of the training through key organizational partners (eg, American Nurses Association, nursing unions). After a gradual decline of learners following 2016, we also observed a rise occurring after 2019. This increase may be indicative of the changing work environments and additional promotion through scientific publications, such as articles in journals for nursing leaders and publications celebrating National Nurses Week on the NIOSH website.24,28 A renewed NIOSH dissemination plan also preceded a required CE reaccreditation in 2019 (C. Caruso, A. Hornbeck, personal communication, March 13, 2024). Future research may help identify dissemination strategies and channels for promoting training uptake.
The results of this study indicate the greatest proportion of learners reside in the Midwest. This may be due to the almost 1.2 million RNs licensed in the region (as of 2020), representing the second largest prevalence of licensees across the 4 regions examined.38,41 Although the Southern region has the highest prevalence of RNs compared to the other 3 regions, we did not find this to be the highest proportion of learners for the NIOSH nurses training. The reasons are unclear and may warrant further investigation. The Northeast and West had lower proportions of US learners compared to the Southern and Midwest regions. This is unexpected given that these regions include California and New York, the 2 states with the largest population of nurses in the United States. 38 Identifying regions and specific states with low potential reach among eligible training participants may highlight areas where additional outreach and dissemination activities with state boards of nursing and/or professional nursing organizations may be warranted. Provision of these trainings may help promote health and safety among nurses and improve worker retention, which is needed given recent predictions of RN and LPN/LVN shortages in the United States.42,43 Understaffing has been associated with increased workloads, extended work hours, and worker fatigue, with further effects on high workforce turnover.44,45
The majority of learners of the NIOSH “Training for Nurses in Shift Work and Long Work Hours” reported completing a Baccalaureate degree, or some college, which includes Associate or technical degrees. These results align with the requirements for individuals to have a technical or college degree in order to apply for a nursing license. 46 In addition, studies have also shown that workers with a higher educational background are more likely to participate in voluntary wellness programs. 47 As such, this provides an indication of the reading comprehension level that would be suitable for future training programs aimed at nurses.
While the majority of learners were nurses (60%), a large part of the remainder (~30%) were students. Student learners were not required to provide details about their current school program or major. However, it is plausible that most were nursing students because the training is designed for nurses, and nursing school practicums often require irregular work hours. Recent updates to the Core Competencies for Professional Nursing Education include teaching students about the work environment as a quality and safety competency. 48 To meet these competencies, nursing student curricula could include CE training on sleep and fatigue, such as the NIOSH training discussed in this study. This may help to promote health and workplace safety culture, as poor sleep among nursing students is associated with mental health distress and sleepiness, with further effects on reduced confidence with patient care and ability to engage in safe work practices.49,50 Additionally, poor sleep and fatigue may extend beyond graduation, as Varner et al 51 found that new nurses experienced disrupted sleep during their first year of their careers, indicating the transition into professional settings may be a challenge. This is concerning as sleep disturbances have been associated with higher turnover rates among novice nurses. 52 Tailored communication and education efforts to support sleep health may improve workforce retention, offer cost savings related to reduced turnover, and provide broader gains, such as improved patient outcomes. 53 Examples for further dissemination efforts among nursing students may include sharing the training directly via student nurse associations. Other strategies could involve outreach to schools of nursing through conferences, publications, and national nursing education associations, where education standards are established.
We found the majority of learners of the NIOSH Training were RNs. Excluding those who also hold APRN licenses, RNs make up 78% of nurses licensed in the United States. 38 However, a small proportion of learners reported being APRNs or LPN/LVNs, suggesting that additional efforts for dissemination among these groups of nurses may be beneficial. APRNs and LPN/LVNs are employed in hospital settings and long-term care facilities where they are also subject to shiftwork, unpredictable shifts, and on-call work, possibly resulting in extended work hours.38,54 Driven by the concern about worker fatigue, the American Association of Nurse Anesthetists and the American College of Nurse-Midwives published position statements on the importance of provider sleep to patient safety with guidance on how APRNs and APRN students can mitigate the risks associated with fatigue.55,56
Perhaps the most surprising finding is that less than 1% of the US nursing population has obtained CEs for the NIOSH “Training for Nurses on Shift Work and Long Work Hours,” despite widespread dissemination efforts including NIOSH social media posts, promotion among professional nursing organizations, such as the American Nurses Association and nurse unions, and a policy brief published in Nursing Outlook, a journal for nurse leaders. 24 Authors of a recent systematic review on nurse fatigue noted significant relationships between high levels of nurse fatigue and poor mental health outcomes, lower perceptions of on-the-job performance, higher rates of sick absences, and nurse turnover, 57 of which total costs in the United States have been estimated as high as $8.5 million annually. 53 This indicates more work may be needed to inform nurses about the risk of nonstandard schedules and effective mitigation strategies, the benefits of which may be impactful for the entire healthcare system.
However, the low potential reach of the training may not reflect the true number of learners, as not all nurses who have completed the training may have requested CE credits, despite incentives to meet nursing licensing requirements. Further efforts are needed to understand the barriers to learner uptake and where alternative dissemination methods may be needed, including among groups harder to engage in workplace health promotion programs, such as night shift nurses. 58 Additionally, better methods for monitoring and measuring dissemination efforts would offer a more accurate measure of success.
Futher investigation could assess if the training is meeting the learning needs of the current nursing population. Nurses have competing demands at work and home, limiting their time for sleep and motivation. 9 As a result, they may not have time or desire to take a long training. Recent evidence suggests that nurses desire asynchronous online learning to allow completion of learning at times convenient for them. 59 Additionally, some may seek out other methods to obtain CEs, such as attending an accredited conference where a large number of nursing CEs are offered. However, recent research on microlearning, a learning method that delivers concise (usually 5-10 minutes) and focused content, in an asynchronous, flexible, and on-demand manner, suggests digital learning tools can successfully reach today’s busy adult learners.60,61 This is supported by a recent scoping review proposing that nurse sleep and fatigue education delivered through multiple methods (eg, in-person, mobile phone applications) may benefit a larger audience. 16 Additionally, nurses and other healthcare professionals prefer obtaining information through short podcasts (less than 30 minutes long) allowing them to multitask and review content as often as needed to reinforce knowledge.62,63 Finally, expanding the training to build knowledge and behavioral skills to improve sleep hygiene and fatigue mitigation skills may also be warranted. 16
Limitations
Although this study has been helpful in identifying where gaps in assessing the potential reach of the NIOSH “Training for Nurses in Shift Work and Long Work Hours” exist, there are limitations to acknowledge. Primarily, results may be biased by who chose to obtain CE credits. The training is freely accessible online and CE credit completion is not required to view the content, so some users may not have been captured in the data. While this is a limitation, potentially biasing results, most nurses need CE credits for state licensure renewal, suggesting a high proportion of nurses took advantage of this offering. Second, due to data limitations, we were unable to match whether learners completed both Part 1 and Part 2 of the training and the corresponding completion dates. Additionally, individuals are able to repeat training and obtain the same CE credits in subsequent years. Therefore, data over the 5-year span may include individuals who have repeated the content, potentially inflating our results. If this is the case, it would further underscore the limited reach of the training, emphasizing the need to consider a broader dissemination plan. Another limitation includes not being able to calculate the true denominator of the reach measure due to the difficulty of estimating how many individuals in the population of interest were aware of the training but declined to engage, and how these people differ from those who did take the training. While reach is typically measured quantitatively, the “who, what, why, and how” of reach may be better explored through qualitative inquiry. 34 Finally, this study used previously collected data, thus limiting the scope of research questions that could be addressed about the training reach.
Conclusion
Training aimed at reducing fatigue among nurses and other workers is an integral component of a shared-responsibility approach to managing occupational fatigue. 64 While this study has found the potential reach of the NIOSH “Training on Shift Work and Long Work Hours” across different nursing licensure types, US geographical regions, and multiple work settings, large gaps in potential reach exist across the existing population of US nurses. Future qualitative research is needed to complement the findings of this quantitative analysis to explore barriers to training uptake among the nursing population. Nevertheless, this study provides valuable insights on the training usage and characteristics of learners and serves as a baseline measure for future sleep and fatigue education programs. Additional efforts may be needed to improve dissemination and uptake. This is important because the provision of this free, on-demand training, which offers CE credits to maintain professional licensure, addresses a critical need when there is limited scientifically based sleep and fatigue education for nurses. As such, it continues to serve as an important resource to enhance organizational efforts to mitigate fatigue risks and support a shared approach to occupational health and safety.
Supplemental Material
sj-pdf-1-wjn-10.1177_01939459251340273 – Supplemental material for Reach of an Occupational Health and Safety Program to Improve Sleep and Fatigue Among Nurses
Supplemental material, sj-pdf-1-wjn-10.1177_01939459251340273 for Reach of an Occupational Health and Safety Program to Improve Sleep and Fatigue Among Nurses by Beverly M. Hittle, Rebecca Guerin and Imelda S. Wong in Western Journal of Nursing Research
Footnotes
Acknowledgements
The authors would like to thank the following individuals for their help with this publication. Mike Barker, PhD, from the National Institute for Occupational Safety and Health (NIOSH) who offered additional advice on statistical analysis. Lynda Robson, PhD from the Institute of Work and Health, for critically reviewing prior manuscript drafts. Adam Hornbeck, MSN, APRN at NIOSH who provided additional details on the training dissemination, as well as reviewing prior manuscript drafts. Finally, we would like to thank all those who have taken the NIOSH Training for Nurses on Shiftwork and Long Work Hours.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by internal CDC/NIOSH funding. Dr. Hittle is currently supported by the National Institute for Occupational Safety and Health, Grant # K01OH012549.
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the National Institute for Occupational Safety and Health, Centers for Disease Control and Prevention. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Office of the Provincial Health Officer, Ministry of Health, Government of British Columbia. This work was prepared while Dr. Imelda Wong was employed at the National Institute for Occupational Safety and Health, Centers for Disease Control and Prevention.
Ethical Considerations
This activity was reviewed by CDC, deemed not research, and was conducted consistent with applicable federal law and CDC policy. (See eg, 45 C.F.R. part 46, 21 C.F.R. part 56; 42 U.S.C. §241(d); 5 U.S.C. §552a; 44 U.S.C. §3501 et seq.)
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.