
Abstract
Background:
Any form of discrimination directly opposes the ethical principles and values of the nursing profession. Discriminatory care is a major moral challenge to healthcare systems around the world.
Objective:
This study aimed to explore clinical nurses’ experiences of discrimination against patients.
Methods:
This qualitative study used a conventional content analysis approach. Thirteen nurses were selected through purposive sampling from various clinical units at public and private hospitals in Iran. Data collection was conducted through semi-structured interviews, and data analysis was performed using Granheim and Lundman’s 5-step method.
Results:
The study identified 3 main themes and 6 subthemes. These include “duplicity in the application of organizational rules” (comprising differences in providing hospitalization and patient accommodation services and ignoring organizational regulations in providing welfare services), “inequality in relationship with patients” (encompassing disregard for ethical considerations in patient relationships and differential physical presence at the patient’s bedside), and “differences in the delivery of care and treatment services” (involving neglecting patients’ needs in care provision and expediting the provision of interdisciplinary services).
Conclusion:
This study underscores that discrimination in health care extends beyond direct patient care, infiltrating physical, material, and even intangible aspects such as communication style and patient attention. To combat this pervasive issue, nurses must receive comprehensive education about the various forms of discrimination. By implementing both immediate and long-term strategies, including policies and programs, we can work toward creating a more inclusive and respectful healthcare environment for all.
Nursing performance and professional standards are based on equality, 1 which means that nurses should respect patients’ human rights and dignity, avoid making assumptions, and acknowledge diversity and personal preferences. 2 Discrimination refers to a situation in which individuals with the same role do not receive equal social benefits. 3 In healthcare, this concept refers to the non-provision, incomplete provision, or differential provision of healthcare to an individual or group of individuals based on personal or social characteristics. 4 It can also be defined as unfair and unequal treatment of individuals based on specific identifying factors, such as race, ethnicity, and gender. 5
Various studies have elucidated the complex ways in which discrimination can impact individuals’ health, including physiological responses, internalization of negative stereotypes, and maladaptive coping behaviors such as substance abuse and physical violence. 6 In addition, experiences of discrimination in healthcare settings can affect the quality of care, the patient-nurse relationship, patient satisfaction, healthcare utilization, health outcomes, and unequal access to resources.7,8 The significance of this issue is emphasized by the 2030 United Nations Sustainable Development Goals, which prioritize the elimination of discrimination in healthcare settings. 9
Understanding and identifying nurses’ experiences of discrimination against patients in healthcare settings is essential. First, the healthcare system bears both a moral and legal obligation to perform equal care to all patients, irrespective of their demographic characteristics or other attributes. 10 Second, discrimination in healthcare environments can lead to patients feeling disconnected from the healthcare system, potentially harming their future healthcare experiences and overall well-being. 11
Although there are international antidiscrimination laws and ethical codes supporting the importance of respecting patients’ rights, discriminatory care is still provided in some cases. Therefore, research in this area is crucial for improving the delivery of healthcare services. 12 On the other hand, knowing the various forms of discrimination can help identify ethical challenges in patient care and treatment, which will ultimately increase patients’ trust in healthcare systems, improve the standard of care, increase patient satisfaction, and lessen nurses’ susceptibility to ethical dilemmas. 13
Discrimination is an internalized feeling shaped by interpersonal interactions, meaning that individuals may perceive and experience discrimination differently. Perceived discrimination refers to a person’s experience or perception of negative and unfair behaviors that prevent individuals or groups from being treated equally. 14 Although discrimination is a subjective phenomenon, people’s experiences of it can differ greatly, so qualitative research is required to examine the subjective and covert aspects of discrimination. In addition, the majority of prior studies have been quantitative and focused on the prevalence and causes of discrimination. Although nurses may unintentionally engage in discriminatory behaviors that patients are unaware of, these behaviors can still harm patients’ health. By qualitatively defining and identifying instances of discrimination from the perspective of nurses, a more specific conceptual understanding of this phenomenon is made possible, one that is both more easily understandable by nurses and generalizable to clinical settings, in contrast to many studies that define discrimination in general terms. Having such definitions makes it easier for nurses to identify overt and covert forms of patient discrimination.
Iran’s healthcare system is run by the Ministry of Health, Treatment, and Medical Education and consists of both public and private hospitals. The public sector is typically associated with the University of Medical Sciences, and some government agencies also have hospitals that offer health services to their employees. The issue of nondiscrimination in healthcare has been examined in Iran, and several ethical guidelines have been prepared for medical groups.
The Charter of Iranian Patients’ Rights and the Code of Nursing Ethics were implemented in 2010. The Charter directly emphasizes providing services to patients without any kind of discrimination, 15 and The Code of Nursing Ethics also requires nurses to provide care without discrimination. 16 Medical and nursing ethics are implemented in the curricula of nurses and physicians. Accreditation of hospital services also emphasizes respect for patient’s rights and providing care without discrimination. 17 Therefore, given the importance of identifying discriminatory nursing care, this study explored clinical nurses’ experiences of discrimination against patients.
Methods
This study used a conventional content analysis approach to explore clinical nurses’ experiences of discrimination against patients in 2024. Content analysis is a descriptive qualitative research method that facilitates the exploration of health-related phenomena. 18 This methodological choice allowed participants to articulate their perceptions of discriminatory nursing care based on their experiences and provide concrete examples of discriminatory practices. The study was conducted in public and private hospitals in Tehran, Iran. This setting was selected because it provides services to a diverse patient population, including sex, age, culture, and economic status.
Research Participants
The participants comprised nurses working in therapeutic departments directly involved in clinical care delivery to patients. The initial selection of participants was accomplished through purposive sampling, adhering to predetermined criteria for study inclusion. Subsequently, additional participants were selected based on the information obtained from the initial participants. To be included in the study, the nurses had to actively work in clinical departments for at least 6 months, display interest in participating, and have relevant experience related to the topic under investigation. The objective was to gather a diverse sample of participants based on age, gender, marital status, work experience, educational background, departmental affiliations, and hospital settings.
Data Collection
Data were collected through semi-structured, face-to-face, and online individual interviews. The first author, a PhD student in nursing with a valid license, conducted interviews in Persian from June 2023 to May 2024. He visited hospitals to invite eligible interviewees. The purpose and research procedures were explained to potential participants during the visits. Once mutual agreement was reached regarding the interview timing and venue, data collection was initiated. First, the interviews began with general questions such as, “Have you ever had to differentiate between patients and provide varying levels of care to them? Please explain your experience” followed by subsequent questions based on the interviewee’s answers. Further exploratory and follow-up inquiries were posed, such as “Could you elaborate further on your statement?” and “Could you provide more context about this specific incident?” The interviews took place individually in quiet settings, without external presence, and continued until participants felt they had conveyed all relevant information. During the interviews, participants’ voices were recorded and notes were taken. After each interview, the participants were allowed to add more comments. The possibility of subsequent interviews or follow-up questions was also mentioned, along with expressions of gratitude for their contributions. By employing continuous comparative analysis, the researcher compared new data with the codes and themes extracted from previous data to assess whether the new information introduced a novel pattern. In fact, after conducting the 11th interview, no new codes emerged, and the same themes and patterns from previous interviews were repeatedly observed, with no new perspectives or insights being obtained. However, to ensure data saturation, 2 additional interviews were conducted. After reviewing the existing codes in a meeting with the research team, data saturation was confirmed.
Data Analysis
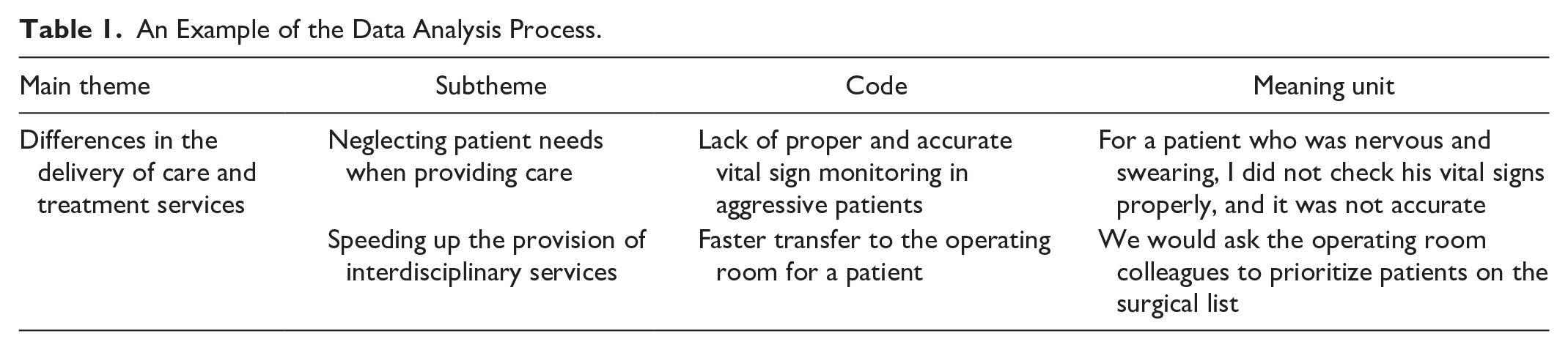
The research used Graneheim and Lundman’s content analysis method, which includes 5 distinct steps. 19 After each interview was completed, the audio recordings were transcribed, and multiple careful readings were conducted to obtain a comprehensive understanding of the interviews. Then, significant statements (semantic units) were identified and classified. Next, similar open codes were extracted to ensure semantic clarity, and these codes were named as classes and subclasses. Throughout the study, the research team continuously reviewed the coding process. It is essential to note that data analysis occurred simultaneously with data collection. An example of this analysis process is illustrated in Table 1.
An Example of the Data Analysis Process.
Rigor
This study aimed to produce reliable and trustworthy results by implementing measures for transparency and adhering to Guba and Lincoln’s standards. 20 Several strategies were implemented to enhance the credibility of the data. These included maintaining an ongoing dialogue between the researcher and the research topic and cross-checking with participants to deepen the understanding. In addition, 2 members of the research team (PhD in nursing and expert in qualitative research) independently examined the coded texts to establish reliability, with any discrepancies resolved through consensus among the researchers. To ensure verifiability, the researcher sought the input of an external observer experienced in qualitative studies. Lastly, sampling was conducted to achieve maximum variance, thereby enhancing the transferability of the findings.
Ethical Considerations
The study’s goals, methods, data confidentiality procedures, and voice recordings were explained in detail to the participants, who were also informed that their participation was voluntary. Both written and verbal informed consent were obtained. Participants were also given the assurance that their information would be kept private and that they could leave the study at any time without facing any repercussions.
Results
Participant Characteristics
The study included 13 clinical nurses with an average age of 34.7 years and an average work experience of 10.8 years. Due to distance, interviews with 3 nurses were conducted online (video call). Table 2 displays the participants’ profiles.
Demographic Characteristics of the Participants.
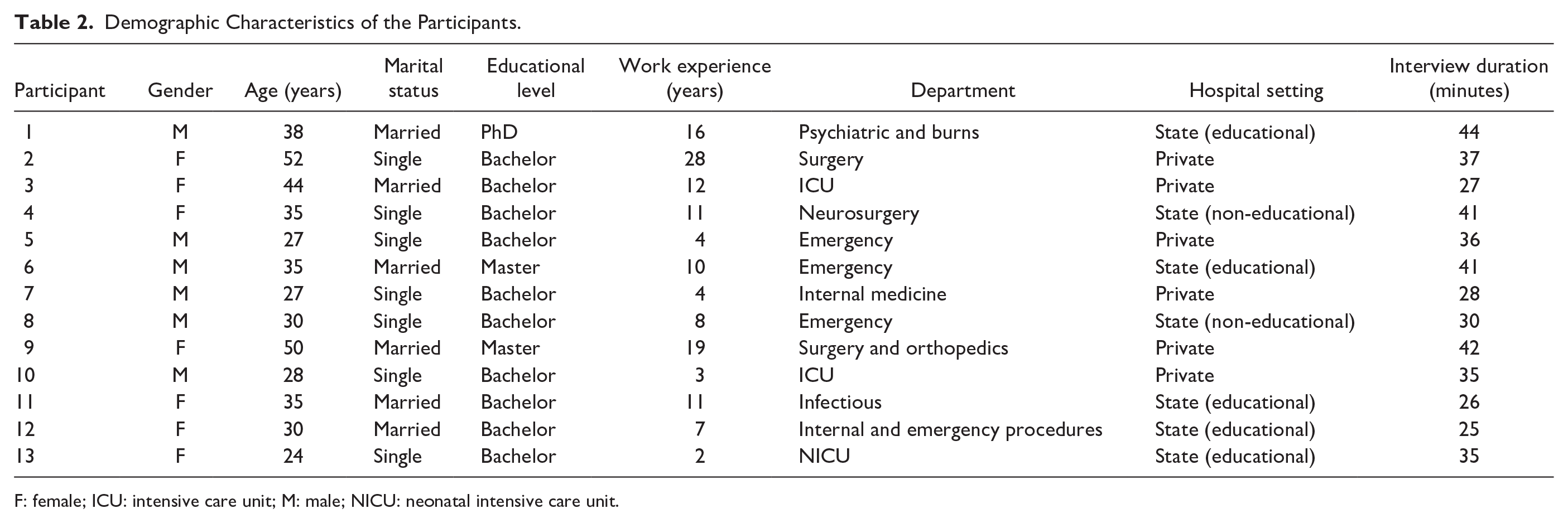
F: female; ICU: intensive care unit; M: male; NICU: neonatal intensive care unit.
Findings of Qualitative Analysis
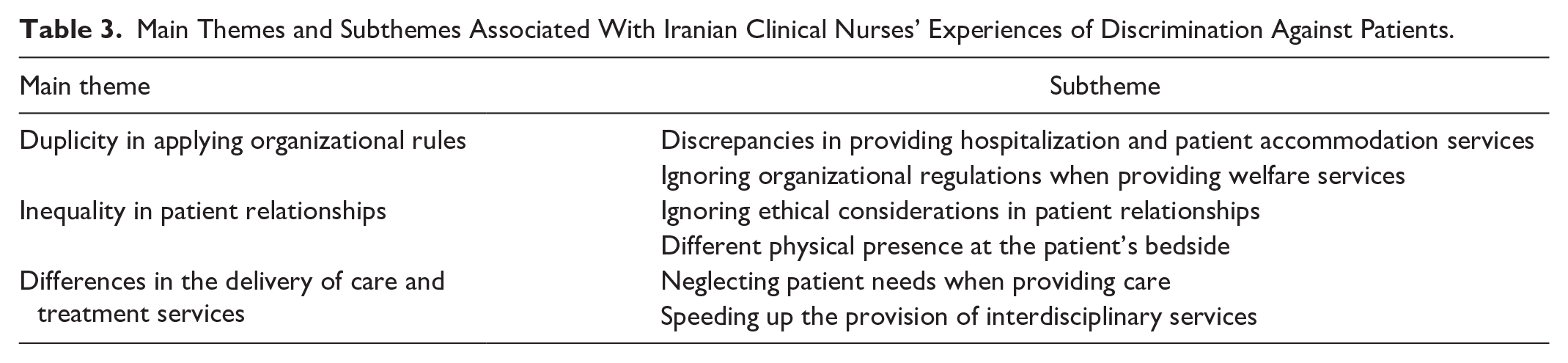
The data analysis led to the exploration of 3 main themes: (1) duplicity in the application of organizational rules, (2) inequality in communication with patients, and (3) different provision of care and treatment services. Under these 3 themes, we also identified 6 subthemes. For better understanding, we provide direct quotes from clinical nurses who participated in the research on these categories. The direction and confirmation of the findings are presented in Table 3.
Main Themes and Subthemes Associated With Iranian Clinical Nurses’ Experiences of Discrimination Against Patients.
Theme 1: Duplicity in Applying Organizational Rules
One common form of discrimination that affects patient care is the uneven application of organizational rules and professional standards. Nurses noted that certain factors, such as patient preferences, gender, age, and socioeconomic status, influenced the unfair allocation of patient accommodation services and welfare amenities. This category represents nurses’ deviation from equitable service provision and includes 2 subcategories: (a) Discrepancies in Hospitalization and Patient Accommodation Services and (b) Neglecting Organizational Regulations When Providing Welfare-Personal Services.
Subtheme 1a: Discrepancies in hospitalization and patient accommodation services
Clinical nurses have reported instances of favoritism in health care services where certain groups of patients receive better-quality care. These groups may include favorite patients (in this article, these patients include celebrity patients, urban patients, acquaintances, individuals of the opposite sex from nurses, and young people). For example, some nurses mentioned that the best ward beds are often allocated to patients in their favorite areas, and they are given priority for transfer to clinical wards or operating rooms. This practice not only perpetuates discrimination but also neglects the needs of other patients. One participant expressed concern about this issue, stating that it is unfair and can have negative consequences for patients who do not receive the same level of care. In this regard, 1 participant stated the following:
Unfortunately, there is discrimination in the ways nurses provide services to patients in their favorite areas, particularly in the field of hospitality services. Unlike other patients, favorite patients may be admitted to a VIP or isolation room or may be prioritized for surgery or transfer to an ICU. (P8)
Regarding providing more high-quality patient accommodation services to her patients, a nurse stated:
We had a patient who was specifically ordered by the hospital chief. Normally, we would give disposable clothes to all patients, but in this case, we provided the patient with ironed hospital clothes. We realized that this was discriminatory behavior. We also placed the patient in an isolation room and ensured that if their bed got dirty, we cleaned it immediately. (P6)
Participants in the study highlighted several issues related to discriminatory and substandard patient accommodation services. These included improper bed allocation, lack of prioritization for elective surgeries, and inpatient services being provided to patients from low economic and social backgrounds, the elderly, homeless patients, and those suffering from infectious diseases such as AIDS and coronavirus. One contributor mentioned a particularly concerning incident:
We had a 14-year-old girl who was susceptible to infection, had just been operated on, and was in an isolation room. That’s when one of the hospital’s supervisors came to the hospital with a cold, and the head of the emergency department took the patient out of the isolation room, and the hospital’s supervisor was admitted to the isolation room instead of her. (P5)
Subtheme 1b: Neglecting organizational regulations when providing welfare-personal services
Participants in this study reported instances where nurses disregarded the organizational regulations for favorite patients. Examples of such violations of organizational rules included allowing a patient access to a mobile phone despite hospital regulations, disregarding ward restrictions for certain patients, providing personal mobile phones to patients, giving personal phone numbers to patients by nurses, permitting unlimited and multiple-person visits to patients in intensive wards, and requesting physicians to expedite visits beyond their scheduled appointments. For instance, 1 nurse recounted, “We have a patient who is not allowed to have visitors, but because he was a friend of the hospital director. Whenever his companions came, we allowed them to enter the ward” (P2).
According to the participants, certain hospital rules were violated for specific patients. For instance, some patients requested visits from more experienced physicians instead of on-call physicians from their service as mandated by the hospital. One participant mentioned the following: “Once my brother came to my hospital. There was an anesthesiologist whom I didn’t accept, so I asked the best anesthesiologist to visit him, and his visit went very quickly” (P8).
Theme 2: Inequality in Patients’ Relationships
One of the main themes identified in this study regarding discriminatory care is the way communication and engagement with patients occur, including its manner, quantity, and quality. This theme includes 2 aspects: (a) Ignoring Ethical Considerations in Patients’ Relationships and (b) Differential Physical Presence at the Bedside.
Subtheme 2a: Ignoring ethical considerations in patients’ relationships
Nurses emphasized that one of their paramount responsibilities is to establish consistent and professional therapeutic relationships with all patients through ethical principles of nursing. They expressed their obligation to provide communication services to patients regardless of their illness, age, gender, or economic and social status. However, they noted that in clinical settings, communication is often inequitable. Two types of discrimination observed in this context include establishing a warm and intimate relationship with some patients (such as acquaintances, fellow citizens, young people, and individuals of the opposite sex) and a lack of communication with some patients (such as drug addicts, prisoners, and patients suffering from addictions or infectious diseases like AIDS and hepatitis). Examples of this discrimination include nurses prioritizing communication and establishing rapport with certain patients, such as a young social media blogger who neglects others. One nurse recounted:
A woman, who I think was less than 30 years old and was a [social media] blogger and was very pleasant, was hospitalized in our department, and I saw that all the nurses were talking to her, laughing, and trying to establish communication with her much more than normal patients. (P7)
Regarding under-routine communication or lack of communication with patients, most nurses stated that all hospitalized patients should be considered only 1 patient and ignore their status outside the hospital. However, contrary to this, there is discrimination against patients with low social levels. In this regard, a nurse stated the following:
In the infectious department, we have a series of patients who are brought from prison, and they have guards, and they do not have a good social status, and this patient was a criminal or had a serious crime, or whatever, both nurses and medical assistants did not have proper communication. They did not get along with them and looked at them with a very bad view. (P12)
Subtheme 2b: Differential physical presence at the bedside
Participants observed discrepancies in the physical presence of nurses at the bedside, with some receiving more attention and prompt responses to their needs than others. For instance, 1 nurse noted the following:
One of the nurses in our ward answered very quickly to the nursing calls of wealthy patients, but I saw that he was late with other patients, or we had a male nurse who answered the nursing call of a female patient earlier. (P9)
Moreover, some nurses displayed reluctance to attend to patients with infectious diseases, such as AIDS or hepatitis, resulting in minimal physical presence at their bedside. One participant recalled:
For HBS-positive patients, some nurses were saying out loud that you should be aware that HBS is positive, and many staff didn’t go up to this patient at all, whatever the patient shouted was useless, and it was like the patient himself would notice the discrimination he had with other patients. (P12)
Theme 3: Differences in the Delivery of Care and Treatment Services
Examples of discrimination in this part of the study show that this category includes 2 categories: (a) Neglecting the Needs of Patients in Providing Care and (b) Speeding Up the Provision of Interdisciplinary Services.
Subtheme 3a: Neglecting the needs of patients in providing care
Based on the results of the study, we can refer to provisions such as providing more routine nursing care, such as providing special training, performing nursing procedures (eg, prescribing medicines and painkillers, checking for vital signs, suction, gavage, and lab sampling), and observing sterile procedures in performing treatment procedures for favorite patients. For example, in the case of further observation of sterile procedures in performing nursing procedures, one of the participating nurses stated:
Our colleague was admitted for a laminectomy in our hospital. According to the protocol, we washed our hands before any procedure or touched him and wanted to change his dressing, we followed the sterile procedures more, and to prevent infection, we took care of infection more. (P3)
Another dimension of discriminatory treatment and training interventions to specific groups is the provision of less than normal care to some patients, which can be attributed to the lack of proper and timely injection of medications, lack of sterile observance, lack of proper training to imprisoned, homeless, addicted, infectious diseases such as AIDS, hepatitis, coronavirus, etc. In this regard, a nurse stated:
When you have an addicted patient or a patient with AIDS or hepatitis, especially in the case of invasive procedures, the nurse does not perform the nursing care correctly, for example, does not inject the drugs correctly, or does not give the drug at all. For example, in the case of infectious patients such as COVID patients, the nurse checked the patient’s vital signs less often and did not inject the drugs properly. (P5)
One of the other discriminatory cases mentioned by the nurses was the non-implementation of treatment orders or the incorrect implementation of medical services toward patients exhibiting exaggerated symptoms. In this context, a nurse stated that “There is also a lot of discrimination against patients exhibiting exaggerated symptoms, for example, nurses do not give the medicines prescribed for them, or they pour distilled water on them instead of narcotics” (P11).
One of the most common examples of discrimination mentioned by most participants is providing special education to some patients. In this context, a nurse working in the internal department stated:
In the case of the celebrity patient, I first introduced myself to him, oriented him more to the environment, and taught him in every field. Then I tried to prepare the patient for the operation. I gave him more information, then in cases where he was afraid, I tried to be with him more and give him peace, but I taught less than this to ordinary patients. (P9)
Subtheme 3b: Speeding up the provision of interdisciplinary services
Participants described samples of discrimination as performing special and out-of-turn paraclinical services (eg, MRI, Computerized Tomography scan); requesting faster preparation of laboratory test results; requesting special and out-of-turn physiotherapy for favorite patients; familiarity with nurses, opposite sex, and young patients; and not sending laboratory samples or not following up on lab test results of patients with addiction and homelessness, as well as for patients with brain death, alcoholism, and child labor. For example, a nurse stated:
Working for favorite patients, really customized, sending patient tests faster to the laboratory. All emergency tests were given in the first half hour. If a blood bag injection was needed and the patient’s hemoglobin was low, we would have prepared the patient’s blood bag faster. (P1)
In addition, regarding prioritizing paraclinical services for certain patients, a nurse in private hospitals stated, “For some patients, the care was much more accurate. We always took these patients to radiology first. CT and MRI were always the first for this, and these patients were always the priority for going to the operating room” (P3).
Discussion
This qualitative study explored clinical nurses’ experiences of discrimination against patients. One key finding of this study was the lack of consistency in the application of professional standards and organizational regulations. Although the primary goal of health care is to preserve or enhance health outcomes, the quality of care, which encompasses hospitality services, plays a critical role in improving health care delivery. Hospital hospitality services, comprehensive nursing care, and initiatives aimed at promoting comfort and well-being, all essential components of the nursing profession, are correlated. Discrimination in the provision of patient accommodation services by nurses can hurt the health of patients and their level of satisfaction with the care received, and there is a need for nurses to gain the necessary knowledge in this field. 21 It is recommended that healthcare facilities implement antidiscrimination training programs to mitigate instances of discrimination. These educational programs can help promote legal literacy, amend discriminatory laws and policies, and ensure legal protection for patients. 22 Furthermore, this problem is multilevel and systemic within hospitals, and it is not just a nursing issue; other healthcare staff members also require educational programs to be implemented, as many of the discriminatory actions that nurses take against patients are forced upon them by hospital administrators.
Another finding of this study examines how healthcare providers interact with different patient demographics. While some patients receive compassionate care, others, like those who are dealing with addiction, incarceration, patients exhibiting exaggerated symptoms, or mental health issues, often face hostile attitudes and a lack of rapport. Despite Iran’s multiethnic population and the unavoidable ethnic fragmentation in the healthcare system, discrimination in nurse-patient communication is not well-taught, which is concerning because interacting effectively with all patients, regardless of their personality and social characteristics, is a basic and essential professional skill that healthcare teams are expected to have. 23 For efficient decision-making and guaranteeing that patients’ values and objectives are fulfilled, a positive relationship between healthcare professionals and patients is essential. 24 A study by Appiah et al revealed that some nurses may discriminate against patients with lower socioeconomic backgrounds or those suffering from certain conditions. 25 The authors found that such nurses were less willing to communicate with these patients, whereas they tended to interact more with patients from affluent backgrounds. 25 When discrimination against patients occurs based on their social status, the nurse-patient relationship is disrupted and negatively affects care outcomes, and patient’s rights to share ideas and participate in their care planning are ignored. 26 The existence of such discriminatory relationships makes it necessary to adopt effective policies and hold relevant nursing training courses.
One notable finding of the study is the discrimination in the presence of nurses at the bedside. The presence of nurses is one of the vital aspects of nursing care that improves treatment outcomes, self-care, and patient satisfaction. 27 Nurses who are physically present with their patients reported that they are more confident in understanding their patients’ problems, beliefs, and wishes, allowing them to better tailor their care to each individual. 28 Many aspects of nursing care, including relationships with patients, physical examinations, spiritual care, and follow-up on the effectiveness of care are neglected when nurses are not present at the bedside of patients who are imprisoned, elderly, or of low economic and social status. This can harm patients’ health, so hospital managers are advised to focus more on this issue and reduce the incidence of this type of discrimination by determining the underlying cause of the issue and conducting training courses.
The findings of this research indicated that nurses in Iran may exhibit discriminatory behavior by expediting medical procedures (eg, medication administration, vital sign monitoring, suctioning, gavage, specimen collection, and diuresis assessment) for certain preferred patients while providing less comprehensive care to individuals of lower social standing. Consequently, this differential treatment may result in insufficient pain relief, misdiagnosis, and unfavorable health outcomes for affected patients. The results of a study by Rafii et al, which examined the development process of discriminatory nursing care, revealed that in discriminatory care, nurses may refuse to care for patients or provide care at the appropriate time or in the proper manner. This neglect leads to the patient being effectively ignored, which results in delayed recovery, absence of necessary care, and numerous physical and mental harm to the patients. 29
Another finding of this study is the discriminatory behavior exhibited by nurses toward individuals with infectious illnesses, including AIDS, hepatitis, tuberculosis, and COVID-19. This type of discrimination encompasses inadequate communication, insufficient physical care, failure to provide necessary education, and substandard or unethical execution of nursing protocols. The primary factor contributing to this discrimination is the negative perceptions of patients afflicted with such diseases. Discrimination against patients with AIDS has also been reported in other studies, and it has been suggested that implementing practices such as antidiscrimination training in medical centers can be effective.30,31 These educational programs promote legal literacy, amend discriminatory laws and policies, and ensure legal protection for these patients. 32 Although one of the reasons for this discrimination seems to be the fear of contracting these diseases, nurses should know that one of their key jobs is to care for these patients and that this fear may be addressed by following safety recommendations. There is evidence in the scientific literature that antidiscrimination training has been implemented to address various forms of discrimination and implicit bias in the healthcare sector. For instance, the Charter of Patients’ Rights in Iran emphasizes that healthcare services should be provided without any form of discrimination, including discrimination based on ethnicity, culture, religion, type of illness, or gender, for all patients, regardless of their condition. 15 The Charter of Patients’ Rights in Iran is a document designed to ensure the rights and protection of patients within the country’s care system. This charter is grounded in human values and underscores the equality and inherent dignity of all healthcare recipients. 33
Another result of this study was the acceleration of the provision of interdisciplinary services to some special patients. Limited medical resources and long waiting times to access these services force nurses to make such positive discrimination for specific patients and their relatives. The existence of such discrimination causes delays in providing paraclinical medical services for other patients and a lack of proper diagnosis, which causes patients to stay longer in medical centers and lose their trust in the healthcare system. 34 Although the findings from the analysis of nurses’ experiences did not directly address the state of the management system in healthcare, the findings show that while the Patients’ Rights Charter and nursing codes of ethics are designed to guide nurses’ performance, there is insufficient monitoring of the implementation of care standards by nurses. In this regard, a study by Hosseinabadi-Farahani et al in Iran showed that the lack of supervision by managers is one of the antecedents of discrimination in the healthcare system. 35 Therefore, hospital managers should have greater oversight over the training of the Patient Rights Charter and its implementation.
Limitations
This research explored nurses’ experiences of discrimination in nursing care in Iran and shed light on aspects of this issue that are often overlooked in quantitative analyses. The inherent limitations of any study should be acknowledged. The investigation was specifically contextualized within the health care system and societal norms of Iran. Therefore, similar studies should be replicated in diverse global contexts to enhance the generalizability of findings. It is imperative to recognize that discrimination poses ethical challenges, potentially leading some nurses to exhibit reluctance or discomfort in engaging with researchers, thereby potentially impacting the outcomes of the study. Consequently, these constraints and variations should be considered when interpreting the implications of the study.
Conclusion
Discrimination against patients is a significant issue that requires immediate attention. The findings of this study indicate that discriminatory behaviors are not limited to the provision of care but can also manifest in the physical and technological aspects of healthcare services, as well as in softer elements such as communication and attentiveness to patients. This study identified instances of discriminatory conduct by clinical nurses, providing valuable insights for improving practices and strategies in this field. To reduce nurses’ discrimination, interventions such as training programs, increased public awareness, and revisions to health care policies can be implemented. In addition, practical measures such as establishing structured reporting mechanisms for discriminatory incidents, incorporating antidiscrimination training into nursing curricula, and promoting mentorship programs to foster inclusive workplace environments should be considered to create a more equitable healthcare system.
Footnotes
Acknowledgements
The authors are grateful to the nurses who shared their stories.
Author Contributions
Aram Karimian, Afsaneh Sadooghiasl, Mitra Khoobi, Eesa Mohammadi and Anoshirvan Kazemnejad: conceptualization; investigation; writing—original draft; methodology; validation; visualization; formal analysis; data curation; writing—review and editing. Afsaneh Sadooghiasl, and Mitra Khoobi, Eesa Mohammadi and Anoshirvan Kazemnejad: supervision.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
Ethical approval was received from the Ethics Committee at Tarbiat Modares University under the ethics code IR.MODARES.REC.1402.017. All participants were provided with a plain language information sheet and given a verbal explanation of the aims of the study and what was required of them. Each participant provided written informed consent before commencing the study.
Statements and Declarations
Not applicable.
Data Deposition
Not applicable.