
Abstract
Objective:
Our aim in this study was to evaluate the effects of education provided to family caregivers of patients with heart failure (HF) on the caregiver’s contribution to the patient’s self-care and on the patient’s quality of life and symptoms.
Methods:
This study utilized a pretest-posttest intervention design and was conducted with 380 patients and family caregivers. Data were collected using the Caregiver Information Form, Patient Information Form, Caregiver Contribution to Heart Failure Self-Care Index (CC-SCHFI), Memorial Symptom Assessment Scale-Heart Failure (MSAS-HF), and the Minnesota Living with Heart Failure Questionnaire (MLWHFQ). After the preliminary interview, a pretest was administered to the patients and their caregivers. Then, caregivers were trained on HF. After the end of the education, the posttest was administered to the patients and their caregivers.
Results:
The difference between the mean (± SD) CC-SCHFI pretest (53.37 ± 1.73) and posttest (72.84 ± 1.08) scores was statistically significant (p < .001). The differences between patients’ MSAS-HF pretest (1.08 ± 0.39) and posttest (0.53 ± 0.25) and MLWHFQ pretest (49.00 ± 12.69) and posttest (39.00 ± 14.06) scores were statistically significant (p < .001). There was no significant correlation between the CC-SCHFI pretest scores of caregivers and the MLWHFQ and MSAS-HF pretest scores of patients, whereas a weak and significant correlation was found between the CC-SCHFI posttest scores of caregivers and the MSAS-HF posttest scores of patients (r = 0.161, p = .002).
Conclusion:
Supporting caregivers in HF through educational program may increase their contribution to patient care and improve patient outcomes.
Keywords
Heart failure (HF) is a chronic condition in which the heart cannot pump enough blood to meet the vital needs of the body. HF is a clinical condition that can occur due to many different causes and encompasses both symptoms and physical findings.1,2 There are ~15 and 5.7 million adults with HF in Europe and America, respectively. 3 By the end of 2022, the number of HF patients alive in Turkey was 1.8 million. 4
HF involves complex clinical treatment and care aimed at reducing long-term and recurrent hospitalizations and minimizing the symptoms of the disease. It is inaccurate to view HF as a singular pathological diagnosis. Rather, it is a clinical syndrome comprising cardinal symptoms (eg, breathlessness, ankle swelling, and fatigue) that may be accompanied by signs (eg, elevated jugular venous pressure, pulmonary crackles, and peripheral edema). 5 HF is a chronic and progressive disease, and the symptoms associated with it have a significant impact on the patient’s activities of daily living. 6 Studies have clearly demonstrated the importance of caregivers in managing HF patients’ medical treatment, increasing self-care, and improving symptom management and quality of life.6,7 Caregiver contribution to patient self-care is defined as the process by which the caregiver supports the patient in maintaining HF stability (caregiver contribution to self-care maintenance), monitoring symptoms (caregiver contribution to symptom monitoring and perception), and addressing symptoms (caregiver contribution to self-care management).7,8 These processes are interrelated and the caregiver’s contribution to the maintenance of self-care influences the caregiver’s contribution to the monitoring and perception of self-care, which in turn influences the caregiver’s contribution to self-care management. 7 When caregivers have adequate knowledge about the symptoms of HF, disease-related symptoms can be identified earlier and patient’s quality of life will improve.8,9
A systematic review reported that structured, goal-oriented, and professional educational interventions for caregivers of HF patients provide benefits for the caregiver and the patient. 10 Therefore, the education provided in this study used an educational program aimed at empowering family caregivers.
To date, a limited number of studies have focused on the outcomes of planned nursing education given to caregivers of patients with HF. 10 Studies, especially in Turkey, have focused on managing the symptoms of HF and improving the quality of life of patients, and caregivers have been neglected in this process.11-13 Therefore, the aim of this study was to evaluate the effects of planned education given to family caregivers of patients with HF on the contribution of the caregiver to the patient’s self-care and on the patient’s quality of life and symptoms.
Methods
Study Design
This study was conducted as a 1-group, pretest-posttest intervention in a university hospital in Ankara, Turkey. Patients were continuously cared for by the same family caregiver until the end of the study; non-primary caregivers, those who had been caring for the patient for <1 month, and formal caregivers (health professionals) were excluded.
Study Population
In this study, the sampling formula for a known population was used to determine the sample size, using the number of patients admitted to the hospital where the study was conducted with a diagnosis of HF in 1 year (27 072). As a result of the formulation given below, it was determined that the sample size should be 380 patients and 380 family caregivers with 95% confidence interval and 5% margin of error. 14

Between July 2018 and June 2019, face-to-face interviews were conducted with 380 patients and 380 family caregivers who were hospitalized with a diagnosis of HF, met the inclusion criteria, and agreed to participate in the study. The sample of this study consisted of patients who were older than 18 years, volunteered to participate in the study, were hospitalized in the cardiology ward, had a diagnosis of HF confirmed by a cardiologist, had no cognitive-psychiatric disorders in their medical history, and did not have a diagnosis of cancer. Caregivers needed to be able to read and understand Turkish, were older than 18 years, volunteered to participate in the study, had no cognitive-psychiatric disorders in their medical history, did not have significant hearing and speech impairment, and provided continuous personal care to the patient (caregiving period was at least 1 month). Non-primary caregivers (alternating) and formal caregivers (health care workers) were excluded. All HF patients with New York Heart Association functional classes (I, II, III, IV) were included in the study along with their caregivers. All participants gave written informed consent and were informed that they could withdraw from the study at any stage of the study. Patients and family caregivers who participated in this study were informed whether or not to participate in the study.
Data Collection
After informing the patient and caregiver about the study, the data of this study were collected with a Caregiver Information Form, a Patient Information Form, the Caregiver Contribution to Heart Failure Self-Care Index (CC-SCHFI), the Memorial Symptom Assessment Scale-Heart Failure (MSAS-HF), and the Minnesota Living with Heart Failure Questionnaire (MLWHFQ). Pretest data were collected simultaneously but separately by interviewing patients and caregivers. Data collection took an average of 20 minutes for each participant and was based on self-report through face-to-face interviews.
Data Collection Tools
The data collection tools used in the study consisted of forms and scales used separately for patients and caregivers. These tools used for patients and caregivers were used in both pretest and posttest.
Caregiver Information Form
This form was prepared by the researchers based on the literature in order to obtain information about the characteristics of the caregivers who participated in the study. Information collected included age, gender, degree of closeness to the patient, marital status, educational level, employment status, and whether there is a person or persons who help in care. 11
Patient Information Form
In this form, which was created by the investigators based on the literature, demographic variables such as age, gender, employment status, education level, marital status, and whether there were other cardiac patients in the family were included.12,13
Caregiver Contribution to Heart Failure Self-Care Index
The CC-SCHFI was developed by Vellone et al and the Turkish validity and reliability study was conducted by Akbıyık and Enç.11,15 The scale is a 4-point Likert-type and consists of a total of 22 questions. The higher the score obtained from the scale, the higher the contribution of the caregiver to the patient’s self-care. The CC-SCHFI is composed of 3 distinct scales. The first part, designated as “A,” encompasses 4 subdimensions that evaluate the management of symptoms, physical activity, adherence to medical treatment, and sodium intake control. These subdimensions are intended to assess the contribution of caregivers to the continuity of self-care in individuals with HF. The second part, “B,” focuses on the caregivers’ contribution to the patient’s self-care management. It comprises 2 subdimensions that evaluate autonomous and directive-dependent management. In part C, the caregiver’s trustworthiness is examined as a contributing factor to the patient’s self-care management, utilizing 2 subdimensions to assess advanced and basic-level trust, respectively. Cronbach’s alpha value of the scale is 0.82 in prior work. 11 In this study, Cronbach’s alpha value was found to be 0.30.
Memorial Symptom Assessment Scale-Heart Failure
The MSAS-HF was developed by Zambroski et al, and the Turkish validity and reliability study was conducted by Akdeniz and Özer. 12 The scale was designed to collect information about many aspects of 32 symptoms experienced by patients with HF in the previous week. Each symptom is assessed in terms of frequency, severity, and feelings of distress or discomfort. If a symptom is experienced, the patient describes the frequency and severity of the symptom on a 4-point Likert-type scale and the feeling of distress or discomfort on a 5-point Likert-type scale. The scale comprises 3 subdimensions: the physical subdimension, the psychological subdimension, and the HF subdimension. Cronbach’s alpha value of the scale was 0.92 in prior work. 12 In this study, Cronbach’s alpha value was found to be 0.82.
Minnesota Living With Heart Failure Questionnaire
The MLWHFQ was developed by Rector et al to measure the impact of HF on an individual’s quality of life. 16 The questionnaire consists of 21 statements examining 2 subdimensions: physical function and emotional. Its translation into Turkish, along with testing of validity and reliability, were performed by Aşık Özdemir. 13 The questionnaire items use a Likert-type scale to measure the physical and social functioning of HF. The highest possible score is 105. A lower score indicates a better quality of life. Cronbach’s alpha value of the scale is 0.85 in prior work. 13 In this study, Cronbach’s alpha value was found to be 0.82.
Booklet and Interventions
The literature search was conducted in PubMed, Embase, and the Cochrane Library databases. Following this, a search question defining the concepts was created and a list of terms was designed to represent them using terms relevant to the study hypothesis. The terms used were caregiver(s), family caregiver(s), informal caregiver(s), caregiver response, “patients and/or caregivers with incapacity,” “educational support,” and “caregiver education program.” After reviewing the relevant literature and brochures, an education booklet for caregivers of patients with HF was developed in accordance with the DISCERN (Quality Criteria for Consumer Health Information) measurement tool.10-13,17 The education booklet was sent via e-mail for the opinions of 5 academic nurses and 1 academic cardiologist who were experts in the field of HF and not from the same institution as the author. The experts evaluated the booklet in accordance with the DISCERN assessment-evaluation tool. 17 The booklet was finalized in line with the expert opinions. In the booklet, it was emphasized that caregivers should have information about the signs and symptoms of HF, drugs used in its treatment and their side effects, ways of coping with the problems that the disease may cause, use this information in the care of patients and know their legal rights. The colorful, readable, illustrated, and diagrammed booklet was distributed to caregivers at the beginning of the education.
First interview and education
Before the first interview, a pretest was administered to patients and caregivers who met the inclusion criteria. The caregivers were administered the Caregiver Information Form and the CC-SCHFI as a pretest. Similarly, the Patient Information Form, the MSAS-HF, and the MLWHFQ were administered to the patients as a pretest. Following the pretest application, the first interview and education session was conducted with the caregivers of each patient in the interview room determined for the planned education program. Each education session was conducted by a single researcher with a group of 10 people (caregivers of 10 patients) in a face-to-face format. A total of 38 different groups, each consisting of 10 caregivers of hospitalized patients, were formed simultaneously, and the education was given to these groups simultaneously. During the interviews, an educational booklet was used to educate caregivers about HF, including information on nutrition, exercise, symptom management, physical aspects of care, and disease-specific care. The duration of the education was ~45 to 60 minutes, and each group was interviewed face-to-face. Following the education, family caregivers were invited to share their experiences and challenges related to the disease. To facilitate the management of HF-related symptoms and to assess the physical, social, and psychological well-being of family caregivers, the researcher provided each family with a telephone number and informed them that they could contact (Figure 1).
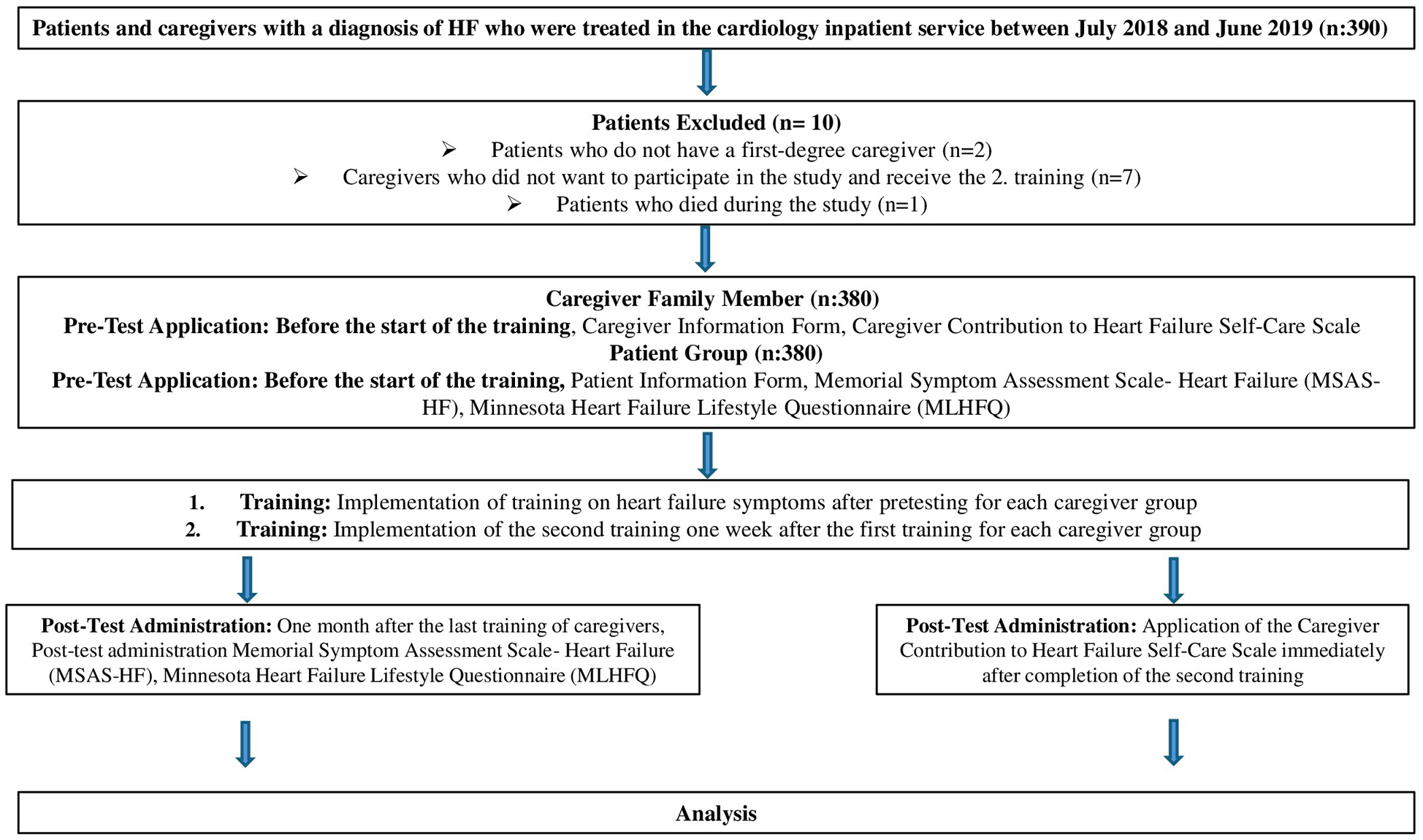
Study flow diagram.
Second interview and education
All family caregivers were contacted by phone, and the second interview was scheduled 1 week after the first education. The second interview lasted between 45 and 60 minutes and was conducted face-to-face in a meeting room with caregivers in each group. The content of the group education included preparation for discharge home, problem solving, what to do in emergencies, and psychosocial situations. Immediately after the end of the second education, a posttest was administered with the CC-SCHFI.
One month after the end of the second education of the caregivers, when the patient came to the hospital for control, the posttest was performed with the same scales applied in the pretest. In this process, the patient’s appointment date in the cardiology outpatient clinic was determined with the recommendation of each patient’s physician. Since the posttests of patients who did not show up for the appointment and patients who died during the study period could not be performed, these patients and their caregivers were excluded from the study (Figure 1).
Data Analysis
Data were analyzed in using SPSS version 23 (IBM Corp, Armonk, NY, USA) applying a 95% confidence interval and p < .05. The characteristics of the participants were analyzed using frequency and percentage analyses, and mean and standard deviation statistics were used in scale analyses. In order to evaluate the distribution of the research variables, kurtosis and skewness values were examined, and it was determined that they showed normal distribution.18,19 Considering the nature of the data, Student’s t test was used to compare the 2 groups and Pearson correlation analysis was used to examine the relationship between the scales.18,19
Ethical Considerations
Before starting the study, we obtained the approval of the Ankara University Health Sciences Ethics Committee (date: April 02, 2018; No.: 06-88) and written permission from the hospital where the study was conducted (date: June 05, 2018; No.: 1490). The study was conducted in accordance with the Declaration of Helsinki after obtaining written informed consent from the participating patients and their family caregivers.
Results
The mean age of caregivers was 56.0 ± 8.3 years, and 82.9% were female (Table 1). More than half of the caregivers (65.3%) were spouses of the patients. Most of the caregivers (93.4%) were married, and almost all (95.3%) had children; 36.6% of caregivers were primary school graduates, and 76.8% were not working. Among the caregivers, 13.9% stated that they received help during caregiving (Table 1).
Descriptive Characteristics of Family Caregivers (N = 380).
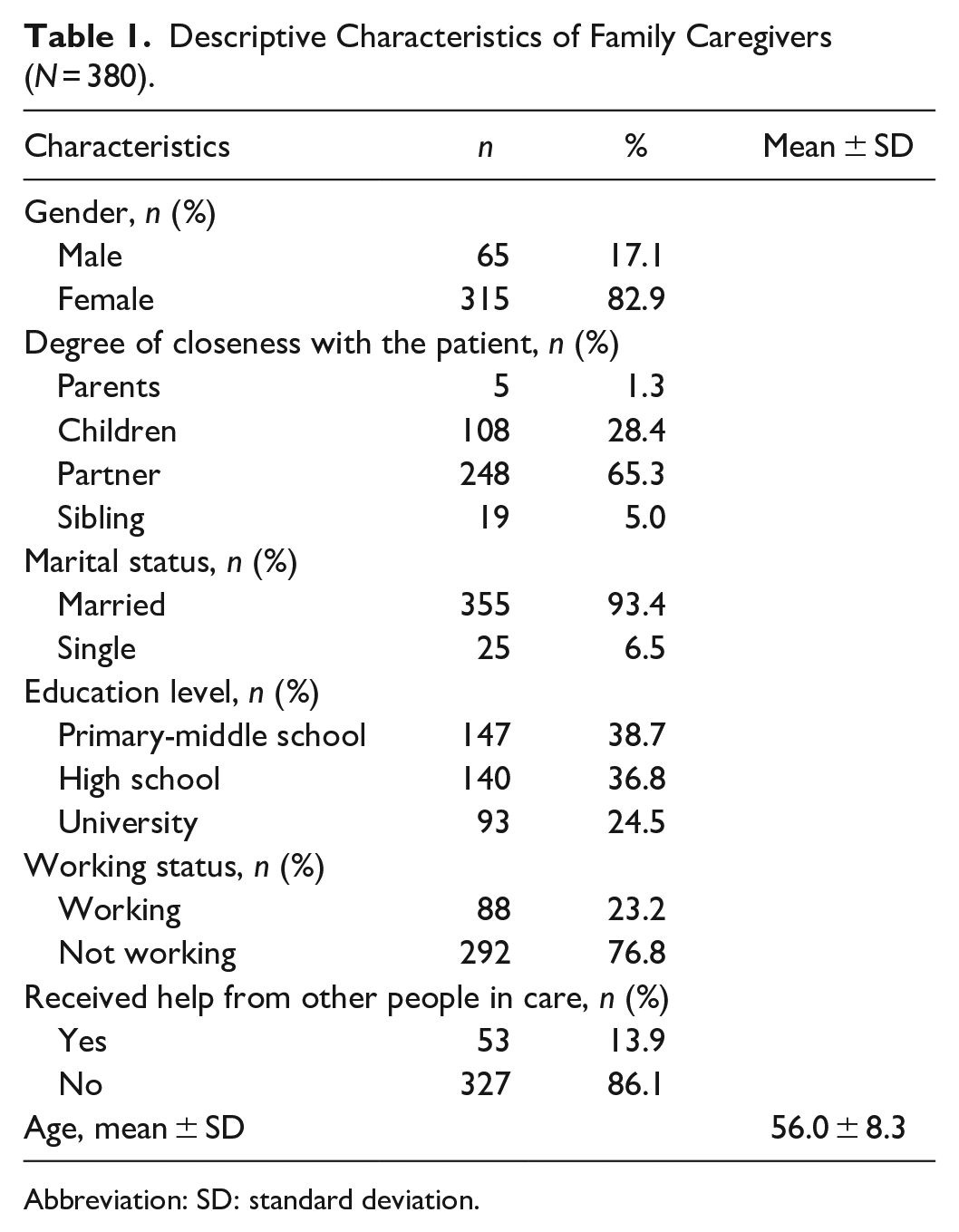
Abbreviation: SD: standard deviation.
The mean age of the 380 patients included in the study was 62.0 ± 10.3 years, and the majority (68.4%) were men. The education level of most of the patients was primary school and high school (37.9% and 36.1%), and 86.1% were not working. In the study, 89% of the patients were married. The rate of patients with other heart diseases in their family was 32.9% (Table 2).
Descriptive Characteristics of Patients (N = 380).
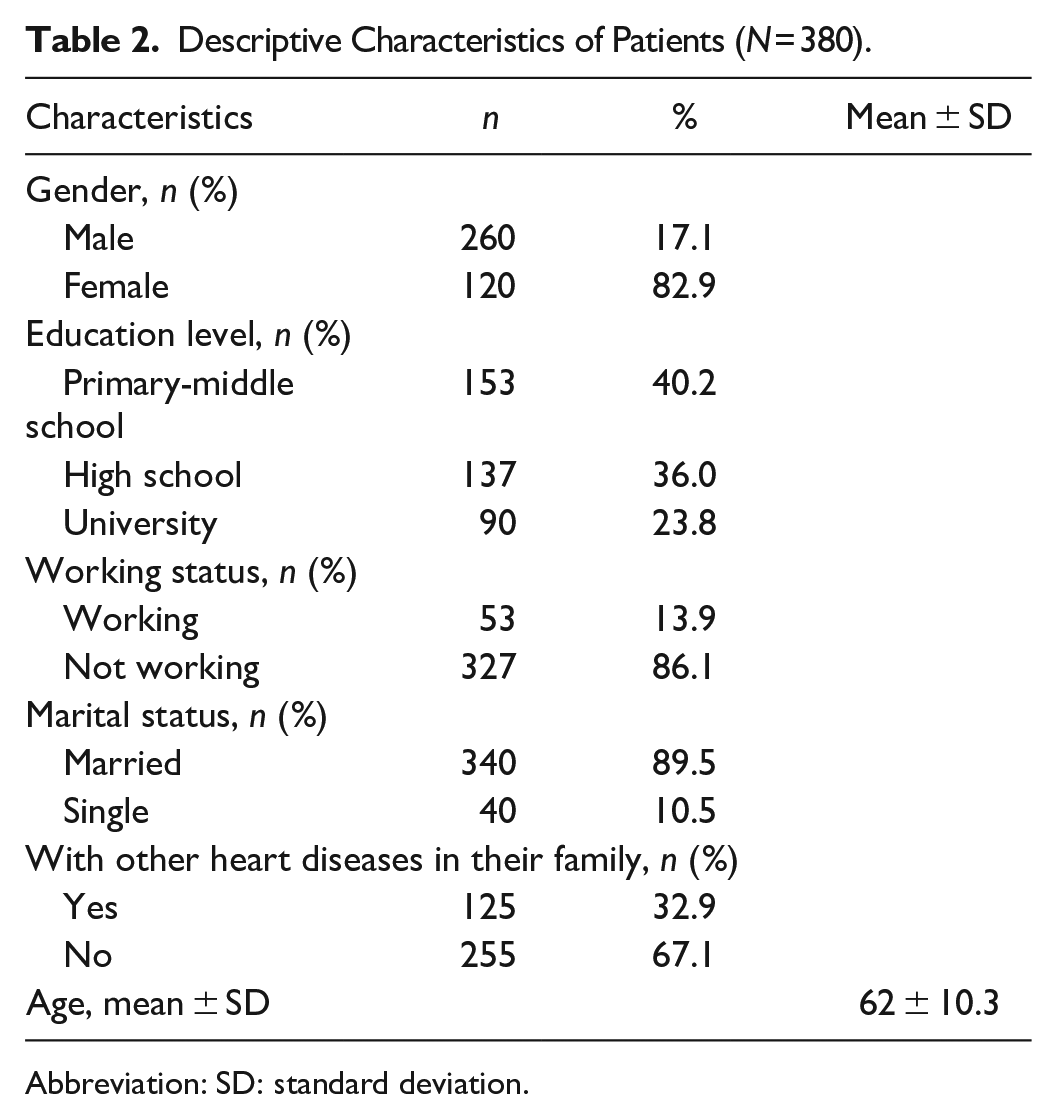
Abbreviation: SD: standard deviation.
The pretest and posttest total scores of CC-SCHFI are given in Table 3. The total score before the planned education was applied to the caregivers was lower than after the education. The difference between the pretest and posttest scores of caregivers was statistically significant (t = −217.7, p < .001).
Pretest-Posttest Total Scores of the CC-SCHFI (N = 380).
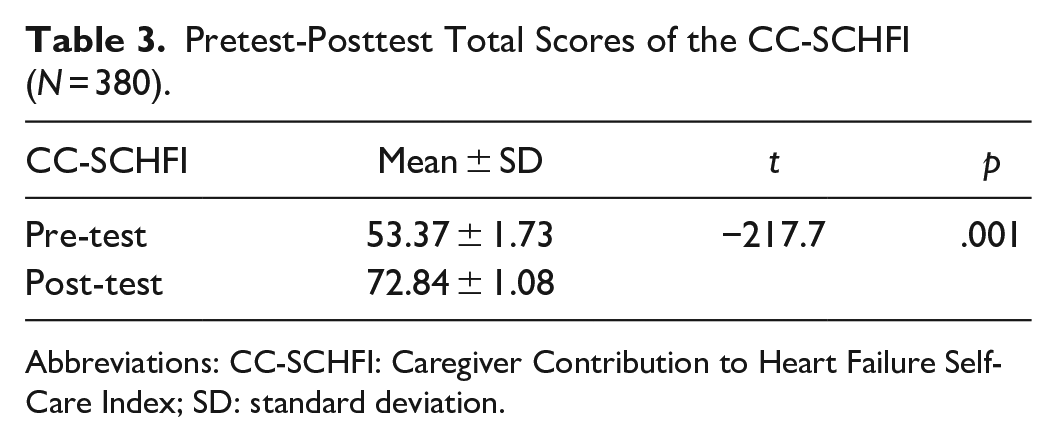
Abbreviations: CC-SCHFI: Caregiver Contribution to Heart Failure Self-Care Index; SD: standard deviation.
The pretest-posttest total scores of the patients’ responses on the MSAS-HF scale are shown in Table 4. When the total symptom scores of the patients were analyzed, it was found that the pretest scores were higher and the difference between the scores was statistically significant (t = 39.425, p < .001). The pretest-posttest total scores of the patients from the MLWHFQ before and after the education was applied to the caregivers are also shown in Table 4. When the total questionnaire scores of the patients were analyzed, it was found that the pretest scores were higher and the difference between the scores was statistically significant (t = 31.724, p < .001).
Pretest-Posttest Total Scores of the MSAS-HF and MLWHFQ (N = 380).
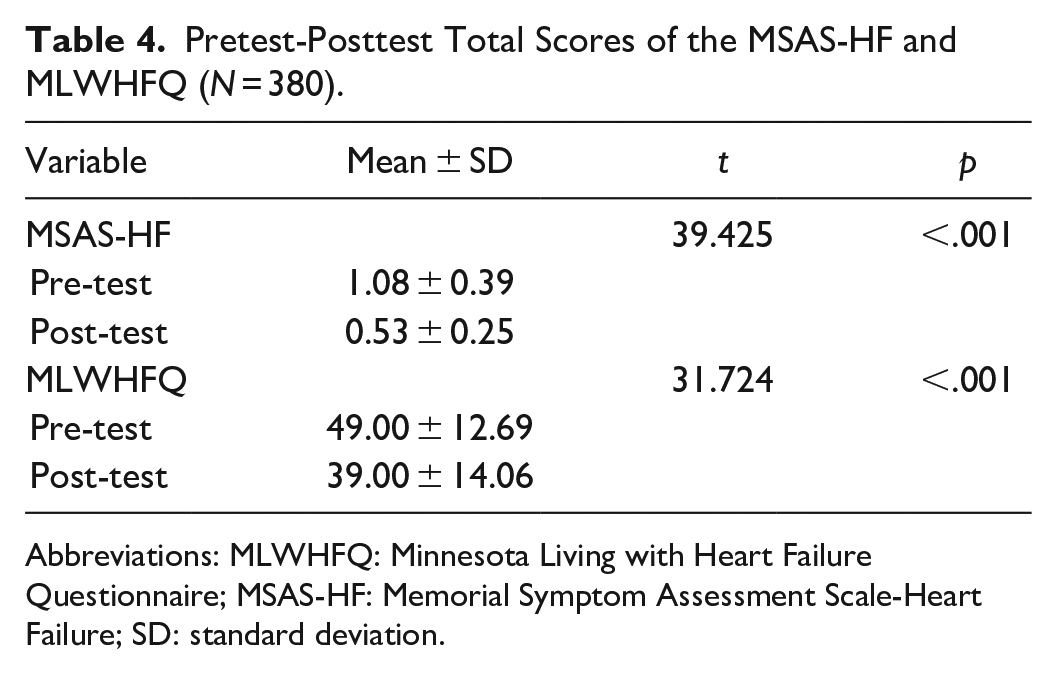
Abbreviations: MLWHFQ: Minnesota Living with Heart Failure Questionnaire; MSAS-HF: Memorial Symptom Assessment Scale-Heart Failure; SD: standard deviation.
There was no significant correlation between the pretest scores of the CC-SCHFI administered to the caregivers and the pretest scores of the MSAS-HF scale (r = 0.023, p = .655) and MLWHFQ (r = 0.098, p = .057) administered to the patients. There was no significant correlation between the posttest scores of the CC-SCHFI and the MLWHFQ posttest scores of the patients (r = 0.045, p = .378), while a significant weak correlation was found between the posttest scores of the MSAS-HF (r = 0.161, p = .002; Table 5).
Relationship Between the CC-SCHFI, MSAS-HF and MLWHFQ Pretest-Posttest Scores.
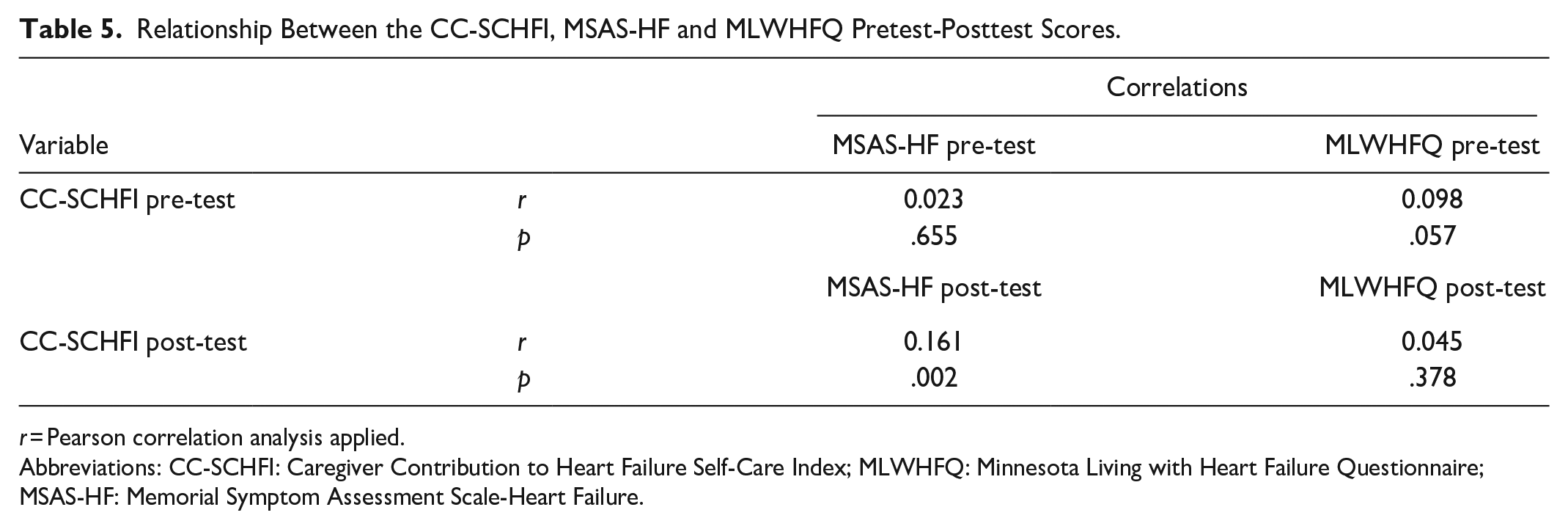
r = Pearson correlation analysis applied.
Abbreviations: CC-SCHFI: Caregiver Contribution to Heart Failure Self-Care Index; MLWHFQ: Minnesota Living with Heart Failure Questionnaire; MSAS-HF: Memorial Symptom Assessment Scale-Heart Failure.
Discussion
The aim of this study was to evaluate the effects of planned education given to family caregivers of HF patients on the caregiver’s contribution to the patient’s self-care and on the patient’s HF symptoms and quality of life. As a result of this study, it was found that planned education given to the caregivers of HF patients increased the contribution of caregiving and improved the quality of life by reducing the symptom burden of the patients. In the study, it was observed that the mean age of the caregiver group was 56.0 ± 8.3 years, the majority were women, more than half of them were married, and almost all of them had children. When the studies conducted with informal caregivers in the literature are examined, it is seen that women generally assume this role.20,21 Women are more likely to assume the role of caregiver in developing societies such as Turkey. 22 In another study, the results were similar to our study. 12 It was determined that the majority of the caregivers included in this study were primary school and high school graduates. This result may be thought to be due to the fact that the majority of caregivers were women. In Turkey, there are still problems regarding girls’ education. 22 Vellone et al showed that 9% of caregivers were university graduates. 23
The mean age of the 380 patients included in the study was 62 ± 10.3 years, and the majority were male. Almost half of the patients had primary school education, and almost all of them were unemployed. The proportion of patients with a family history of heart disease was lower than those without. The results were similar in studies in the literature.24,25 In other studies, it was found that more than half of the patients included in the sample had a family history of heart disease.26-28 It is thought that this may be related to genetic factors, lifestyle habits, and nutrition.
Caregivers’ total scores before the training were significantly lower than their total scores after the training. This is probably due to the fact that the training applied to caregivers increased caregiver contribution. In a study, it was shown that planned training applied to caregivers reduced the burden of caregiving and the quality of caregiving of caregivers increased after the training. 29 In other studies in the literature, it was determined that caregiving levels increased after the training applied to caregivers.10,11,23
In this study, after the education given to caregivers, it was found that the contribution of caregivers to patient self-care increased and, at the same time, the symptom scores of the patients decreased and their quality of life increased. Caregivers play a very important role in patients’ symptom management and disease recovery. With educational face-to-face training, caregivers can provide support in patient self-care and disease management and improve patient outcomes. 9 Buck et al found that the quality of life of patients with HF improved after caregiver education. 30 Similar results were obtained in other studies.31-35
In this study, no significant correlation was found between the pretest scores of caregivers and the pretest scores of patients. This may be due to the inability of patients and caregivers to assess the symptoms of HF and the need for planned training for caregivers. After the training, a significant but weak correlation was found between the posttest scores of caregivers and the posttest scores of patients. This may suggest that the training given to caregivers was effective in the management of HF and caregivers were more successful in evaluating symptoms, which positively affected the quality of life of patients. Rochmawati et al reported that the disease-related symptoms of the patient decreased and their quality of life increased with the training applied to caregivers. 31 It has also been shown in other studies that caregiver education positively affects the symptom management of patients and thus improves quality of life.9,13,34-36
Limitations
This study has several limitations. First of all, since the research design was a one-group pretest-posttest, there was no control group to compare the results, so the effect of other factors on the improvement seen due to the intervention could not be evaluated. Since the study was conducted in a single hospital, caution should be exercised when generalizing the results to larger populations. The cultural elements interpreted in the article may differ from those of the reader. Furthermore, the survey-based nature of the data collected imposes limitations on accuracy and potential recall bias, particularly given the low Cronbach’s alpha value for the CC-SCHFI in this study.
Conclusion
It is important to reduce the problems of caregivers in chronic diseases and to interact with caregivers in the treatment process. In this respect, nurses are in a key position in establishing a relationship with caregivers. Nurses should be able to evaluate the behaviors of caregivers and make behavior change interventions for them. Especially when caregivers are educated about the disease and can manage the symptoms related to the disease, the burden of care provided to the patient will decrease and the symptom control and quality of life of the patients will increase. As a result of this study, it was concluded that planned education applied to caregivers was effective in alleviating the symptom burden felt by patients and improved their quality of life. It was concluded that planned education applied to caregivers also reduced the burden of caregiving on caregivers.
Footnotes
Acknowledgements
We thank all patients and caregivers who took part in the study. This article is a condensed form of the first author’s doctoral thesis (dissertation) from Ankara University. (This study was produced from the PhD thesis.)
Author Contributions
Conception: ET, TB; design: ET, TB; supervision: ET, TB; fundings: ET; materials: ET; data collection ET; analysis and interpretation: ET; literature review: ET, TB; writing the article: ET; critical review: TB.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki after obtaining the approval of the Ankara University Health Sciences Sub Ethics Committee (date: April 02, 2018; Ethics Committee No.: 06-88), written permission from the hospital where the study was conducted (date: June 05, 2018; No.: 1490), and written informed consent from the participants.