
Abstract
Background:
Childhood obesity has emerged as a significant public health issue globally, with one-quarter of obese children living in Africa. Maternal factors have been linked with childhood obesity, yet there is limited research in Ghana.
Objective:
This scoping review examined maternal factors associated with childhood obesity in Ghana.
Methods:
This review was conducted using the framework by Arksey and O’Malley. The strategy involved searching electronic databases (PubMed, Web of Science, and Embase) and reference lists of relevant literature. Additional searches were performed using Google Scholar. Keywords, including maternal factors, childhood obesity, and Ghana, with their synonyms and related Medical Subject Headings (MeSH) terms, were combined using Boolean operators. Peer-reviewed articles investigating maternal factors in relation to obesity in children in Ghana were included.
Results:
The scoping review included 11 studies conducted between 2012 and 2022 with 8101 children between 4 and 17 years old. The prevalence of childhood obesity was between 2.3% and 21.2%. Higher socioeconomic status was consistently associated with a higher risk of childhood obesity. Several studies also found a positive association between maternal education and childhood obesity. Other maternal factors, including BMI and empowerment, have been less frequently studied.
Conclusion:
Contrary to results from the developed countries, Ghanaian children from higher socioeconomic backgrounds and with more educated mothers are more prone to obesity, highlighting the need to specifically target these families in obesity prevention and intervention strategies.
Childhood obesity has emerged as a significant public health issue globally. 1 The World Health Organization (WHO) reported that 340 million children and adolescents aged 5 to 19 years were affected by overweight and obesity in 2019, with one-quarter of these children living in Africa. 2 In Ghana, Mogre et al 3 found that 17% of children aged 5 to 14 years were obese. Lartey et al 4 found a combined prevalence of overweight and obesity among children aged between 9 and 15 years to be nearly 50%. Overweight and obesity prevalence among schoolchildren in the Tema Metropolitan area were 26% and 21%, respectively. 5 Notably, Ghana has shown a relatively high prevalence of childhood obesity compared to other African countries. 6 In 2014, the obesity prevalence among children under 5 was 2.6% in Ghana, compared to 1.8% and 1.1% in Nigeria and Burkina Faso, respectively. 7 Similarly, in 2013, among adolescents aged 15 to 19, Ghana reported an obesity prevalence of 13.0%, while Togo and Côte d’Ivoire reported 1.9% and 4.0%, respectively.
The consequences of childhood obesity are profound. Childhood obesity is associated with an increased risk of asthma, sleep disturbances, cardiovascular disease, and type 2 diabetes.8,9 Furthermore, obesity is linked to low self-esteem, increased depressive symptoms, and increased body dissatisfaction in children.10,11 Additionally, individuals with obesity in childhood often continue to struggle with excess weight into adulthood,2,9,12 leading to an elevated risk of cardiovascular diseases, hepatic impairment, diabetes, cancer, and premature death.13-15 These chronic conditions require long-term medical care, significantly increasing healthcare costs, straining already limited healthcare systems, and reducing access to care for others.16,17 Furthermore, adults with obesity frequently experience diminished productivity due to chronic illness, absenteeism, and early retirement. 18 These outcomes underscore the urgent need for early prevention and intervention strategies to mitigate the long-term health and economic burdens of childhood obesity.
Numerous risk factors have been linked to childhood obesity, including eating behaviors, nutritional intake, physical activity, and sedentary behavior. 19 Among these, family socioeconomic status (SES) and maternal factors are key upstream determinants that shape the broader environment in which children grow and develop.20,21 These factors influence food availability, physical activity, health literacy, and access to healthcare. Lower SES, often characterized by limited income, poor access to nutritious foods, and lower parental education, can expose children to obesogenic environments.22,23 However, in the urban areas in Ghana, rising income levels have led to increased consumption of processed foods24,25 and sedentary behavior, 26 suggesting that higher SES may paradoxically contribute to a greater risk of childhood obesity in Ghana. Maternal education also plays a critical role in shaping children’s health behaviors. Higher maternal education is associated with improved health literacy, which supports better decision-making around children’s diet and physical activity.27-29 Additionally, maternal obesity, a growing concern in Ghana, has been linked to childhood obesity30,31 potentially through genetic predisposition and shared behaviors, such as sedentary lifestyles and ultra-processed food consumption. 32 Cultural perceptions, such as viewing overweight children as signs of prosperity, may further contribute to the risk of childhood obesity, particularly in low-income households. 33
Many studies have investigated the association between maternal factors and childhood obesity in Africa, such as maternal education, SES, and maternal obesity. Studies conducted in Nigeria, 34 Kenya, 35 and Ethiopia 36 have reported that higher maternal education and/or SES are positively associated with childhood obesity and overweight. These findings contrast with results from developed countries, where higher maternal education and/or SES are typically associated with a reduced risk of childhood obesity.37-40 Maternal obesity has also been found to be associated with the risk of childhood obesity in African countries.35,41,42 Several maternal factors have been linked to childhood obesity in Africa. 1 However, despite the high prevalence of childhood obesity, research on this topic in Ghana remains relatively limited. Therefore, this scoping review explored which maternal factors have been associated with childhood obesity in Ghana to date.
Methods
This scoping review followed the steps of the framework by Arksey and O’Malley, 43 which entails identifying the research question, identifying relevant studies, selecting studies, charting the data, and summarizing and reporting the results.
Identifying the Research Question
We aimed to answer the following research question: What maternal risk factors are associated with childhood obesity in Ghana? In this review, maternal risk factors were defined as biological, behavioral, and socioeconomic characteristics or conditions of the mother that may influence a child’s risk of developing obesity through genetic, epigenetic, behavioral, and environmental pathways.
Identifying Relevant Studies
The review strategy involved a comprehensive search of electronic databases and reference lists of relevant literature. A thorough search was conducted in PubMed, Web of Science, and Embase, with additional searches using Google Scholar. PubMed, Web of Science, and Embase were chosen for their extensive coverage of public health and clinical research. Google Scholar was included to capture potentially relevant articles not indexed in traditional databases. This multifaceted approach was conducted to reduce publication bias and ensure inclusion of diverse and contextually relevant studies. Additionally, hand-searching of citations and reference lists from the included studies was performed to capture relevant articles that might be missed during the initial search. Keywords, including maternal factors, childhood obesity, and Ghana, along with their synonyms and related MeSH terms, were combined using Boolean operators (“AND” and “OR”) to ensure an inclusive search. The search strategy in PubMed was developed and then adapted for use in other databases. Aligned with the Joanna Briggs Institute’s Population, Concept, and Context framework, 44 the target population for this review was children aged <18 years and their mothers. The concepts considered were childhood obesity and maternal factors, while the context was studies conducted in Ghana (Supplemental Appendix).
Inclusion and Exclusion Criteria
The inclusion criteria for this scoping review were peer-reviewed articles published in English that investigated (1) maternal risk factors, (2) obesity in children aged <18 years, and (3) studies conducted in Ghana. Articles were excluded from this review if they were dissertations, systematic reviews, meta-analyses, narrative reviews, opinion articles, editorials, conference presentations, case studies, webinars, and clinical presentations. Systematic reviews, meta-analyses, and narrative reviews were excluded because this review aimed to synthesize findings from primary research articles.
Study Selection
Two authors (E.D. and K.G.A.) independently conducted the literature search, study selection, and data extraction based on the inclusion criteria. Discrepancies were resolved through author discussions and consensus. All relevant articles were selected based on their titles and abstracts. Duplicate articles were removed. The full texts of articles that met the inclusion criteria were retrieved and reviewed for a final inclusion decision, as shown in Figure 1.
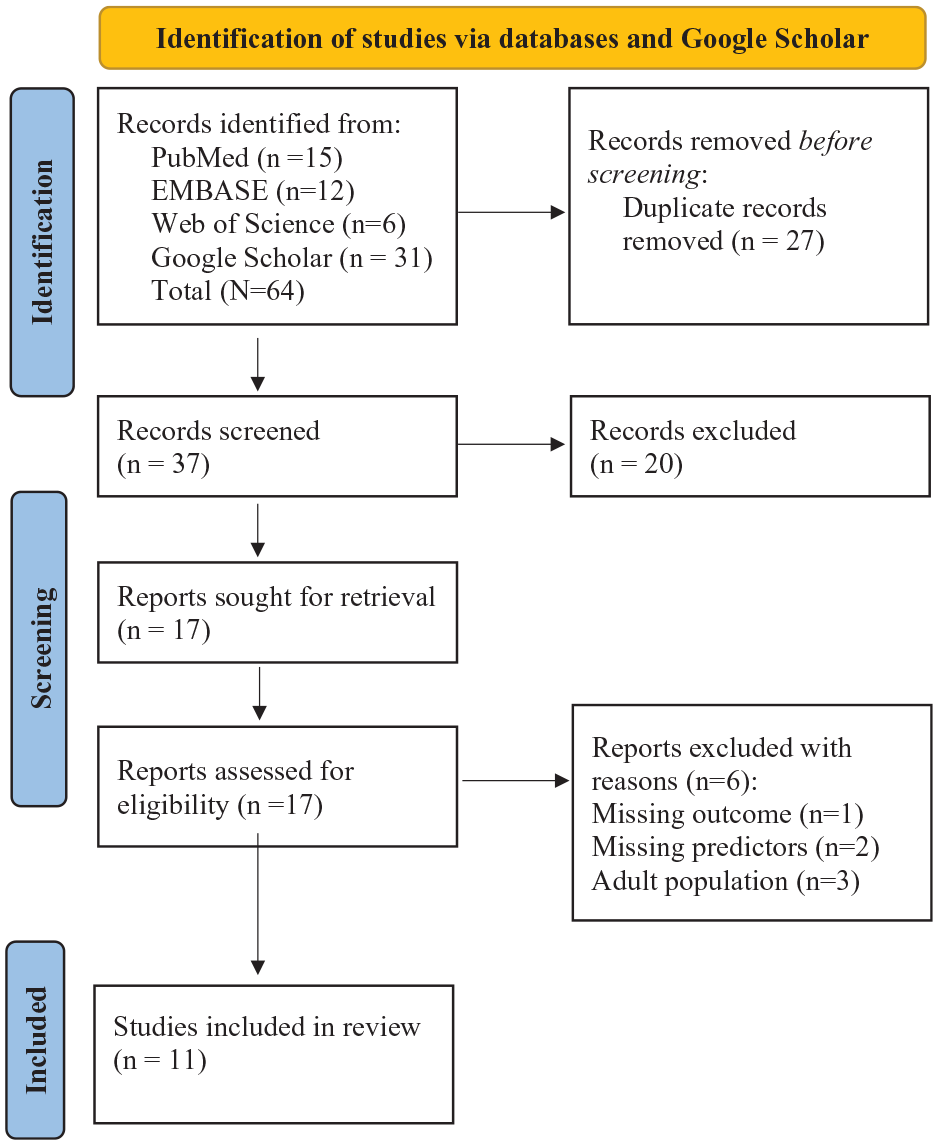
Flowchart.
Charting the Data
Two authors (E.D. and K.G.A.) independently used a standardized data extraction form to identify variables related to the research questions (Table 1). The data extraction form was pretested with 2 articles to ensure its appropriateness. Information was extracted on study characteristics, including authorship, year of publication, study design, sample size, age, maternal factors, and prevalence of childhood obesity. Discrepancies were resolved through discussion and consensus. As a scoping review is an iterative process, the data extraction form was refined and updated in response to emerging findings. All extracted data were thoroughly inspected for accuracy, and any inconsistencies and errors were addressed. Data synthesis was primarily narrative. Meta-analysis was not conducted due to the varying age groups examined across studies.
Main Findings From Included Studies.
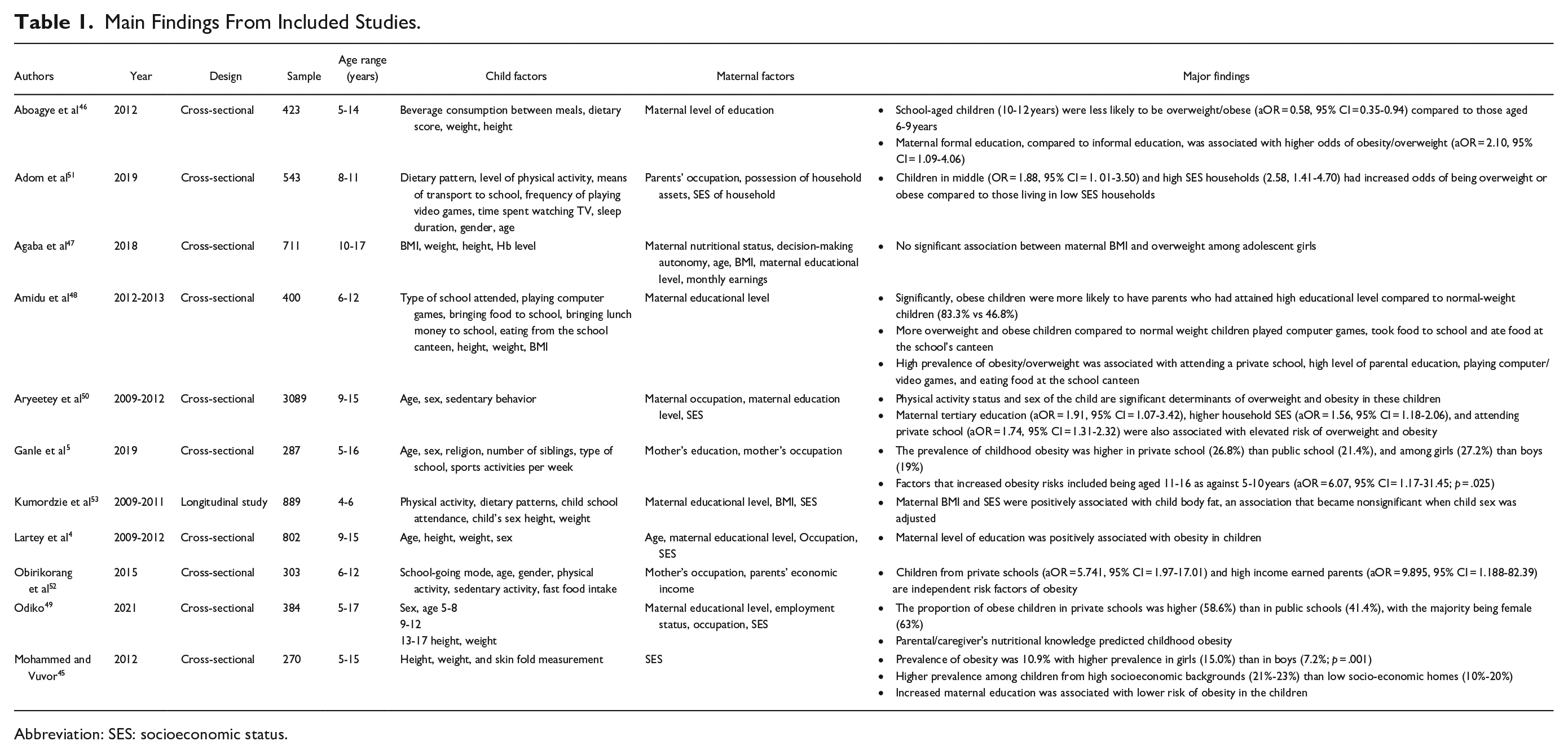
Abbreviation: SES: socioeconomic status.
Collating, Summarizing, and Reporting the Results
Study characteristics and types of research
The scoping review included 11 studies with 8101 children between 4 and 17 years old. The sample size of the individual studies ranged from 270 to 3089 children. The included studies explored between 1 and 6 maternal risk factors related to childhood obesity. Ten of the studies were cross-sectional studies,4,5,45-52 while 1 study was a cohort study. 53 Nine studies were conducted in urban areas4,5,45,48-53 and 2 in the rural communities46,47 of Ghana.
Prevalence of childhood obesity in Ghana
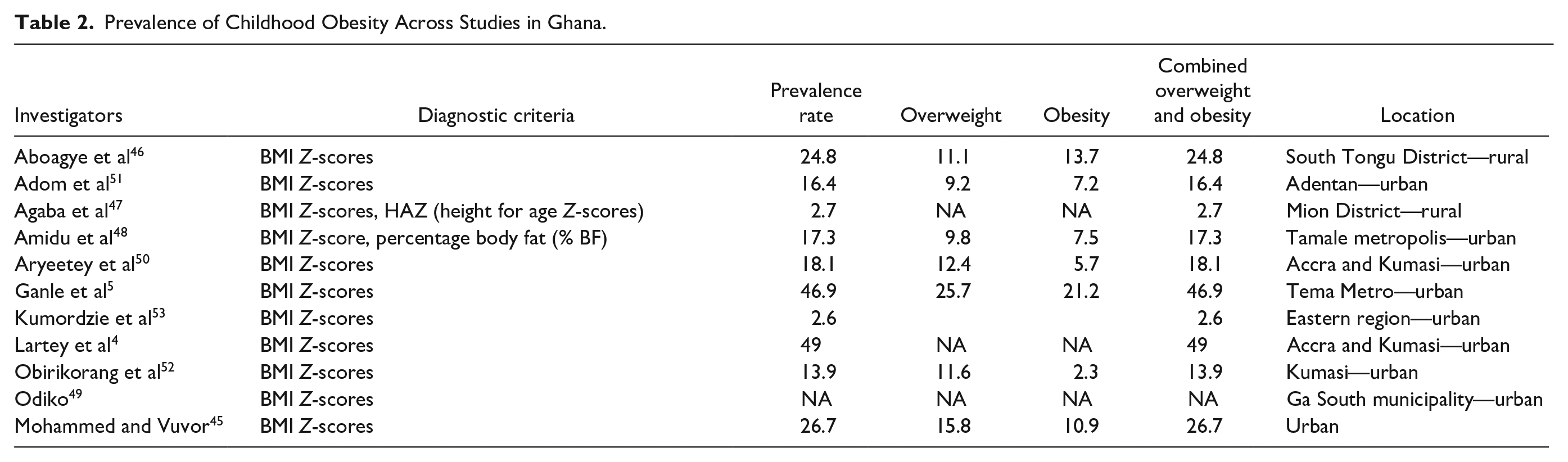
Body mass index for the children’s age and sex (BMI Z-scores) were used to determine the weight status of each child across the studies according to the following cutoffs defined by the WHO 54 : For children aged <5 years: obesity = BMI Z-score > +3 SD, overweight = +2 SD < BMI Z-score ≤ +3 SD, and “normal” weight = −3 SD < BMI Z-score ≤ +2 SD; for children aged 5 years and above: obesity = BMI Z-score > +2 SD, overweight = +1 SD < BMI Z-score ≤ +2 SD, and “normal” weight = −2 SD < BMI Z-score ≤ +1 SD. The prevalence of childhood obesity from the studies in this scoping review ranged between 2.3% 52 and 21.2% 5 (Table 2). Most of the studies45,46,48-51 reported the overall prevalence of childhood obesity but did not report the prevalence by age categories. Aboagye et al 46 reported age-specific differences in the risk of childhood obesity, finding that children aged 10 to 12 years were 42% less likely to be obese than those aged 6 to 9 years (adjusted odds ratio [aOR] = 0.58, 95% CI = 0.35-0.94). In contrast, Ganle et al 5 reported that children aged 11 to 16 years had a higher risk of obesity compared to those aged 5 to 10 years (aOR = 6.07, 95% CI = 1.17-31.45; p = .025). Five studies also examined sex differences in childhood obesity prevalence, yielding inconsistent findings.5,45,50-52 Two studies found a significantly higher prevalence in female participants compared to males.45,50 Another 2 studies5,52 also observed a higher prevalence in females participants, though this difference was not statistically significant. Conversely, Adom et al 51 reported a higher but nonsignificant prevalence among male participants.
Prevalence of Childhood Obesity Across Studies in Ghana.
Maternal factors related to obesity among children
Maternal education, SES, BMI, and empowerment have been assessed for their associations with childhood obesity in Ghana. Nine studies assessed maternal education.4,5,45-50,53 Six studies found a positive association between higher maternal educational levels and childhood obesity.4,46-48,50,53 In contrast, 2 studies reported a negative association between maternal education and childhood obesity,45,49 while 1 study found no significant association. 5 Maternal SES was examined in 7 studies. Participants’ household assets4,45,50,51,53 or average monthly income levels49,52 were used to measure SES for the studies under consideration. Five studies found a positive association between the middle and high SES groups and childhood obesity,45,50-53 while 2 studies4,49 found that SES was not significantly related to childhood obesity. Maternal BMI was assessed in 2 studies.47,53 Kumordzie et al 53 identified a positive relationship between maternal BMI and childhood obesity, whereas Agaba et al 47 found no significant relationship. Another maternal factor assessed was empowerment through decision-making autonomy. 47 Agaba et al found no association between maternal decision-making autonomy and overweight/obesity in adolescent girls.
Discussion
In the current review, most included studies employed cross-sectional designs, with only 1 longitudinal study. The reliance on cross-sectional designs in Ghana may be partly attributed to insufficient research funding and support. The UK Department for International Development 55 reported that funding for research and development in Ghana is low, with only 0.4% of the country’s gross domestic product allocated to research. Additionally, there is a disproportionate distribution of studies between urban and rural areas, with more research conducted in urban settings. This focus is likely due to the higher prevalence of childhood obesity among children living in cities and urban areas.56,57 However, including both rural and urban populations in the same studies would provide a more comprehensive comparison of prevalence rates. Also, longitudinal studies would be beneficial for monitoring trends in childhood obesity in the urban and rural areas to determine whether rates are stable, increasing, or decreasing.
The prevalence of obesity among children in this review differed vastly among studies, although they used similar obesity cut-off criteria. The prevalence of childhood obesity ranged from about 6%, as reported by Aryeetey et al, 50 to about 21% by Ganle et al. 5 When combining overweight and obesity, the prevalence rates showed an even wider range, from about 3% 53 to 49%. 4 The vast difference in prevalence across the studies might be partially explained by the varied geographical locations,56-58 type of schools, 5 family SES,59,60 and urban or rural settings.61,62 Therefore, nationwide survey studies with random sampling strategies are needed to estimate the rate of childhood obesity in the population in the future.
Several maternal factors related to childhood obesity have been assessed. Of the 9 studies assessing maternal education, 6 identified a positive association between maternal education and childhood obesity,4,46-48,50,53 while 2 found a negative association.45,49 Based on the sample sizes and the number of studies, higher maternal education might be associated with an increased risk of childhood obesity in Ghana, which is consistent with findings in other African countries.34-36,59 In contrast, in developed countries, higher maternal education is typically associated with a reduced risk of childhood obesity.37,38,40,63 The level of education of mothers can affect their perceptions of health care and living habits. 27 Often, those with high education levels are more likely to promote healthy lifestyles in their children by choosing a balanced and healthy diet, 28 a wider variety of food consumption, 29 and sufficient intake of fruits and vegetables. 64 However, many employed mothers may have limited time to cook and instead provide more processed foods for their children in Ghana. While home cooking is associated with healthier dietary patterns and a reduced risk of obesity, 65 employment can pose a challenge to regular home-cooked meals.66,67
Similarly, regarding the maternal SES, 5 studies found an association between the middle and high SES groups and an increased risk of childhood obesity.45,50-53 The results are consistent with those from other developing countries,68-70 but not from the developed countries.37,63,71,72 Similar to maternal education, Choukem et al 56 have suggested that the positive association between childhood obesity and higher SES could be due to increased sedentary behaviors and unhealthy food intake, such as using motorized transportation instead of walking, and spending long hours watching television, and accessibility to packaged foods high in sugars and saturated fats, which are more affordable to these families.
Two of the studies investigated the relationship between maternal BMI and childhood obesity, with inconsistent findings. However, in a systematic scoping review of obesity among children in sub-Saharan Africa, the researchers found that all 6 studies included in the review reported a positive correlation between maternal obesity and the risk of childhood obesity. 73 Other previous studies also reported this positive relationship.38,74-77 Since mothers are mostly responsible for how food is prepared and served in Ghana, their eating habits may affect the nutritional status of children and other family members. There is also a misconception among some Ghanaian people that obesity signifies good living and affluence. 33 Cultural beliefs that associate obesity with prosperity persist, particularly among older generations, despite growing public health efforts to reframe obesity as a health risk. Consequently, mothers who hold this belief may view their own and their children’s excessive weight gain as a sign that they are well-nurtured and nourished.
The relationship between maternal empowerment through decision-making autonomy and childhood obesity has also been investigated. The researchers found no association between maternal decision-making autonomy and overweight/obesity among adolescent girls. 47 While mothers with greater autonomy often manage household food budgets, this autonomy may lead to prioritizing calorie-dense, less nutritious foods, particularly among those who hold misguided cultural beliefs, which can potentially increase the risk of obesity among children. However, other studies argue that women’s involvement in household decision-making is crucial for promoting diverse diets and improving their children’s nutritional outcomes.78,79 Hence, further research is needed to clarify the nuances between maternal decision-making autonomy and childhood obesity in Ghana.
Strengths and Limitations
This review summarizes research articles conducted in Ghana, contributing to the current understanding of maternal factors that increase the risk of overweight and obesity among children in Africa. However, the search was limited to peer-reviewed articles published in English; hence, articles published in any other language are not included. Also, we could not conduct a meta-analysis due to the age differences among the different studies.
Conclusion
This review synthesized the current evidence from 11 published articles on maternal factors associated with childhood obesity in Ghana. Most studies were cross-sectional and conducted in urban areas between 2012 and 2022 and reported a wide range of childhood obesity rates. Therefore, nationwide longitudinal surveys with random sampling in the future would offer a more accurate and comprehensive estimation of the prevalence of childhood obesity in Ghana. Contrary to the findings in developed countries, Ghanaian children from higher socioeconomic backgrounds and with more educated mothers are at a greater risk of obesity. These findings highlight the importance of targeting childhood obesity interventions toward families at higher risk. Future research should employ mixed-methods and longitudinal designs to better disentangle the complex interplay of cultural, socioeconomic, and biological factors. Such approaches will help identify effective strategies to reduce childhood obesity while remaining sensitive to the local contexts.
Supplemental Material
sj-pdf-1-wjn-10.1177_01939459251359377 – Supplemental material for Maternal Factors Related to Childhood Obesity in Ghana: A Scoping Review
Supplemental material, sj-pdf-1-wjn-10.1177_01939459251359377 for Maternal Factors Related to Childhood Obesity in Ghana: A Scoping Review by Emmanuel Dapilah, Kofi Gyasi Agyei and Ying Meng in Western Journal of Nursing Research
Footnotes
Author Contributions
Emmanuel Dapilah conceived, designed, and drafted the study, conducted the literature search, screened articles, and extracted and synthesized the relevant information. Kofi Gyasi Agyei conducted the literature search, article screening, data extraction and synthesis, and drafting of the article. Ying Meng assisted with the design, drafting, and critical revision of the article. All authors have approved the final article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
This was a review study. No primary data were collected from human participants for this work. Institutional Review Board/Ethics Committee Review and informed consent were not required.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.