
Abstract
Background:
(Pre-)frailty is a state of heightened multidimensional vulnerability. Therein, (pre-)social frailty and (pre-)physical frailty are common subtypes, often coexisting and synergistically increasing risks of adverse outcomes.
Objective:
We aimed to compare the effectiveness of an exercise intervention among community-dwelling (pre-)physically frail older adults by baseline (pre-)social frailty status.
Methods:
This was a secondary analysis of a stepped-wedge cluster randomized trial evaluating a 12-week exercise intervention among 149 community-dwelling (pre-)physically frail older adults, with 3 follow-up visits at the 0-week, 12-week, and 24-week postintervention. Intervention effectiveness was examined within subgroups by baseline (pre-)social frailty status (non-[pre-]social frailty: n = 47; [pre-]social frailty: n = 102) using multilevel linear regression.
Results:
The non-(pre-)social frailty group exhibited immediate and persistent treatment responses across most outcomes. The (pre-)social frailty group showed improvements in physical frailty (all time points), cognitive function (0-week postintervention), depressive symptoms (all time points), social frailty (score: 0-week and 12-week postintervention; status: all time points), and quality of life (physical: all time points, mental: 0-week and 12-week postintervention). The (pre-)social frailty group had greater immediate improvements in fear of falling, depressive symptoms, and social frailty scores and status than the non-(pre-)social frailty group, but their improvements in social frailty score were less persistent at the 24-week postintervention.
Conclusions:
Older adults with (pre-)physical frailty who had comorbid (pre-)social frailty experienced effective improvements in fewer outcomes and less persistent gains in certain outcomes than their counterparts. Interventions should incorporate social support components to ensure comprehensive and lasting effectiveness for this population.
Trial Registration:
Chinese Clinical Trial Registry (ChiCTR2100041981).
Keywords
Introduction
Frailty is a prevalent condition among older adults, which is characterized by a heightened susceptibility and an increased risk of mortality when exposed to stressors, with a prevalence of 10.3% among older adults in Chinese communities.1,2 Pre-frailty, an intermediate stage between robustness and frailty, affects about 38.8% of this population and also predisposes them to adverse outcomes including disability, hospitalization, and death.2,3 Frailty has been recognized as a multidimensional concept that encompasses physical, psychological, and social components, 1 of which physical frailty is investigated most and is associated with falls, disability, hospitalization, and mortality.4,5 Exercise interventions have proven effective in reversing (pre-)physical frailty (which includes [pre-]physical frailty and physical frailty), by reducing muscle inflammation, stimulating anabolic processes, and enhancing muscle mass and function. 6 These physiological improvements ultimately lead to better health outcomes in older adults. 7 Nevertheless, social influence and dynamics could impact the improvements in and persistence of exercise, thus influencing the effectiveness of exercise interventions. 8 This impact requires further explorations among older adults with (pre-)physical frailty to identify the most vulnerable population and develop targeted interventions to maximize benefits.
Social frailty is another subtype of frailty that encompasses social influence and dynamics. 9 It refers to a state of vulnerability in individuals resulting from the depletion or loss of social resources, social behaviors, social activities, and self-management capabilities necessary to meet fundamental social requirements. 9 Social frailty is associated with numerous adverse outcomes, including poor physical performance, reduced activities of daily living (ADLs), decreased cognitive function, depression, and mortality.10-12 Pre-social frailty, an early stage of social frailty, manifests as early signs of social disengagement or reduced participation. Pre-social frailty can also lead to negative outcomes such as cognitive impairment, depression, diminished vitality, disability, and mortality.13,14 (Pre-)social frailty includes pre-social frailty as well as social frailty.
A reciprocal relationship exists between (pre-)physical frailty and (pre-)social frailty. 15 Older adults with (pre-)physical frailty are less likely to be physically active and participate in outdoor social activity, which may contribute to (pre-)social frailty. 16 Meanwhile, the low levels of social activity, social participations, and poor social relationships associated with (pre-)social frailty can have a negative impact on physical function, thus leading to (pre-)physical frailty. 17 Moreover, (pre-)physical frailty and (pre-)social frailty often coexist, possibly due to shared mechanisms, including the bidirectional interaction between physical capacity and social functioning, 18 as well as the aging-related etiological pathways as proposed by the geroscience model. 19 Critically, the co-occurrence of (pre-)social frailty and (pre-)physical frailty appears to have synergistic detrimental effects. Older adults with both conditions, compared with those with either condition alone, face substantially elevated risks of adverse outcomes, including falls, disability, and mortality. 11 However, it is scarcely investigated whether the additive adverse effects resulting from the coexistence of (pre-)social frailty and (pre-)physical frailty would influence the effectiveness of behavioral intervention among community-dwelling (pre-)physically frail older adults.
Our previous study verified the effectiveness of a theory-driven exercise intervention among community-dwelling (pre-)physically frail older adults, 20 which was developed by integrating the Health Belief Model (HBM), the Theory of Planned Behavior (TPB), and the Health Action Process Approach (HAPA). It has shown positive results in improving physical and psychosocial functioning, as well as the quality of life (QoL) in this population. 20 However, given the close association between (pre-)social frailty and high risks of adverse outcomes, as well as the worsening consequence of the coexistence of (pre-)social frailty and (pre-)physical frailty, (pre-)social frailty is a factor that may significantly affect the outcomes of exercise interventions among (pre-)physically frail older adults. 21 Therefore, this post-hoc analysis aimed to explore whether (pre-)social frailty influences the effectiveness of the exercise intervention. Specifically, we would examine how the exercise intervention works across different groups of (pre-)physically frail older adults with or without baseline (pre-)social frailty.
Methods
Study Design and Participants
The parent trial’s design, including sample size determination, randomization, blinding procedures, and intervention details, has been previously published in full detail. 20 The parent trial obtained approval from the institutional review board (no: IRB00001052-20094) and was registered on www.chictr.org.cn (no.: ChiCTR2100041981). All (pre-)physically frail older adults provided their written informed consent before their involvement in the study. This research employed a stepped-wedge cluster randomized trial (SW-CRT) design. The study was carried out from January to November 2021 and involved (pre-)physically frail older adults from 6 communities in a county located in central China. Communities were eligible if they had no previous or ongoing intervention programs and had at least 50 older adults. The 6 communities were randomly divided into 3 clusters. In this SW-CRT, the intervention was introduced to the clusters sequentially (Supplementary Figure S1). Initially, the clusters were in the control period, when participants continued their normal daily activities. Then, each cluster transitioned to the exercise intervention at a randomly assigned time point, with a 12-week interval between each transition. This design ensured that all clusters eventually received the intervention. 22
The inclusion criteria for participants were as follows: (1) being (pre-)physically frail (FRAIL score ≥1) 23 ; (2) being 60 years of age or older; and (3) having the ability to walk independently. Older adults were excluded if they met any of the following criteria: (1) suffering from severe hearing or visual problems; (2) having severe cognitive impairment (Short Portable Mental Status Questionnaire [SPMSQ] score ≥8) 24 ; (3) having contraindications to exercise, such as poorly controlled hypertension or diabetes; or (4) currently participating in other intervention programs.
Due to the nature of this behavioral intervention and the fact that measuring exercise adherence could reveal group allocations, it was not possible to blind the participants, intervention deliverers, and outcome assessors. Nevertheless, the data analysts were kept unaware of the randomization results. The sample size calculation method for the parent trial was previously reported, 20 and a total of 149 participants were enrolled in this study.
The exercise intervention in this study was developed by integrating the HBM, the TPB, and the HAPA to improve the adherence to this exercise program (Supplementary Figure S2). The HBM and the TPB were integrated by combining their shared motivational constructs, including attitudes and perceived behavioral control. The gaps in each theory were addressed by incorporating subjective norms from the TPB into the HBM and adding perceived threat and barriers from the HBM into the TPB. Finally, the HAPA was incorporated to bridge the intention-behavior gap through action and coping planning. This 12-week exercise intervention consisted of 2 main components: one component aimed at changing beliefs in exercise to promote adherence, and the other provided exercise instructions. The intervention for beliefs in exercise utilized behavior change techniques to promote exercise adherence. 25 It was implemented in the first week, the second week, and then every other week. The exercise instruction component included both aerobic training and resistance training. Each type of exercise session lasted ~25 minutes and was carried out at a moderate intensity 3 times a week throughout the 12-week intervention period. The exercise intervention was implemented by trained researchers in a group-based, face-to-face format at community centers for the first time, with attendance restricted exclusively to study participants. Thereafter, participants were instructed to independently perform the prescribed exercises in a home-based setting for the rest of the time. To ensure intervention fidelity, trained researchers regularly reviewed the session-by-session protocol and attended biweekly group supervision meetings led by the principal investigator. Participants were instructed to assess their adherence to the prescribed exercise throughout the 12-week intervention using a Numerical Rating Scale (NRS), according to their actual situations. The scale ranged from 0 to 10, with 0 representing no adherence to the exercise requirements and 10 representing complete adherence. More in-depth information about this intervention can be found in previous publications.20,26
Measurements
Primary and secondary outcome data were gathered at baseline, as well as at the 0th, 12th, and 24th week after the intervention. Supplementary outcomes such as the dropout rate, exercise adherence, and adverse events were collected at the 0-week, 12-week, and 24-week postintervention. To ensure data collection quality, data collectors received training on study objectives, content, methods, and techniques employed in the data collection process. The duration for outcome collection was ~30 to 40 minutes.
The primary outcomes consisted of frailty and frailty-related characteristics, namely, muscle mass, muscle strength, and physical performance. Frailty was evaluated using the Chinese version of the FRAIL scale. 23 This scale ranges from 0 to 5, with 0 indicating a robust status, 1 representing pre-frailty, and 2 or above denoting frailty. 23 Higher scores on this scale reflect greater frailty. Moreover, frailty statuses (ie, robustness, pre-frailty, and frailty) were also compared across the 2 subgroups. Muscle mass was measured through bioelectrical impedance analysis (Tanita BC-611 device; TANITA Corporation, Maeno-Cho, Itabashi-ku, Tokyo, Japan). 27 Muscle strength was measured by handgrip strength. 27 As for physical performance, the Short Physical Performance Battery (SPPB) 28 was used to assess lower extremity function, while the Timed Up and Go (TUG) test29,30 evaluated ambulation and dynamic balance. The SPPB score ranges from 0 to 12, with higher scores suggesting that the lower extremity function is better. The TUG test was timed in seconds, where less times indicate superior ambulation and dynamic balance.
Secondary outcomes included physical, psychological, and social well-being, as well as QoL of (pre-)physically frail older adults. Regarding the physical well-being, ADLs were assessed via the Katz Index, 31 and instrumental ADLs (IADLs) were measured using the Lawton scale 32 ; fear of falling was evaluated with the Short Falls Efficacy Scale-International (short FES-I). 33 As for psychological well-being, cognitive function was assessed by the SPMSQ, 24 and depressive symptoms were measured by the 5-item Geriatric Depression Scale (GDS-5). 34 In terms of social well-being, social frailty was evaluated by the HALFT (Help, pArticipation, Loneliness, Financial and Talk) scale. 12 QoL was measured through the 12-Item Short Form Health Survey, with the Mental Component Summary (MCS) indicating mental QoL and the Physical Component Summary (PCS) reflecting physical QoL. 35 Specifically, higher scores on the short FES-I, SPMSQ, and GDS-5 imply more fear of falling, cognitive impairment, and depressive symptoms, respectively, while higher scores on the other assessment tools suggest better health status. In this post-hoc analysis, (pre-)physically frail older adults were subgrouped according to their baseline (pre-)social frailty levels as determined by the HALFT scale. 12 The HALFT scale consists of 5 items: inability to help others, limited social participation, loneliness, financial difficulty, and not having anyone to talk to. 12 The scale score ranges from 0 to 5 points; a score of 0 is considered nonsocial frailty, 1 to 2 is considered pre-social frailty, and a score of ≥3 indicates social frailty. 12
Supplementary outcomes included exercise adherence, which was evaluated via the NRS. 36 Higher scores on this scale indicated better adherence. Adverse events were recorded by researchers, including injury, falls, and death.
Statistical Analysis
Intention-to-treat (ITT) analyses were conducted, with missing data addressed through multiple imputation techniques. Additionally, the full analysis set, including participants completing all follow-up assessments without missing data, were conducted as sensitivity analyses. Baseline characteristics, dropout rates, exercise adherence, and adverse events across subgroups were compared using independent sample t-tests or Mann-Whitney U-tests for continuous variables, and chi-squared or Fisher’ s exact tests for categorical variables, utilizing SPSS 24.0 (IBM Corp, Armonk, NY, USA).
A multilevel linear regression model was employed using Mplus 7.0 (Muthen & Muthen, Los Angeles, CA, USA) to assess the influence of baseline (pre-)social frailty on the effectiveness of the exercise intervention, comparing outcomes against their control statuses across subgroups. The Bonferroni correction was applied to account for multiple primary outcomes, distributing the overall α level equally among the primary endpoints. Given that there were 5 primary outcomes (FRAIL score, muscle mass, handgrip strength, SPPB, and TUG), the adjusted critical α was set at a 2-sided p value of .01 (.05/5). The practical significance of the intervention effects over time within subgroups was quantified through local effect size calculations (Cohen’s f2) using SAS 9.2 (SAS Institute Inc., Cary, NC, USA), with Cohen’s f2 values categorized as trivial (<0.02), small (≥0.02), moderate (≥0.15), and large (≥0.35). 37 Differences between subgroups were analyzed through the interaction of the intervention with baseline (pre-)social frailty. Furthermore, a generalized linear mixed model was employed using Stata 17.0 (StataCorp LLC, College Station, TX, USA) to evaluate changes in frailty status (robust status = 0, pre-frailty = 1, frailty = 2) and (pre-)social frailty (non-[pre-]social frailty = 0, pre-social frailty = 1, social frailty = 2). Except for within-group differences in primary outcomes (continuous form), p values for other within-group comparisons and all between-group differences were calculated as 2-sided, with a significance threshold set at .05.
Results
Baseline Characteristics
The parent trial enrolled 149 (pre-)physically frail older adults (aged 68.2 ± 5.6 years, 58.4% female; Table 1 and Supplementary Figure S3). These (pre-)physically frail older adults were divided into 2 subgroups based on their baseline (pre-)social frailty: the non-(pre-)social frailty group (n = 47, 31.5%) and the (pre-)social frailty group (n = 102, 68.5%).
Baseline Characteristics of Participants.
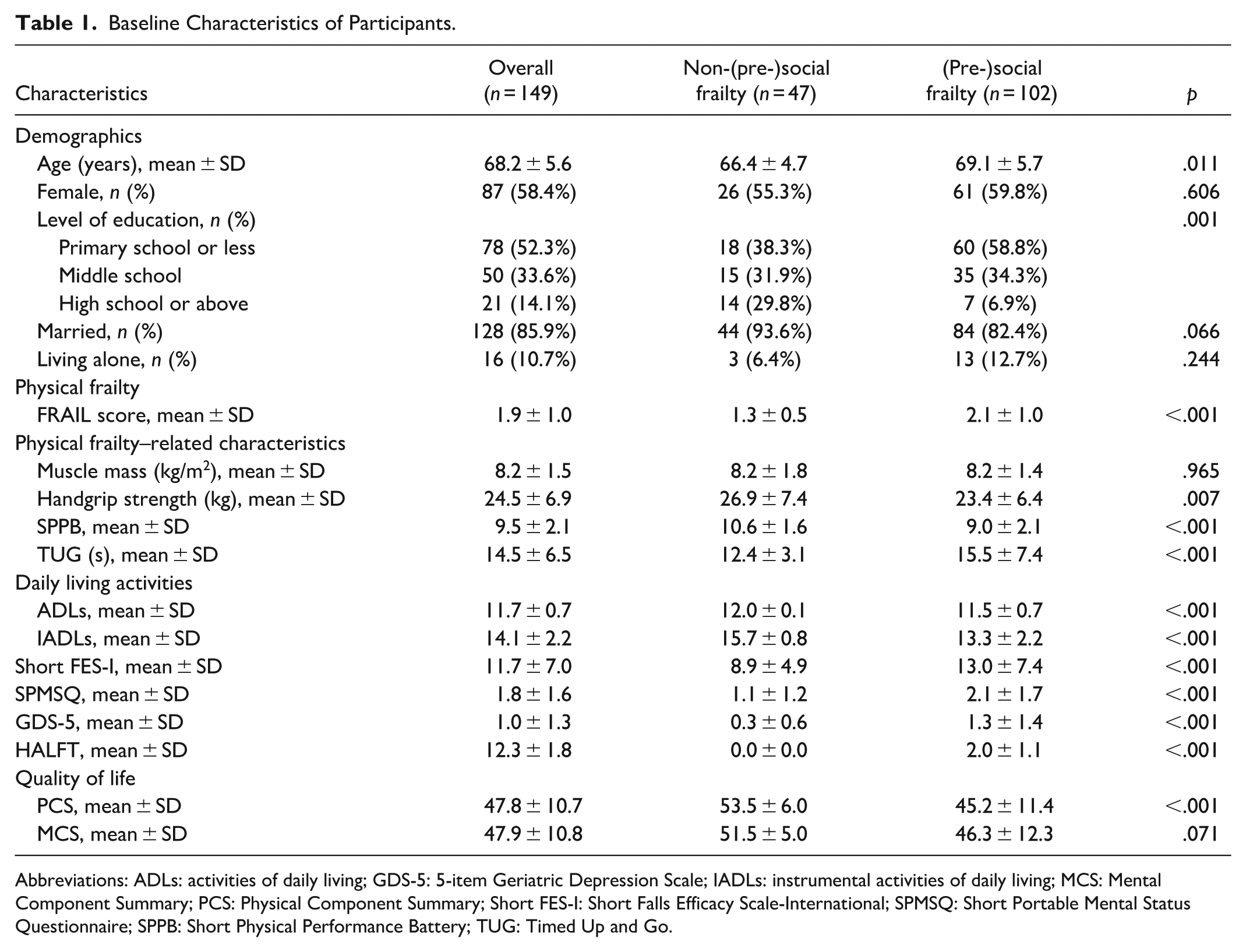
Abbreviations: ADLs: activities of daily living; GDS-5: 5-item Geriatric Depression Scale; IADLs: instrumental activities of daily living; MCS: Mental Component Summary; PCS: Physical Component Summary; Short FES-I: Short Falls Efficacy Scale-International; SPMSQ: Short Portable Mental Status Questionnaire; SPPB: Short Physical Performance Battery; TUG: Timed Up and Go.
Impact of Baseline (Pre-)Social Frailty on Intervention Effectiveness
Primary outcomes
Tables 2 and 3 present the outcomes following the intervention, both immediately and at subsequent follow-ups, in comparison with the control status. In the non-(pre-)social frailty group, significant beneficial intervention effects were observed on the FRAIL score (B = −0.407 to −0.328, p < .01; Table 2) and frailty status (odds ratio [OR] = 0.104-0.110, p < .05) at the 0-week and 12-week postintervention (Table 3). The (pre-)social frailty group showed beneficial treatment responses in the FRAIL score and frailty status at all time points (Table 2: B = −1.001 to −0.837, p < .01; Table 3: OR = 0.004-0.048, p < .05). No statistically significant differences were detected between the subgroups at any time point (all p for interaction > .05).
Impact of Baseline (Pre-)Social Frailty on Outcomes Using Intention-to-Treat Data Set.
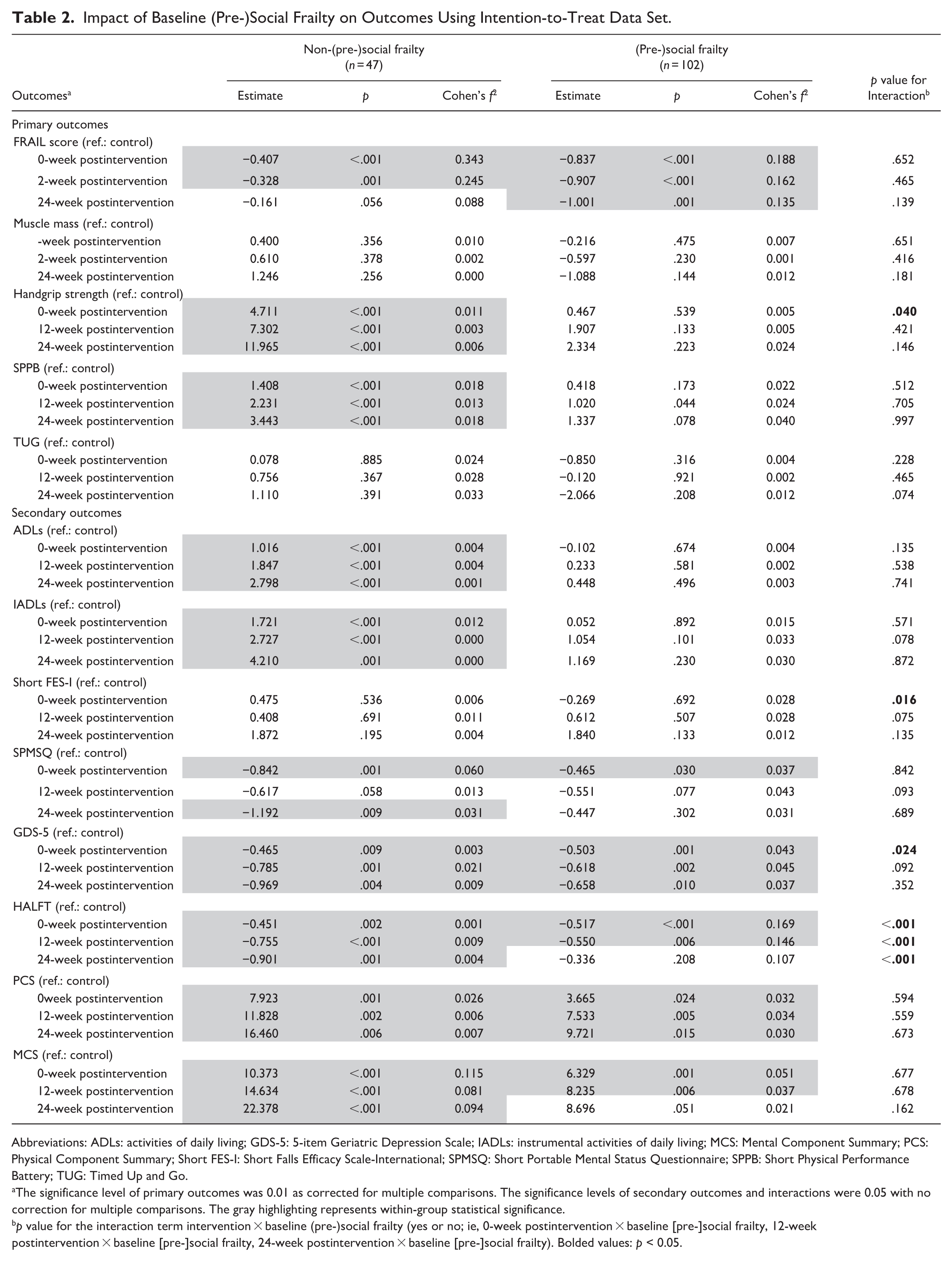
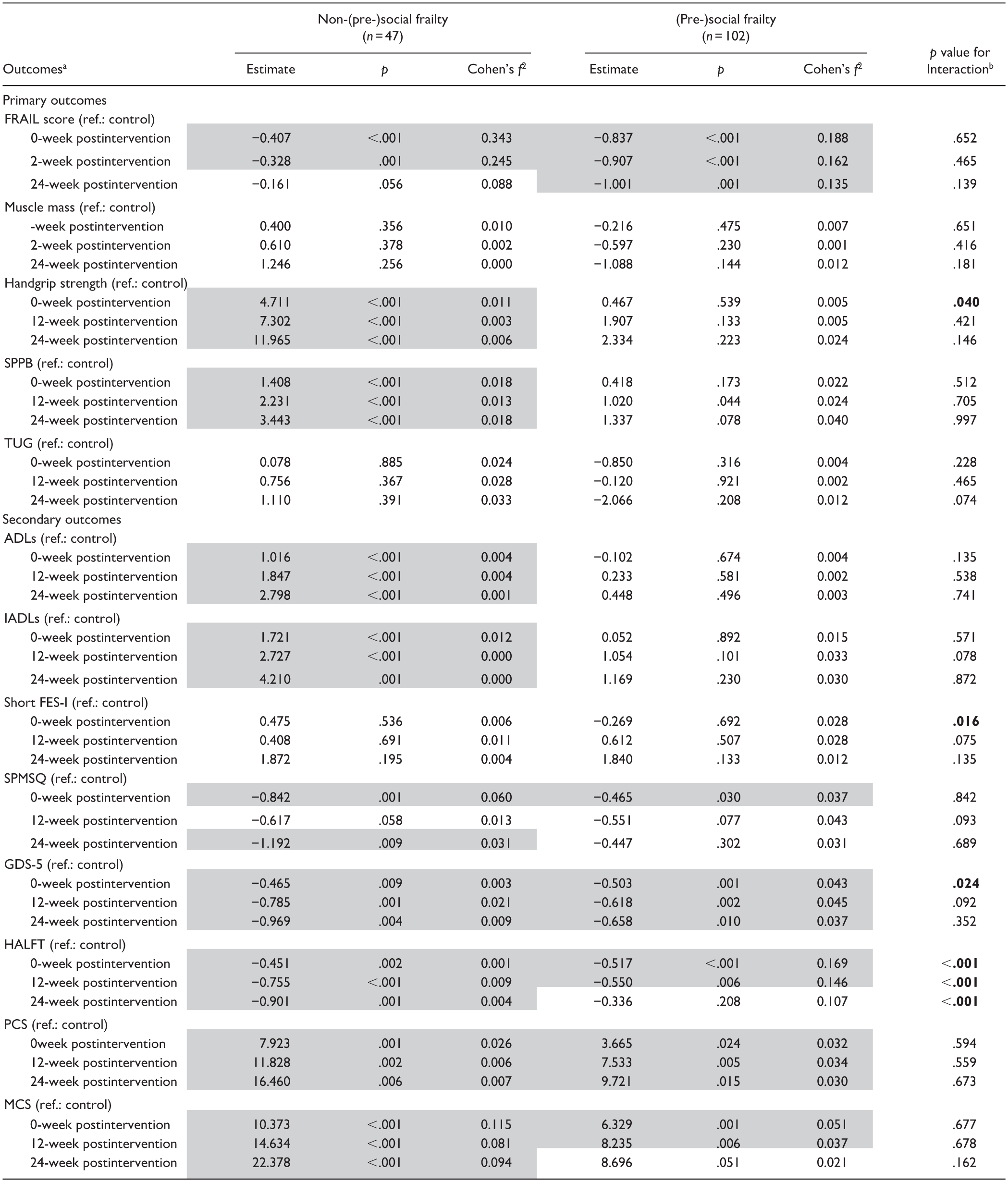
Abbreviations: ADLs: activities of daily living; GDS-5: 5-item Geriatric Depression Scale; IADLs: instrumental activities of daily living; MCS: Mental Component Summary; PCS: Physical Component Summary; Short FES-I: Short Falls Efficacy Scale-International; SPMSQ: Short Portable Mental Status Questionnaire; SPPB: Short Physical Performance Battery; TUG: Timed Up and Go.
The significance level of primary outcomes was 0.01 as corrected for multiple comparisons. The significance levels of secondary outcomes and interactions were 0.05 with no correction for multiple comparisons. The gray highlighting represents within-group statistical significance.
p value for the interaction term intervention × baseline (pre-)social frailty (yes or no; ie, 0-week postintervention × baseline [pre-]social frailty, 12-week postintervention × baseline [pre-]social frailty, 24-week postintervention × baseline [pre-]social frailty). Bolded values: p < 0.05.
Comparison between Physical Frailty Status and Social Frailty Status in Subgroups Using Intention-to-Treat Data Set.
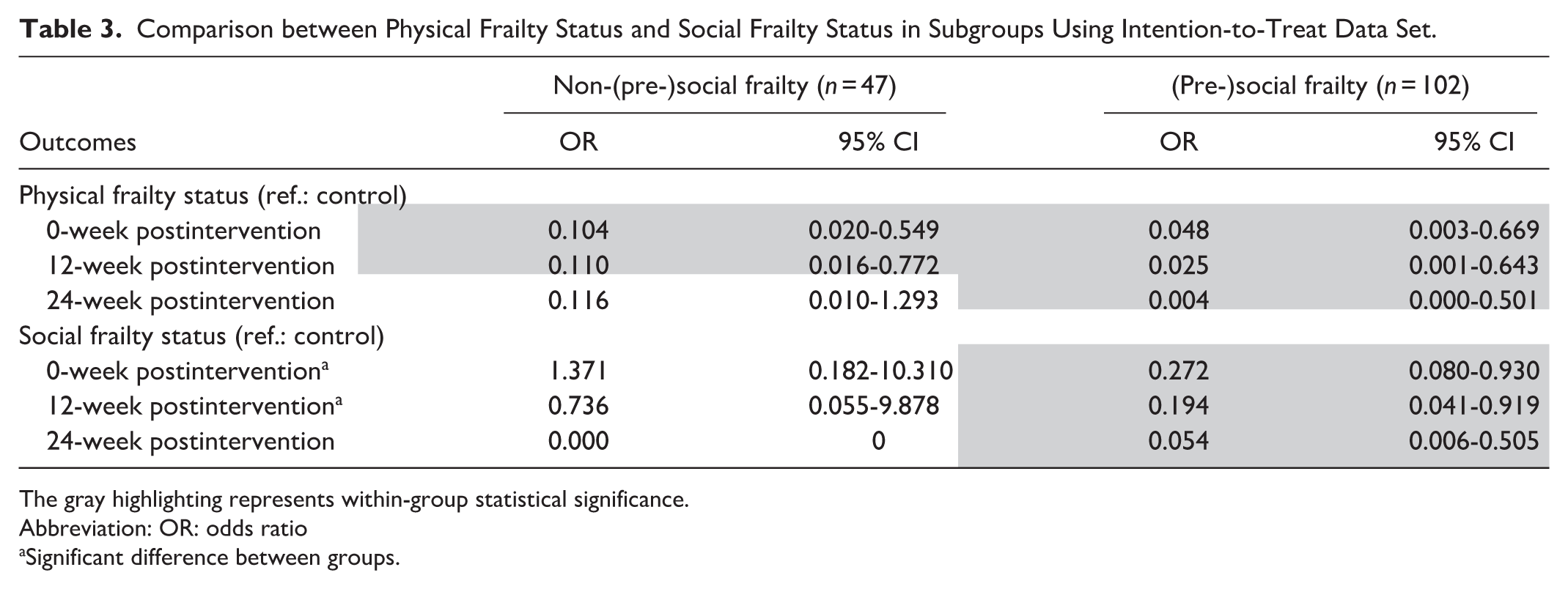
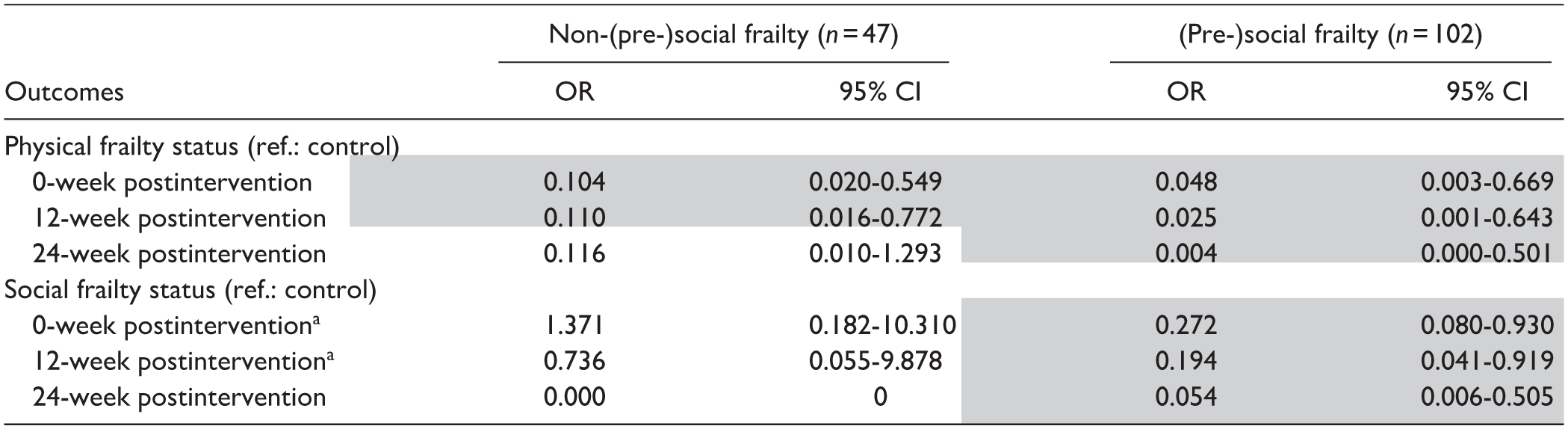
The gray highlighting represents within-group statistical significance.
Abbreviation: OR: odds ratio
Significant difference between groups.
In terms of frailty-related characteristics, no statistically significant differences were observed in muscle mass or the TUG at any time point, either within or between the subgroups. Notably, a significant beneficial intervention effect was found exclusively in the non-(pre-)social frailty group for handgrip strength (B = 4.711-11.965, p < .001) and the SPPB (B = 1.408-3.443, p < .001) at all time points. Additionally, a significant interaction effect for handgrip strength was noted at the 0-week postintervention (p for interaction = .040).
Secondary outcomes
Significant beneficial intervention effects were exclusively noted in the non-(pre-)social frailty group for ADLs (B = 1.016-2.798, p < .001) and IADLs (B = 1.721-4.210, p < .05) at all time points. Despite insignificant effects in either group, the (pre-)social frailty group showed a significantly larger effect size in the short FES-I at the 0-week postintervention (p for interaction = .016). There were significant beneficial intervention effects on the SPMSQ in the non-(pre-)social frailty group at the 0-week and 24-week postintervention (B = −1.192 to −0.842, p < .05), while such effects were only observed at the 0-week postintervention in the (pre-)social frailty group (B = −0.465, p = .037).
Both groups demonstrated beneficial intervention effects on the GDS-5 (B = −0.969 to −0.465, p < .05) and the PCS (B = 7.923-16.460, p < .05) at all time points, with significantly better effects on the GDS-5 in the (pre-)social frailty group at 0-week postintervention (p for interaction = .024).
Regarding the HALFT and the MCS, there were significant beneficial intervention effects in the non-(pre-)social frailty group at all time points, while they were only at the 0-week and 12-week postintervention in the (pre-)social frailty group. For the HALFT, the (pre-)social frailty group had significantly greater effect sizes at the 0-week and 12-week postintervention, but had smaller effect sizes at the 24-week postintervention than for the non-(pre-)social frailty group (all p for interaction < .001). As for social frailty status, beneficial intervention effects were found only in the (pre-)social frailty group at all time points (OR = 0.054-0.272, p < .05; Table 3), with significant interaction effects observed at the 0- (p for interaction < .001) and 12-week postintervention (p for interaction = .012).
Adherence and Adverse Events
There were no statistically significant differences regarding exercise adherence or dropout rates between subgroups (Table 4). Moreover, no adverse events occurred in either subgroup during the trial.
Exercise Adherence and Dropout Rate in Subgroups.
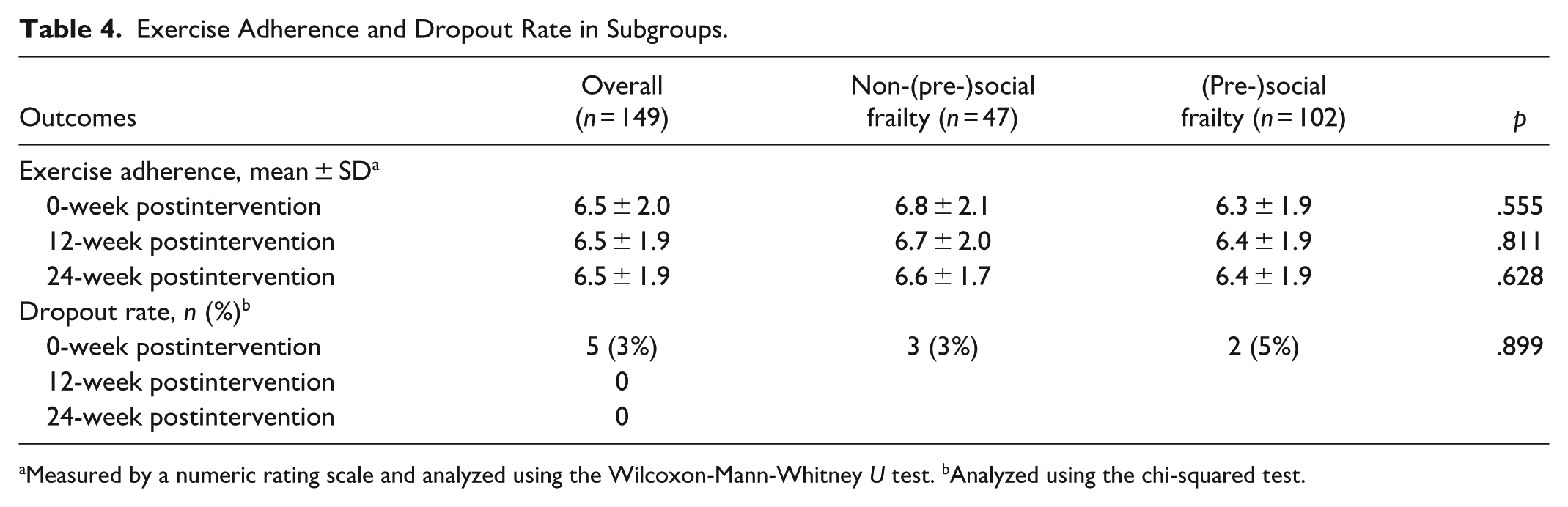
Measured by a numeric rating scale and analyzed using the Wilcoxon-Mann-Whitney U test. bAnalyzed using the chi-squared test.
Sensitivity Analyses
As for the non-(pre-)social frailty group, certain outcomes (ie, SPPB, ADLs, IADLs, GDS-5, HALFT, PCS) in the full analysis set did not show significant improvement, unlike those observed in the ITT analysis (Supplementary Tables S1 and S2), possibly due to the limited number of participants in the non-(pre-)social frailty group within in the full analysis set. Regarding the (pre-)social frailty group, the results obtained from the ITT analysis were generally consistent with those derived from the full analysis set, except for handgrip strength and SPPB, which showed significant intervention responses only in the full analysis set.
Discussion
This post hoc analysis of a SW-CRT revealed that (pre-)physically frail older adults without (pre-)social frailty experienced improvements across most outcomes following the exercise intervention. These improvements included reduced physical frailty, increased handgrip strength, enhanced lower extremity function, better performance in ADLs and IADLs, improved cognitive function, alleviated depressive symptoms, reduced social frailty scores, and improved QoL. Most of these benefits manifested immediately postintervention and showed sustained effects during follow-up periods. In contrast, (pre-)physically frail older adults with comorbid (pre-)social frailty exhibited a more selective response pattern, showing immediate improvements in physical frailty, cognitive function, depressive symptoms, and QoL. Notably, their gains in social frailty scores and mental QoL failed to persist over time. Another intriguing finding was that those with comorbid (pre-)social frailty demonstrated more pronounced immediate improvements in fear of falling, depressive symptoms, and social frailty status and score than their counterparts without (pre-)social frailty, yet they exhibited less persistent improvements in social frailty scores.
Generally, after the exercise intervention (pre-)physically frail older adults with (pre-)social frailty showed treatment responses to fewer outcomes than those without (pre-)social frailty. Notably, improvements in the comorbid group were predominantly observed in psychosocial domains, specifically cognitive function, depressive symptoms, social frailty (score and status), and QoL, whereas physical outcomes remained largely unaffected by the intervention. From the perspective of the nature of physical and psychosocial outcomes, it has been suggested that psychosocial markers are more likely to be changed by interventions than physical markers, 38 due to the high malleability of psychosocial markers and the stability and lagged response of physical indicators.39,40 Moreover, even without a targeted social support intervention element, this exercise intervention naturally fostered a supportive environment among participants, promoting communication and mutual assistance. Consequently, it may positively impact the psychological and social outcomes, even for (pre-)physically frail older adults with (pre-)social frailty.
In addition, compared with those of (pre-)physically frail older adults without (pre-)social frailty, the insignificant effects on physical indicators among those with (pre-)social frailty may be attributed to the detrimental impact of (pre-)social frailty on physical health, including handgrip strength, lower extremity function, ADLs, and IADLs.10,11,41 From a physiological perspective, social stressors associated with social frailty can trigger the release of pro-inflammatory cytokines in the body, 42 which can be linked to muscle wasting and decreased physical function. 43 This may prohibit those with comorbid (pre-)social frailty from achieving the same improvements in physical health following the intervention as those with only (pre-)physical frailty, leading to the unsatisfying treatment responses in muscle strength (handgrip strength), muscle endurance (lower extremity function), and physical functioning (ADL and IADL). Moreover, the concept of social frailty encompasses social isolation, limited social support, and reduced social participation, 9 all of which are closely related to adverse physical outcomes, thus making it particularly challenging for older adults who are (pre-)physically frail and (pre-)socially frail to improve their physical health. First, social isolation can lead to increased stress, 44 which can further impact the body’s physiological functions, such as muscle recovery ability. 45 Consequently, this can hinder improvements in muscle strength and function among (pre-)physically frail older adults with (pre-)social frailty. Additionally, due to insufficient social support, those with (pre-)social frailty may lack enough motivation and encouragement from their social environment to adhere to the exercise intervention, 46 possibly leading to the limited physical improvements in this study. Meanwhile, similar to the results of this study, low social participation was found to dampen the benefits of an exercise intervention on mobility among older adults. 47 This may be explained by the fact that low social participation can limit older people’s possibility to find meaningfulness in social environments, thus diminishing their confidence in remaining functionally independent. 47 This negative exercise belief could discourage exercise behavior, 26 ultimately limiting the effectiveness of the exercise intervention on physical outcomes such as muscle strength, physical performance, and physical independence as indicated by this study. Furthermore, social frailty can lead to cognitive decline, 48 making it more difficult for (pre-)physically frail older adults with (pre-)social frailty to understand and follow the exercise instructions, 49 hence the disappointing physical improvements.
Another important finding is that for some outcomes, the effects of the exercise intervention did not persist over time among (pre-)physically frail older adults with (pre-)social frailty. This could be due to the lack of long-term social support to reinforce the positive changes achieved through exercise. 50 Once the exercise intervention ceased, without continuous support from the social environment, (pre-)physically frail older adults with (pre-)social frailty may revert to their previous lifestyles, leading to the gradual loss of the intervention effects. 51 To address these issues, it is crucial to incorporate social support interventions into exercise programs. Social support interventions can provide (pre-)physically frail older adults with the necessary emotional, informational, and instrumental support. 52 Consequently, by integrating social support into exercise programs, more outcomes may be positively and persistently affected,53,54 ultimately improving the health-related outcomes of (pre-)physically frail older adults. In conclusion, the findings highlight the importance of considering social frailty when designing and implementing exercise interventions for (pre-)physically frail older adults. By understanding the mechanisms underlying the negative impact of social frailty on treatment responses, more targeted and comprehensive interventions could be developed to address both physical and social aspects of health. Future research should further explore the optimal combination of social support and exercise interventions to maximize the benefits for this vulnerable population.
Nonetheless, it is unexpected that (pre-)physically frail older adults with (pre-)social frailty showed more immediate improvements in fear of falling, depressive symptoms, and social frailty following the intervention than those without (pre-)social frailty. This finding is consistent with the vulnerability framework, 55 which posits that individuals with higher vulnerability face greater challenges in managing health-related limitations. As a result, they are more likely to rely on compensatory resources and respond more positively to targeted interventions aimed at enhancing these resources. Therefore, the increased vulnerability of participants with comorbid (pre-)social frailty,56,57 compared with that of those with solely (pre-)physical frailty, may explain their greater benefits from such interventions.
It is interesting to note that the intervention effects on social frailty status were observed only among (pre-)physically frail older adults who also had (pre-)social frailty. One potential explanation is the floor effect in the social frailty scores of non-(pre-)social frailty participants, who already had the lowest possible score (ie, 0) on the HALFT scale. 12 Conversely, those with (pre-)social frailty had more room for improvement in social frailty status. While the changes in their social frailty scores were not statistically significant, these changes could still result in shifts in social frailty status. Furthermore, this finding underscores the benefits of reporting outcomes using both continuous and categorical forms. The former enhances the probability of detecting potential enhancements, 38 whereas the latter provides an understanding of their practical implications. 58
Implications
Regarding exercise interventions targeting (pre-)physically frail older adults, it is important to assess whether the participants had (pre-)social frailty and implement stratified strategies based on their social frailty status to realize comprehensive and persistent intervention benefits. Moreover, for (pre-)physically frail older adults with comorbid (pre-)social frailty, it is essential to incorporate social support interventions, catering to the nature of social frailty, in addition to the current exercise interventions. Social frailty is a multidimensional concept consisting of insufficient social resources, social behaviors, social activities, and self-management capabilities. 9 To enhance social resources, mentorship and peer support could be utilized to strengthen social networks and obtain support from others. 59 Regarding social behavior, programs can be developed to enhance social participation, including improving close relationships and promoting involvement in community activities. 59 Additionally, group-based social interactions could be considered to encourage social activities. 60 Concerning self-management, self‑management education and psychological self‑management interventions could be employed to improve individuals’ ability of managing their emotions and behaviors. 59 These interventions could be adopted to ensure that more positive outcomes are achieved and sustained over time among this disadvantaged population with both (pre-)physical frailty and (pre-)social frailty.
Limitations
This study has several limitations. First, it is a post hoc subgroup analysis where the sample size was not predetermined, and may lead to a small number of participants identified to be (pre-)social frail. Nevertheless, the post hoc power analysis showed that the current sample size and improvements in FRAIL scores in each subgroup reached a satisfactory power (99.2%). 61 Second, the study did not measure other health-related factors, such as physical pain, that might be associated with outcomes and behavior changes. However, the ITT analysis based on the random allocation protocol employed in this study is capable of controlling for various confounding factors, including both known and unknown confounders, to ensure balance. 62 Additionally, the lack of correction for multiple comparisons in secondary outcomes further necessitates a cautious approach to interpreting the results. Lastly, because the participants were recruited from a single county in central China, the findings may lack the generalizability to other regions within China or other countries.
Conclusion
The exercise intervention yielded immediate and sustained improvements on more outcomes for (pre-)physically frail older adults without (pre-)social frailty than for those with (pre-)social frailty. These findings suggest that the presence of (pre-)social frailty may attenuate the long-term benefits of exercise interventions in this population. These results underscore the potential need to integrate targeted social support components into exercise programs to enhance both the breadth and durability of intervention effects for older adults with comorbid (pre-)physical and (pre-)social frailty.
Supplemental Material
sj-pdf-1-wjn-10.1177_01939459251384714 – Supplemental material for Impacts of (Pre-)Social Frailty on the Effectiveness of a Theory-Driven Exercise Intervention Among Community-Dwelling (Pre-)Physically Frail Older Adults
Supplemental material, sj-pdf-1-wjn-10.1177_01939459251384714 for Impacts of (Pre-)Social Frailty on the Effectiveness of a Theory-Driven Exercise Intervention Among Community-Dwelling (Pre-)Physically Frail Older Adults by Wendie Zhou, Xiaoxia Qiao, Peng Zhao, Yiran Zhang, Xuan Tang, Yanyan Li, Jiaqi Yu, Xue Wang, Hejing Chen and Cuili Wang in Western Journal of Nursing Research
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (72274009), the National Natural Science Foundation of China (72404180), and the Fundamental Research Program of Shanxi Province (202303021222157). The sponsors had no role in the design, methods, subject recruitment, data collection, analyses, and preparation of this paper.
Ethical Considerations
The parent study was approved by the Institutional Review Board of Peking University (no.: IRB00001052-20094) on December 25, 2020.
Consent to Participate
All participants provided their written informed consent before their involvement in the study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.