
Abstract
Background:
Although progress has been made in teaching dementia care to nursing students, there is still a need to include person-centered dementia care (PCDC) education, because nursing students have a limited understanding of this approach.
Objectives:
This study aimed to explore the perceptions of prelicensure nursing students regarding PCDC within the context of their professional nursing education.
Methods:
This study used a qualitative descriptive design using Brooker’s VIPS model as a conceptual framework. Data were collected through individual and semi-structured interviews conducted virtually from January 22, 2024, to March 8, 2024, and analyzed using thematic analysis.
Results:
Thirty prelicensure nursing students completed the interviews. Five primary themes were identified: knowledge of PCDC interventions, PCDC perceived negatively as an intervention, education, long-term care facilities (LTCFs), and joining the dementia care workforce.
Conclusion:
Prelicensure nursing students demonstrated a higher level of knowledge of PCDC than anticipated. However, 2 key educational gaps were noted: first, nursing students require more instruction on the safe and ethical use of restraints; and second, they need greater awareness that older adults, including those with dementia, receive care across nearly all healthcare settings, not only in LTCFs. The findings of this study inform curriculum modifications and provide guidance to educators on teaching strategies that are derived from the experience of nursing students, who emphasized their desire for more role modeling or simulation on communicating with people with dementia.
Introduction
The prevalence of Alzheimer’s disease and related dementias (ADRD) in the United States poses a substantial public health concern, impacting millions and profoundly influencing the overall well-being of the population. Globally, dementia affects over 55 million individuals, with nearly 10 million new cases reported annually, ranking as the seventh leading cause of death both internationally and in the United States.1,2
The shortage of certified geriatric nurses, with less than 1% holding certifications in 2020, emphasizes the pressing need for increased specialization to address the growing needs of the aging population, particularly those with ADRD. 3 Simultaneously, the National Center for Health Workforce Analysis warns of a decade-long shortage of geriatricians, projected to worsen by 2025, intensifying the demand for professionals, such as registered nurses, to address and meet the challenges associated with the rising prevalence of ADRD. 4
Care for persons with ADRD often involves the extensive use of pharmaceuticals, particularly to address the commonly associated behavioral and psychiatric symptoms of dementia, such as aggression and agitation. 5 These symptoms typically manifest when older adults living with dementia attempt to express unmet physical and emotional needs that are common in older age, but that people with dementia (PwD) cannot communicate in the usual ways, such as stating they have pain. 6 It is important to note that nonpharmacological interventions, primarily rooted in person-centered care (PCC), are the preferred approach for managing ADRD, 7 and are proven to reduce behavioral and psychiatric symptoms of dementia, wandering, and depression in older adults with dementia. 5 PCC has become a model in long-term care facilities (LTCFs), with a 2017 Centers for Medicare and Medicaid Services regulation mandating PCC adoption for all residents. 4 This regulation emphasizes the need for foundational training in PCC for care providers, including nursing students.
Despite calls for enhanced care for PwD and the existence of significant statistics and movements advocating for it, the educational content on person-centered dementia care (PCDC) is notably absent in the curricula of many healthcare programs, including nursing. 8 PCDC applies PCC principles specifically to dementia, often operationalized via Brooker’s VIPS framework: Valuing PwD and their careers (V), treating them as Individuals (I), seeing care from the Perspective of the person (P), and fostering a supportive Social environment (S). 9 Additionally, both registered nurses and nursing students often demonstrate poor knowledge and negative attitudes toward dementia care and PwD. The complexities associated with caring for PwD are commonly viewed as overwhelming challenges. Given the low to moderate dementia care knowledge among nursing students and their reluctance to enter the geriatric workforce, urgent attention is needed to enhance their knowledge, skills, empathy, and attitude, as the content taught in educational institutions can significantly impact the quality of care for PwD.5,10,11
Therefore, the purpose of this study was to explore the prelicensure nursing students’ perceptions of PCDC with the ultimate goal of enhancing and transforming the PwD’s healthcare experience. This study sought to provide insights into potential curriculum modifications and recommendations for effective teaching strategies for PCDC. Dawn Brooker’s VIPS model was adopted as the theoretical foundation for this study. The model emphasizes the importance of understanding and responding to the individual needs of PwD through a holistic approach that focuses on maintaining dignity, respect, and meaningful social connections. 9
Methods
Study Design
A cross-sectional, qualitative, descriptive design was used for this study. The use of a descriptive design is often recommended to provide straightforward descriptions of experiences and perceptions, particularly in areas where little is known about the topic under investigation. 12 This study follows the Standards for Reporting Qualitative Research to ensure transparency and rigor in reporting qualitative findings. 13
Participants
Using purposive sampling, participants were recruited from a state university in a large midwestern city. Eligibility criteria for participation included: (1) students in their third or fourth year of baccalaureate professional nursing education (prelicensure), (2) majoring in nursing, (3) enrolled either full-time or part-time, and (4) fluent in spoken and written English. Participants were excluded from the study if they: (1) were not fluent in English, (2) were not majoring in nursing, or (3) were students in the RN to BSN track (ie, they were already licensed nurses).
Data Collection
Data were collected through in-depth individual and semi-structured interviews conducted between January 22, 2024, and March 8, 2024. The screening process occurred when student participants expressed interest in participating via email or text messages. Subsequently, scheduling of the interviews and sharing of the Zoom interview links were facilitated through email correspondence. The interviews were conducted by the first author virtually via the Zoom platform and were audio-recorded and transcribed verbatim. Zoom autotranscripts were generated and then line-checked against the audio by the first author; discrepancies were corrected immediately after each interview. To enhance accuracy, a second coder spot-checked ~20% of transcripts against the audio; disagreements were resolved by discussion. The average interview length was between 25 and 45 min. Sample size was guided by information power and operationalized via code-saturation monitoring; recruitment ceased when no new codes emerged across 3 consecutive interviews. Monetary incentives were provided. Example interview questions are presented in Table 1.
Examples of Interview Questions.
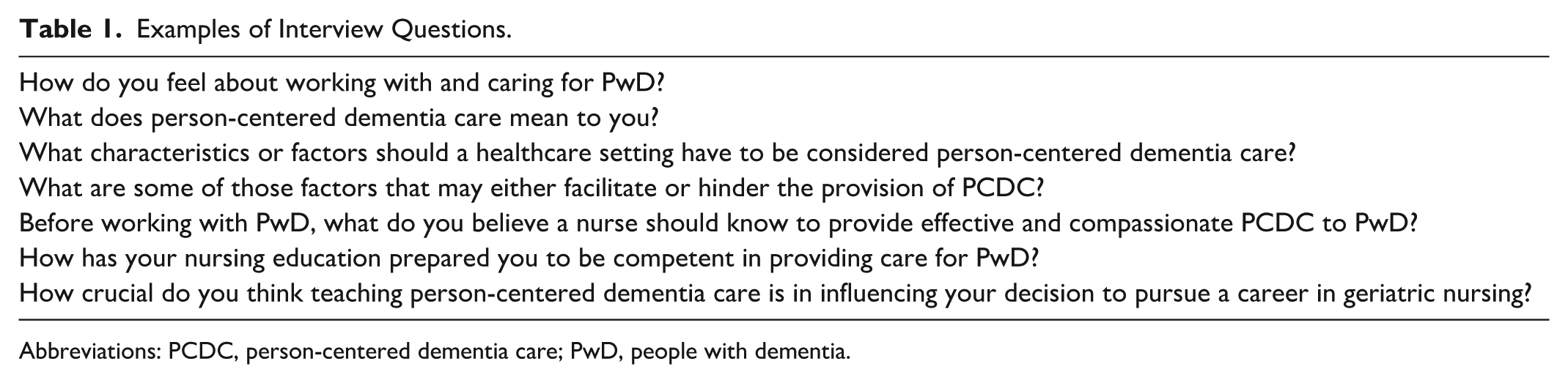
Abbreviations: PCDC, person-centered dementia care; PwD, people with dementia.
Data Analysis
Thematic analysis was used to analyze the interview data, and it occurred simultaneously with data collection. The interviews were transcribed at the time of the interview using Zoom’s transcription feature. Thus, the data cleaning process took place immediately after each interview. The cleaning process involved de-identifying all personal information, removing redundant words, and correcting mistranscribed words by re-listening to the interview’s audio recordings. Once the data were cleaned, the coding process began. Braun and Clarke’s non-linear 6-phase guide for thematic analysis was followed in this study, including familiarization with data, line-by-line open coding, grouping codes to create themes, and reviewing and defining those themes. 14 Two researchers independently coded an initial subset to calibrate the codebook; the first author then coded all transcripts, with analytic memos and peer debriefs to refine themes and definitions.
Credibility was enhanced through investigator triangulation (2 researchers), audit trails (codebook and analytic memos), and peer debriefing. Transferability was addressed via a thick description of context and participants. Dependability and confirmability were supported by documentation of analytic decisions and reflexive journaling.
Ethical Approval
This study was approved by the school’s Institutional Review Board (IRB# 24.130). Verbal informed consent was obtained from all participants, who were informed of their right to withdraw from the study at any time without consequences. The research purpose and methods were thoroughly explained to them. Participant identities were anonymized using numbers to ensure confidentiality.
Results
Participants’ Characteristics
A total of 30 students were enrolled in the study and completed interviews. All participants were majoring in the professional nursing program, with a mean age of 23.1 years. Of the participants, 23 (76.7%) were fourth-year nursing students, and 7 (23.3%) were third-year nursing students. In addition, 5 participants (16.6%) had volunteered in LTCFs, 13 participants (43.3%) had experience with a family member diagnosed with dementia, and 14 participants (46.6%) had prior work experience in LTCFs. Furthermore, 7 participants (23.4%) out of the 30 had experienced 2 or more of the following: volunteering at an LTCF, working in an LTCF, or having a family member with dementia (Table 2).
Participants’ Characteristics (N = 30).
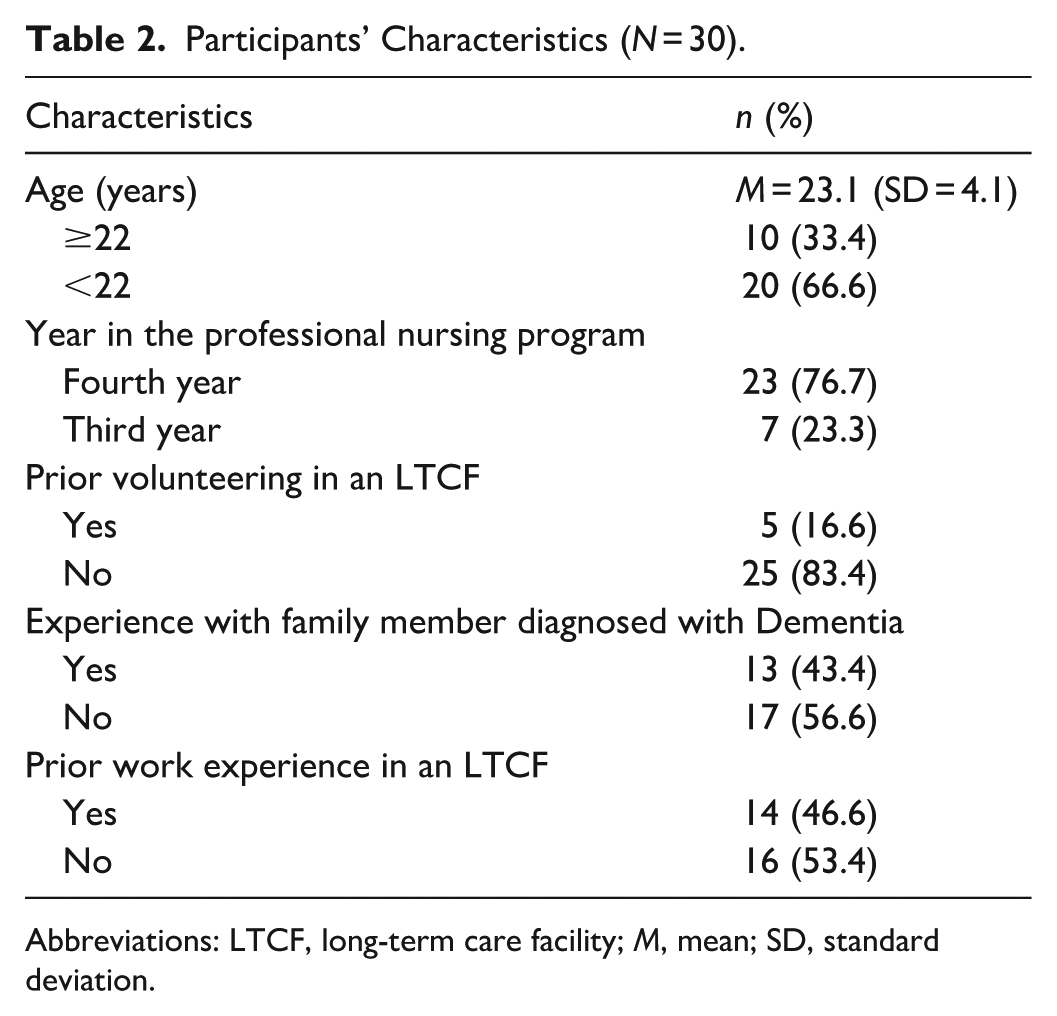
Abbreviations: LTCF, long-term care facility; M, mean; SD, standard deviation.
Themes
Five themes emerged from the data analysis: (1) foundations of PCDC; (2) challenges and negative perceptions of PCDC; (3) educational preparation and gaps; (4) perceptions of LTCFs; and (5) dementia care and career intentions (Table 3).
Themes, Subthemes, and Representative Quotes.
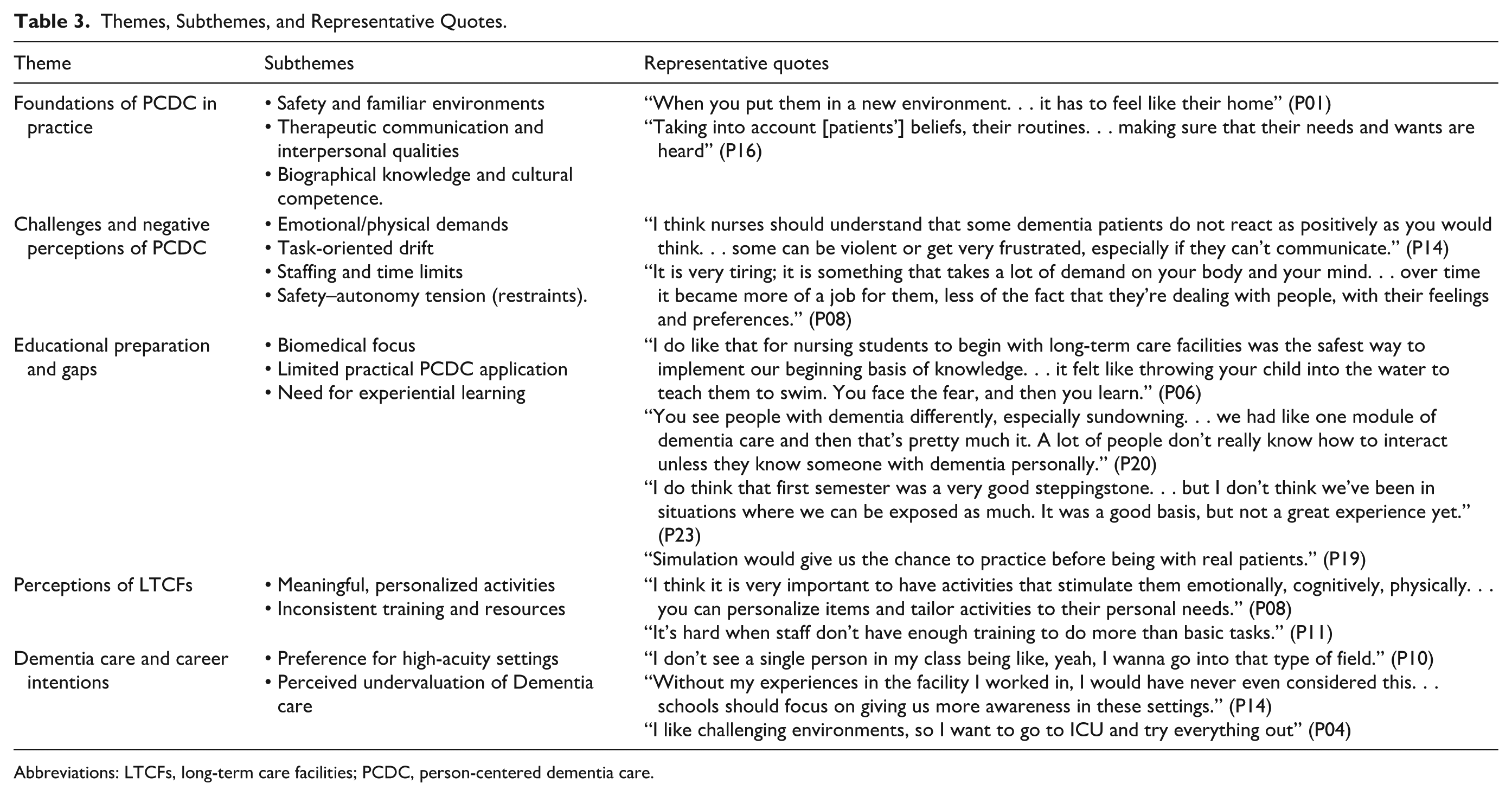
Abbreviations: LTCFs, long-term care facilities; PCDC, person-centered dementia care.
Theme 1: Foundations of PCDC in Practice
Students described safety, familiarity, and empathy as essential to PCDC. They emphasized that PwD often experience confusion, forgetfulness, and difficulty interpreting their surroundings, making safety precautions to prevent falls and wandering a priority. As 1 student explained, PCDC “revolves around safety. . . making sure that these people are able to walk around where they live” (P25). Beyond physical safety, participants highlighted the interpersonal qualities of nurses, stressing that effective PCDC requires empathy, respect, and therapeutic communication. As 1 participant summarized, “to have person-centered care, the nurse should have empathy, respect. . . and also have good communication” (P21).
Theme 2: Challenges and Negative Perceptions of PCDC
While students valued PCDC, many described its delivery as physically and emotionally demanding. Repeated explanations and communication breakdowns with PwD were frequent triggers for frustration, compounded by staffing shortages and time constraints that limited individualized care. One student reflected that providing PCDC was “very tiring” and, over time, began to feel “more of a job. . . less of the fact that [nurses are] dealing with human beings” (P08). These challenges highlighted the tension between students’ ideals and the realities of dementia care.
Theme 3: Educational Preparation and Gaps
Students’ reflections on education echoed this tension. Participants acknowledged that their curriculum provided a solid biomedical foundation and training in safety principles, but reported limited preparation for individualized, PCC. PCDC often remained abstract, leaving students unsure how to implement it in practice. As 1 reflected, “we learned a lot about safety. . . but maybe a little bit more on person-centered care would help before clinicals” (P05). Others advocated for experiential learning strategies such as role-play and simulation, explaining that such methods would “make it more real” (P19). Clinical experiences in LTCFs were seen as a useful “first step,” but learning was sometimes restricted by limited teaching time and staff workload.
Theme 4: Perceptions of Long-Term Care Facilities
Experiences in LTCFs further shaped how students made sense of PCDC. Students with exposure to LTCFs described them as contexts that could either support or constrain PCDC. They valued meaningful, individualized activities that promoted engagement, with one explaining that “activities that stimulate them—like singing or music—are really impactful, especially when personalized” (P08). At the same time, they observed that inconsistent staff training and systemic limitations often diluted the promise of person-centered approaches.
Theme 5: Dementia Care and Career Intentions
Finally, students linked their perceptions of PCDC to their developing professional identities. While they acknowledged its importance, many expressed reluctance to pursue dementia care as a career, positioning acute and high-intensity specialties as more appealing. One participant explained, “I’ll probably be in ICU or ER. . . I don’t think I could see myself working in dementia care” (P10), while another added, “I like challenging environments, so I want to go to ICU and try everything out” (P04). Dementia care was often framed as slower, less stimulating, and undervalued.
Discussion
As the aging population continues to grow, the prevalence of ADRD is increasing, necessitating a well-prepared nursing workforce to ensure the highest quality care for PwD. The literature review revealed that studies on PCC use in dementia care, or PCDC, have increased in recent years due to its widespread acceptance and promising impact on PwD well-being.9,15 These studies have focused on measuring outcomes for PwD, such as behavioral and psychological symptoms of dementia, use of neuroleptic medications, and changes in quality of life.16,17
Moreover, the literature review also revealed a body of knowledge on the integration of PCC into baccalaureate nursing curricula (prelicensure nursing education). However, these research studies primarily focus on identifying factors that predict PCC competence among nursing students,18,19 with some exploring the learning experience within 1-semester elective courses. 20 Notably, research studies specifically addressing PCDC within prelicensure nursing education and assessing the extent of PCDC content received are lacking. Therefore, this study aimed to explore the perceptions of prelicensure nursing students regarding PCDC within their educational context.
The study identified 5 primary themes reflecting nursing students’ experiences and thoughts; these themes are: (1) Foundations of PCDC in practice; (2) challenges and negative perceptions; (3) educational preparation and gaps; (4) perceptions of LTCFs; and (5) career intentions and identity. Overall, the prelicensure nursing students demonstrated a higher level of knowledge regarding PCDC than anticipated. Some students had prior experience working in nursing homes or assisted living facilities with PwD, and a few had personal experience with grandparents affected by dementia. This exposure likely contributed to their depth of knowledge. However, the overall level of understanding exceeded expectations, considering that the college curriculum integrates geriatric content throughout rather than offering a dedicated geriatrics course.
In this study, prelicensure nursing students expressed the belief that PCDC should be centered around the person’s preferences and values. They emphasized the importance of planning and delivering care in a holistic and comprehensive way, considering the person’s voice and involving their support system (eg, family members or friends), and preserving their autonomy as much as possible. This finding aligns with previous research 21 where nursing students highlighted that PCC is a comprehensive approach and should be an integral part of the nursing process.
While prelicensure nursing students recognized the importance of maintaining safety for PwD, this study found that they required more education regarding restraint use. Participants described strategies such as locked units, ankle monitors for wandering, and even physical restraints for agitated patients—interventions that restrict movement and raise ethical concerns about autonomy. In contrast, Tanaka 22 reported that nursing students in Japan expressed strong opposition to the use of physical restraints, particularly when they observed nurses employing restraints without first attempting alternative interventions. These students framed restraint reduction as a matter of person-centeredness, autonomy, and advocacy. This divergence may reflect differences in curricular emphasis, cultural framing of safety versus autonomy, or the clinical settings to which students were exposed. Another explanation is that our data reflect self-reported understanding rather than observed clinical practice. Students may verbalize acceptance of restraints as a safety measure, yet in practice might respond differently when faced with real clinical contexts and institutional norms. Recognizing this limitation emphasizes the need for future studies to examine not only students’ knowledge and attitudes, but also their actual clinical behaviors and decision-making when confronted with ethical dilemmas in dementia care.
Moreover, despite long-standing regulations such as the Omnibus Budget Reconciliation Act of 1987 and a robust evidence base showing that physical restraints are harmful, participants frequently lacked clarity about what is considered a restraint. 23 Restraints are often justified for patient safety when behaviors such as wandering or resisting care are perceived as “unsafe” by nurses and other healthcare providers. Therefore, the best practice to maintain patient safety is to develop an individualized care plan that includes understanding the patient’s usual or baseline behaviors. In addition, investigating the underlying triggers of behaviors is critical to individualizing care and preventing the use of any form of restraint. Examples of these triggers could include unmet physical needs or communication challenges. It is worth noting that using restraints does not prevent falls or fall-related injuries in high-risk patients. Instead, implementing strategies such as assisting the patient in getting out of bed is recommended. 24 In PCC, there is an inherent tension between providing for safety and autonomy; therefore, education that focuses too narrowly on safety without considering autonomy is not truly person-centered. According to Kitwood’s philosophy, when delivering PCDC, the focus should be on how tasks are done rather than solely on what is done. 25 This principle was evident in the data, where prelicensure nursing students expressed a belief that nurses often carry out care tasks hastily, neglecting the fact that PwD are human beings with feelings. Prelicensure nursing students note that nurses sometimes prioritize physical needs over emotional well-being, which they emphasized as equally important for all patients and particularly crucial for those with dementia. prelicensure nursing students attributed these behaviors among nurses to their busy schedules, high nurse-to-patient ratios, burnout, turnover, and lack of education or training regarding PCDC. This finding is consistent with previous research, 26 which identified nurse busyness, lack of awareness of PCC, and excessive workload as barriers to implementing PCC in general healthcare settings.
Regarding nursing school education on PCDC, prelicensure nursing students in this study perceived that they had received good foundational education on dementia care and the disease process, which has significantly increased their knowledge in this area. This finding contrasts with Laura et al, 27 where nursing students reported receiving limited education on dementia, particularly a lack of clinical exposure to working with PwD. In addition, prelicensure nursing students in this study appreciated the education they received, including a 1-semester clinical exposure in an LTCF. However, they expressed a desire for more specific practical knowledge on interventions and problem-solving strategies for behavioral issues in PwD. A recurrent theme was the suggestion to incorporate simulation-based activities and clinical interactions with PwD at different times of the day. Previous research supports the use of simulation to enhance nursing students’ learning experiences and knowledge, and to increase their confidence when working with PwD, especially when addressing the challenging behaviors and critical situations that might arise with this population. 28 A study by Haugland and Reime, 29 showed that the use of simulation increased prelicensure nursing students’ knowledge of the importance of learning PCDC, which includes knowing patients’ history, building personal relationships, and gaining the trust of the patient. It also demonstrated through ethical scenarios that stimulation improved their comprehension of the legislations of coercion use and increased their confidence in handling challenging situations by enhancing their communication skills. 29
In this study, prelicensure nursing students discussed a couple of activities that can be implemented in LTCFs to keep PwD socially engaged and prevent them from being left alone. They also mentioned that these activities should be personalized to the individuals’ needs and preferences. Among the activities mentioned, singing classes were highlighted. Music therapy has been shown to be one of the most impactful management interventions for PwD, specifically beneficial in addressing behavioral and psychiatric symptoms of dementia.30,31
Finally, prelicensure nursing students in our study expressed less desire to work with PwD, despite feeling confident in their knowledge and skills and recognizing the increasing aging population and the need for more geriatric nurses. Some factors mentioned by prelicensure nursing students in this study align with those in previous research.10,32 These factors included personal preference, lack of faculty enthusiasm, lack of confidence, and nursing schools’ emphasis on other specialty areas such as Critical Care, Obstetrics, and Pediatrics. Furthermore, while most nursing students do not plan to work in LTCFs or consider geriatric nursing as a career option, they will inevitably care for older adults across diverse clinical settings. In US hospitals, approximately 1 in 4 patients has dementia, emphasizing the need for all nurses—not only those in long-term care—to be prepared to deliver PCDC. 33 Thus, PCC is the essence of holistic nursing care for all patient populations and not just limited to PwD. Nursing students must be prepared and trained to implement this care approach regardless of the setting in which they will be practicing.
Limitations
This study has limitations. First, the findings are based on nursing students’ self-reported perceptions of PCDC, which may not fully reflect their actual clinical behavior. Students may articulate ideals that differ from what they would enact in practice, particularly when influenced by institutional norms, systemic pressures, or the complexities of real patient care. Future research using observational methods or triangulating self-reported data with clinical performance evaluations could provide a more accurate understanding of how knowledge and attitudes translate into practice.
Second, the sample was drawn from a single educational institution in 1 state, which restricts the transferability of findings to broader or international contexts. Future cross-cultural or multi-institutional studies could compare how PCDC is conceptualized, taught, and practiced across different nursing programs and healthcare systems. For example, such studies might reveal whether students in collectivist cultures emphasize family involvement more strongly, or whether programs with earlier clinical exposure foster greater competence in individualized care. These comparative insights would highlight context-specific challenges while helping identify culturally sensitive teaching strategies and curricular adaptations that support broader implementation of PCDC.
Finally, although students reported increased understanding of PCDC, their reflections emphasized the need for more experiential learning opportunities. Nursing curricula should integrate simulation, role-play, and theory-based scenarios that mirror real-life challenges, as well as structured training modules delivered just before clinical placements. Such approaches could optimize students’ ability to apply PCDC principles in practice.
Conclusion
The current study aimed to explore the perceptions of prelicensure nursing students regarding PCDC within the context of their professional nursing education. Several themes emerged from the thematic analysis that are valuable for informing future research and policy changes related to teaching PCDC and working with PwD. The study’s results can serve as a foundational baseline for understanding PCDC among prelicensure nursing students.
Footnotes
Author Note
This manuscript is part of the primary author’s PhD dissertation. The coauthors served as the dissertation committee members.
Ethical Considerations
This study was reviewed and approved by the University of Wisconsin-Milwaukee Institutional Review Board (IRB# 24.130).
Consent to Participate
Verbal informed consent was used at the time of the interview to reduce perceived pressure on the students, maintain anonymity, and reflect the minimal risk nature of the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institutes of Health under award number 5R01AG074227-03 “Relationships of dementia care workforce experiences, training, and work environment to resident outcomes in skilled nursing facilities” (PI: L.M. Wagner). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data are available upon request from the primary author.