
Abstract
Background:
Models of rounding are different across institutions and nurses do not always participate or feel involved during daily rounds.
Objective:
The purpose of this analysis was to examine nurses’ contributions during family-centered rounds in a children’s hospital.
Methods:
This study is a secondary analysis of 50 video-recorded conversations between families of pediatric patients and clinicians during daily rounds in a Midwest children’s hospital. Children were patients of one of the 4 participating medical teams: 2 general pediatric hospitalist services, the pulmonary service, or the hematology/oncology service. Data were analyzed using conversation analysis and content analysis. We identified and categorized the “action” of nurse utterances or what they were “doing” in the conversation.
Results:
Nurses contributed to daily rounds to accomplish a variety of actions. Although it was most common for nurses to provide information and assessments, nurses were also active in making recommendations and correcting information that was shared. Nurses also asked clarifying questions, either for themselves or on behalf of the family. However, when solicited to ask a general question or add information at the end of the conversation, nurses most often passed on the opportunity to participate, or at times, first denied having questions before asking a question or adding information.
Conclusion:
Nurse contributions to daily rounds demonstrate that a normative role for nurses is to provide information or assessments, with limited question-asking. We also found that nurses displayed their role as an advocate by asking questions to the team on behalf of the family.
Keywords
Introduction
Daily rounds occur in hospitals globally, yet there is great heterogeneity in how rounds are structured, how often rounds occur, and the purpose of rounding. 1 In some rounding models, only the medical team is included for the purposes of patient care and trainee education, in which nurse communication and attempts to contact physicians are seen as interruptions. 2 Other rounding models only include various nursing roles (bedside nurse/staff nurse, case manager, nursing director, clinical nurse specialist, etc.) for the purpose of rapid communication to decrease the patient’s length of stay. 3 A scoping review of interprofessional bedside rounding models that incorporate both the medical team and nurses, along with patients and families, found positive outcomes for the team, patient, and care quality. 1 In addition, healthcare members have described interprofessional rounds as a way to facilitate information sharing and provide more effective patient-centered care. 4
Nurse Participation in Daily Rounds
Despite the benefits of interprofessional rounds, there are barriers to nurses participating during daily rounds. Nurses are not always asked to attend rounds 5 or are not notified when the medical team is rounding on their patients.6,7 Even when invited and notified, nurses’ heavy and unpredictable workloads often mean having to address the needs of patients instead of attending rounds.6,8 When nurses are present, not all physicians ask for their input7,8 and many nurses do not feel involved. 5 Rounding structures may not always be present for nurses to actively participate and the nurses themselves may be unfamiliar with their role during daily rounds. 9
Implementation of structured models that encourage nurse involvement in daily rounds increases nurse presence and participation.7,10 Some models specify a role for the nurse, such as the structured interdisciplinary bedside rounds standard communication protocol that assigns the nurse to update the patient’s status by reviewing overnight events, patient goals for the day, and any concerns, along with reviewing items in a quality-safety checklist. 11 However, in the absence of preassigned tasks and roles, it is not yet known how the nurse contributes to daily rounds.
Purpose
Studying daily rounds via video recording can provide insight into how nurses contribute to conversations during daily rounds. Additionally, studying communication can inform how participants are normatively oriented to the structure of a given conversation. 12 Thereby, studying nurses’ contributions to the conversation can be a first step to show how nurses are oriented to their role during daily rounds. The purpose of this analysis was to examine nurses’ contributions during family-centered rounds (one model of interdisciplinary rounds) in a children’s hospital.
Methods
This study is a secondary analysis of data collected from February 2013 to May 2013 as part of a randomized controlled trial (RCT) that examined the use of a family-centered rounds checklist. The outcomes of interest for the RCT were family engagement and patient safety 13 and did not include nurse contributions to rounds. We used conversation analysis and content analysis to examine nurses’ contributions during video-recorded daily rounds conversations.
Sample and Setting
There were a total of 673 video recordings of conversations during daily rounds in a Midwest children’s hospital in the RCT study. 13 Participants were eligible for the RCT if they met the following criteria: able to speak and read English, children were under the age of 18, children did not have a new cancer diagnosis or sensitive or stigmatizing reason for hospitalization, and children were patients of one of the 4 medical teams participating in the study: 2 general pediatric hospitalist services, a pulmonary service, or a hematology/oncology service.
We a priori selected to view video recordings of the final 75 daily rounds conversations because it was enough data to identify patterns while still being manageable for analysis. We decided to use the last recordings of the dataset because the longer participants are observed, the more likely they are to return to their usual behaviors. 14 The 75th video recording involved a family that had recordings on 2 subsequent days, resulting in 77 video recordings. Of the 77 conversations, nurses were not present in 20, and nurses were present but did not contribute to the conversation in 7, leaving a sample size of 50 conversations for analysis of nurse contributions during daily rounds.
Data Collection
A member of the RCT research team video recorded daily rounds in the patients’ rooms or in the hallway by the patients’ rooms, depending on where the conversation occurred. Data were transcribed using notations for conversation analysis; however, the notations have been removed to enhance readability. To view the excerpts with all appropriate notations, please see Appendix A in the Supplemental Material. 15 Protected health information was not included in the transcripts. We indicated members of the medical team (including resident physicians and medical students) with “Dr”; nurses with “RN”; and family members with “Fa”; as well as a number assigned during transcription (the first physician to talk is “Dr1,” the second is “Dr2,” etc.).
Data Analysis
Identifying Actions of Nurse Contributions
We used conversation analysis to identify the actions of nurses’ contributions in the conversation during daily rounds. Conversation analysis is a qualitative methodology with the theoretical assumption that “social interaction is informed by institutionalized structural organizations of practices” and investigates social action.12(p303)A focus of conversation analysis is the actions of utterances or what utterances are “doing” (such as announcing, requesting, declining) in turns-at-talk and sequences in a conversation.16,17 Turns-at-talk that occur together to accomplish a joint activity among communicators—such as introducing each other or negotiating the plan of care—are sequences. 16 For each sequence, we examined the action of the utterance for which the nurse initially contributed, either by starting the sequence (such as by asking a clarifying question) or responding as part of a sequence (such as by acknowledging the proposed plan of care). We met as a team (KEP, ML, KM, MJ) to engage in analysis and discuss nurse actions of what the nurse was “doing” in their contributions to the conversation.
Categorizing Nurses’ Actions
We used summative content analysis to categorize identified nurses’ actions. Summative content analysis involves exploring the usage of certain words or content 18 ; in our analysis, we were interested in the usage of nurse actions. Similar actions were grouped together. In addition, there were few instances when nurse contributions were not made relevant to the main daily rounds conversation that were abstracted to a higher-level of action instead of the interactional action seen in conversation analysis. For example, when a nurse offered a sibling a quarter for the vending machine, the action of the utterance is “offer.” However, this “offer” was part of a side conversation between the nurse and sibling of the patient that was not made relevant to the main daily rounds conversation. Therefore, the action was coded as “attending to the family.” To increase trustworthiness of the summative content analysis, 2 researchers (KEP, MJ) reviewed and discussed each identified nurse action to ensure consistency across the dataset. We then calculated the percentages of each action relative to all the actions from the nurses’ contributions to see which were most common.
Deeper Analysis
An integral part of conversation analysis is “noticing” phenomena to then focus on for turn-by-turn analysis. 19 When categorizing nurse actions, we “noticed” 2 nurse contributions that we felt warranted further analysis with conversation analysis: (1) nurses asking questions on behalf of the family and (2) nurse responses to physician solicitations to ask a question or add information. We also calculated the percentage of each of 3 types of nurse responses to these solicitations—adding something, passing on the opportunity to add something, or first passing and then adding something. Consistent with conversation analysis, we provide excerpts and our analysis of these excerpts for the reader to determine the rigor of the analysis as it compares to the data presented.
Researcher Characteristics and Ethical Approval
None of the individuals engaged in the data analysis had any contact or relationship with study participants. Study team members have expertise in conversation analysis (KEP), nursing (KEP, ML, KM, MJ), pediatrics (EDC), and family-centered rounding (EDC). The study was reviewed and approved by the University of Wisconsin-Madison Institutional Review Board (ID#2010-1277). As part of the recruitment protocol in the RCT study, parents or guardians provided written consent and children over the age of 7 provided written assent. The University of Wisconsin-Madison Institutional Review Board also reviewed and approved this secondary data analysis (ID#2020-0688).
Results
There were 23 patients discussed in the 50 conversations; there were multiple conversations for patients who were in the hospital for longer than one day. The average length of stay was 2.96 days. Patients were on average 3.5 years of age, with the oldest being 9 years and the youngest less than 1 month. Patients were admitted for a variety of reasons, including acute illnesses, cancer treatment, and postsurgical care.
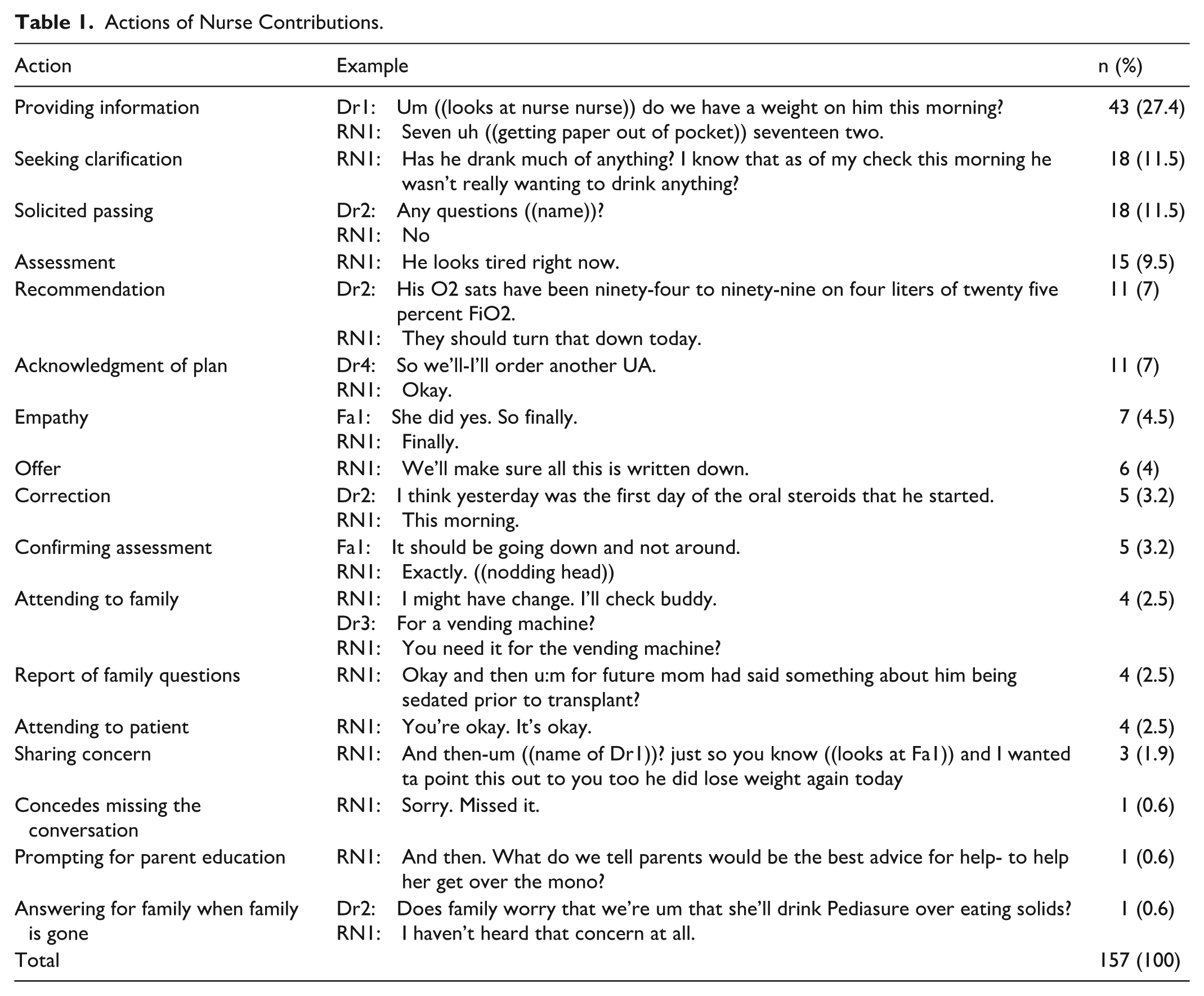
As seen in Table 1, nurse contributions varied from offering recommendations, correcting information, seeking clarification (from either the physician or the family), and acknowledging the plan of care. We will first give an overview of some of the most common actions (providing information and assessments) and then provide a closer analysis of the nurse asking questions for the family as well as nurse contributions after solicitations.
Actions of Nurse Contributions.
Providing Information and Assessments
The most common action that nurses performed was providing information (27%, Table 1). Providing information included objective information such as patient data, nurse tasks, or availability of equipment. We distinguished providing information from nurses’ assessment in that assessments only included the nurses’ subjective and often overall evaluation, such as, “he sounds like he’s still sick.”
Asking Questions for the Family
Nurses also commonly sought clarification, often about the plan of care. However, there was a distinction between when nurses asked questions that they themselves had (such as “We’re okay drawing and flushing off that lower port?”) and when they asked questions on behalf of a family member. In the latter situation, the nurse asked the question by referencing the family member, while the family member was present.
In Excerpt 1, the nurse brought up a question about the child potentially taking a multivitamin.
The nurse uses a preface that alerts everyone that a question about a multivitamin is forthcoming (line 1-2). The nurse’s gaze is on the family member, and the preface may also work to remind the family member about the question regarding the multivitamin. Both the family member’s response of a change-of-state token (“oh”), which acts as a recollection of this topic, 20 and an utterance of gratitude (“thank you,” line 3), provide evidence that they discussed the multivitamin previously with the nurse. The family member’s response, along with the gesture of pointing the finger at the nurse, also acts like a “go-ahead,” 16 in that the family member was giving the nurse permission to go ahead and continue to ask the question on the family member’s behalf. The nurse first maintains gaze on the family member and points to the family member when mentioning their name to further demonstrate that this is a topic that was initially brought up by the family member before turning to the rest of the healthcare team to introduce the issue that the patient is not getting a multivitamin (lines 5-6). The nurse again looks at the family member when additionally stating it’s a “home vitamin” that may work to affiliate and potentially ensure that the nurse is getting the facts right (lines 6-7) before looking at the team and asking about the multivitamin (line 7). The family member’s turn “so yeah” (line 8) seemed to align with the question and the gaze at the team also seemed to anticipate their answer.
Excerpt 2 is another example of the nurse asking a question for the family, in this case about vascular access.
The nurse uses “we” to signify that this is a question from both the nurse and the family member (lines 1-2). In addition, the family member expands upon the nurse’s question to include not only the option of a Hickman but also the potential for a Broviac (line 3), which further demonstrates the family member’s knowledge and alignment with this question being posed to the team.
The family members from which both Excerpts 1 and 2 were taken were very active in asking the team questions throughout the conversations. However, these examples show that even while the family member is present and active in the conversation, a role of the nurse can be to make sure that the family member’s questions are brought up to the team and answered. The affiliation with the family, both with the gaze moving back and forth in Excerpt 1 and the use of “we” in Excerpt 2, demonstrates to the team that the question is being asked on behalf of the family.
General Solicitations to Contribute
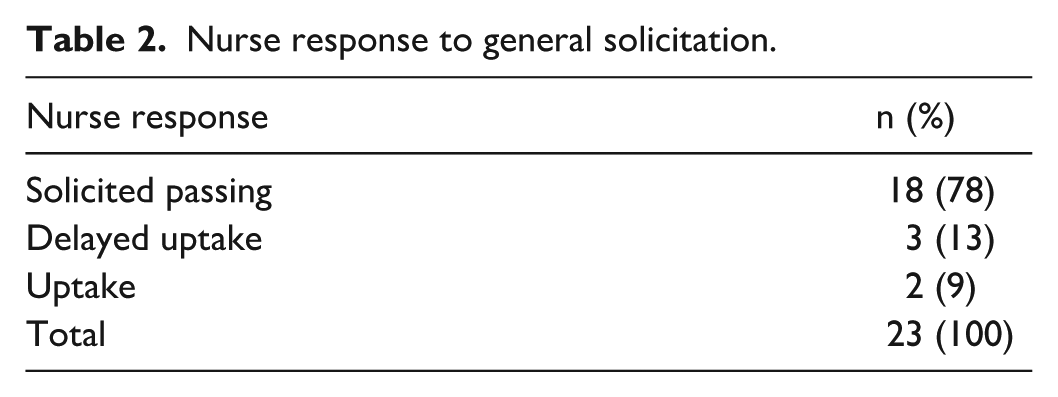
Nurses were often asked if they had any questions or anything else they would like to bring up, particularly at the end of the conversation. As has been seen with patients,21,22 this type of question provides space for nurses to bring up any concern or question that they have. However, nurses often did not contribute to the conversation when invited in this way (Table 2). This is what we have referred to as “solicited passing” in that the nurses were solicited to participate but passed on the opportunity, as shown in Excerpt 3.
Nurse response to general solicitation.
Despite being solicited first for questions (lines 1-2) and then for “anything” (line 4), the nurse passed on the opportunity by shaking their head (line 3) and verbally denying anything to add (line 5).
In the examples where nurses did contribute to the conversation in response to being solicited to participate, it was often to seek clarification about something, such as in excerpt 4.
There were a few times when the nurse answers were not as simple as denying anything to add or ask (Excerpt 3) or asking a question (Excerpt 4). Instead, nurses first denied something to add, but then asked a question or added information (Excerpts 5-7).
In Excerpt 5, the physician had just described the plan for the family member to feed the patient so that the patient may be discharged home. The physician then asked the family member if they had any questions, which they denied (not shown), before asking others if they have questions.
The first question is open to anyone else present during the rounds (line 1) before another physician (Dr4) specifically asked the nurse if they have any questions (line 2), which the nurse denied (line 3). After a “sequence-closing third” from the physician (line 4), in which the “okay” accepts the nurse’s response and moves to close the sequence to move on to something else, 16 the nurse sought clarification about how much they should try to feed the baby (lines 5, 7, 9).
In Excerpt 6, the physician asked the family member for questions, to which the family member asked about the stem cell infusion (not shown). After, the family member indicates that they did not have any other questions, as shown in line 1.
The physician asks the nurse for “anything else” (line 2), and the nurse passed on the opportunity to ask a question or provide information (line 3). After the physician opened the question to “anyone else” (line 4), the nurse then explained to the team the timing of the planned phosphorus treatment discussed earlier in the conversation (lines 5-6). After some discussion about the parent’s interest in bathing the patient (lines 10-14), the nurse also asked a clarifying question about turning off the total parenteral nutrition during the administration of stem cells, which was discussed earlier in the conversation (line 15).
In Excerpt 7, after first denying questions (“no”, line 5), the nurse uses a preface (“the only thing I was”) to introduce a question (line 5). The nurse then tells a narrative (lines 5-13) that the family had previously shared with the nurse (akin to relaying family questions as discussed in Excerpts 1 and 2), before asking the physician a question about the child’s constipation, a topic that was discussed earlier in the conversation (lines 13-14). Similar to Excerpt 1, the nurse points to the family member and moves their gaze from the family member to the physician to ask the question.
In Excerpts 5-7, the physician asked the family member for questions before asking the nurse or “anyone” to ask or add to the conversation. Although the nurse at first passed on the opportunity to ask or add, the nurse then moved on—sometimes in the same turn or sometimes in a different turn—to add information or ask a clarification question. Although some topics had just been “closed” for conversation before the nurse asked about them, other topics were talked about much earlier in the conversation before the nurse reintroduced them.
Discussion
Nurses contributed to daily rounds to accomplish a variety of actions. Although it was most common for nurses to provide information and assessments, nurses were also active in making recommendations and correcting information that was shared. Nurses also asked clarifying questions, either for themselves or on behalf of the family. However, when solicited to ask a general question or add information at the end of the conversation, nurses most often passed on the opportunity to participate, or at times, first denied having questions before asking a question or adding information.
The findings from this study align in part with an integrative review that shared the role of the nurse “was to provide a summary of the patient’s progress” (p. 12). 23 Many of the contributions of nurses involved sharing the patient’s progress, such as providing information and assessments as well as correcting information. However, an important role of the nurse identified in this study was to share the family’s questions. Nurses have reported asking questions on the family’s behalf in pediatric units during daily rounds 24 and during family meetings. 25 Our study shows how nurses engage in this task during daily rounds, likely as part of their role as an advocate. Two key aspects of advocacy in nursing are to empower patients to voice their concerns and to act as an intermediary between the patient and the physician in facilitating communication, given that nurses are consistently at the bedside and communicate more frequently with patients and families. 26 By asking the family’s questions—perhaps because the family member forgot to ask, is less comfortable asking, may feel overwhelmed during rounds, or they expected that the nurse would ask for them—nurses ensured that family concerns were heard. Future research could explore whether nurses assume a similar role in adult inpatient care, as well as patient or family perspectives on the value of this role.
When nurses were solicited to ask questions or add information at the end of the conversation, they often did not do so. Although occurring comparatively less often than an outright “no,” nurses also stated a “no” response followed by a question, which has been seen in research with patients in primary care visits. 22 Robinson and Heritage 22 found there were times when patients denied having additional questions or concerns beyond their chief concern but then asked a question or shared a concern. In particular, they found that patients first said “no” before asking a question or sharing a concern about a “non-new” problem that related to a previously diagnosed, chronic condition (regarding lab work or medication) as opposed to “new” problems that had not been previously discussed with the physician. 22 “Newness” is difficult to translate to the hospital setting where there are multiple aspects of the plan of care that are discussed and addressed during daily rounds. 27 In our work, all of the topics that nurses brought up after first stating “no” were previously discussed in the conversation and in the 2 instances where nurses asked a clarifying question after a general solicitation (without saying “no” first), the topics were also previously discussed in the conversation. Therefore, the “newness” of the topic does not seem to fit the reasoning for why the response is first “no” followed by a question or information. One possibility is that the nurse knows the topic has already been discussed and is unsure whether the physician is open to discussing the topic again, particularly in front of the family or when discharge is imminent. Future research is necessary to determine why there are instances where nurses first deny a question or concern before responding with a question or concern. Such work could help to illuminate potential efficiencies in care and discharge planning, where such questions or topics are raised as soon as possible during the patient’s stay.
It is possible that soliciting nurses for general concerns or questions earlier in the conversation may lead to more nurse responses and, subsequently, more nurse engagement. Research has shown that question-seeking and concern-seeking questions that are asked earlier in the conversation are more likely to result in patients sharing questions or concerns than when these questions are asked at the end of the conversation.21,28 In addition, research has shown that a welcoming environment is helpful for nurses to “speak up” in rounds, 24 and having nurses involved from the beginning of the conversation may help to create that environment. However, it is also possible that nurses did not engage at the end of the conversation in response to a general solicitation because they engaged throughout the conversation to ask questions or contribute information in-the-moment when certain topics were being discussed between the team and the family. When deciding among the multiple models of interdisciplinary rounds to adopt into practice, clinicians should consider whether the model allows for active participation of nurses throughout the conversation, not just at the end, to fulfill their role in the care of the patient and family.
This study has several limitations. Because this is a secondary analysis of a study in which nurse communication was not the original focus, we do not have demographic information on the nurses. It is possible that nurse contributions may vary based on characteristics such as familiarity with the team, time in practice, or degree obtained, and the single-site study may have limited the heterogeneity of nurses. In addition, the site includes learners where resident physicians and medical students participate in rounds, which limit the generalizability to institutions without these roles. Another limitation is that half of the included conversations used the RCT checklist. The checklist was a bundle of steps to facilitate family-centered rounds and included items for having the nurse present and soliciting the nurse for questions. These items likely increased the number of times physicians solicited the nurse for questions during daily rounds. However, our analysis was not focused on whether physicians solicited the nurse for questions; rather, the focus was how nurses contributed to conversations, specifically how they responded when solicited for questions. As noted in our analysis, most nurses did not contribute to the conversation in response to such solicitations. Nevertheless, it is possible that consistently being asked to contribute to the conversation led to nurses feeling more comfortable contributing to subsequent conversations. Lastly, the data used for this analysis are video-recordings of conversations, which cannot account for how nurses felt about the daily rounds conversations. For example, it is possible that nurses who had minimal contributions during daily rounds had consistent communication with the medical team throughout the day, making further questions or clarifications during rounds unnecessary. Future research should explore nurse contributions along with their perception of their participation in daily rounds.
Conclusions
Nurse contributions to pediatric daily rounds demonstrate that a normative role for nurses is to provide information or assessments, which is consistent with prior work. We also found that nurses demonstrated their role as an advocate in making recommendations to the plan of care as well as asking questions on behalf of the family. However, when asked if they had questions or would like to add information, nurses often passed on this opportunity or first denied having anything to add before proceeding to ask a question or providing information. Nurses play an important role doing daily rounds and utilizing a model for interdisciplinary rounds that allows for active nurse engagement and comfort in asking questions or sharing concerns is important for developing the patient’s plan of care.
Supplemental Material
sj-docx-1-wjn-10.1177_01939459261438893 – Supplemental material for Nurse Contributions to Daily Rounds
Supplemental material, sj-docx-1-wjn-10.1177_01939459261438893 for Nurse Contributions to Daily Rounds by Kristen E. Pecanac, Mariah Larson, Kristin Merss, Michael Jaeb and Elizabeth D. Cox in Western Journal of Nursing Research
Footnotes
Ethical Considerations
The study was reviewed and approved by the University of Wisconsin-Madison Institutional Review Board (2010-1277). The University of Wisconsin-Madison Institutional Review Board also reviewed and approved this secondary data analysis (2020-0688).
Consent to Participate
Parents provided written consent and children ages 7 to 14 years old provided written assent prior to participation.
Author Contributions
Kristen Pecanac: Conceptualization, Formal analysis, Writing—Original draft; Mariah Larson: Formal analysis, Writing—review and editing; Kristin Merss: Formal analysis, Writing—review and editing; Michael Jaeb: Formal analysis, Writing—review and editing; Elizabeth D. Cox: Conceptualization, Data curation, Funding acquisition, Writing—review and editing
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The data analyzed were collected with the support of an Agency for Healthcare Research and Quality Health Services Research Dissemination and Demonstration grant [R18 HS018680] to Dr. Cox. Dr. Cox is also supported by the National Patient Safety Foundation, the Arthur Vining Davis Foundation and the National Center for Advancing Translational Sciences grant 9U54TR000021. The sponsors did not have a role in study design; the collection, analysis and interpretation of data; the writing of the report; or the decision to submit the article for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The participants of this study did not give written consent for their data to be shared publicly, so due to the sensitive nature of the research supporting data is not available.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.