
Abstract
Background:
Insomnia is highly prevalent during pregnancy, but the role of modifiable cognitive and behavioral factors remains understudied.
Objective:
We aimed to investigate factors associated with insomnia symptoms in pregnant women, with a focus on sleep-related psychological and behavioral factors.
Methods:
A cross-sectional study was conducted among 545 pregnant women recruited from 2 tertiary hospitals in Eastern China (December 2023-March 2024). Participants completed self-reported questionnaires assessing insomnia severity, pregnancy-related rumination, physical discomfort, anxiety symptoms, depressive symptoms, presleep arousal, dysfunctional sleep-related cognitions, maladaptive sleep habits, and demographic information. Univariable and binary logistic regression were used to identify factors associated with insomnia symptoms.
Results:
Among the 545 participants (mean age = 29.1 years), 27.0% reported insomnia symptoms. In the regression model, insomnia was significantly associated with prepregnancy insomnia symptoms (OR = 2.82; 95% CI, 1.69-4.70; P < .001), increased physical discomfort (OR = 1.05; 95% CI, 1.01-1.09; P = .012), higher presleep arousal (OR = 1.13; 95% CI, 1.07-1.20; P < .001), dysfunctional sleep-related cognitions (OR = 0.95; 95% CI, 0.92-0.98; P < .001), and maladaptive sleep habits (OR = 1.03; 95% CI, 1.01-1.05; P = .005).
Conclusion:
Insomnia during pregnancy is associated with prepregnancy insomnia, physical discomfort, and key modifiable perpetuating factors including presleep arousal, dysfunctional sleep-related cognitions, and maladaptive sleep behaviors. Interventions targeting these modifiable factors are needed to improve insomnia symptoms in pregnant women.
Introduction
Insomnia, characterized by difficulties in initiating or maintaining sleep, is associated with adverse daytime outcomes such as fatigue, mood disturbances, cognitive impairments, and dissatisfaction with sleep quality. 1 Overall, 38.2% of pregnant women experience insomnia symptoms. 2 The prevalence varies significantly by trimester, with a higher rate observed in the third trimester (39.7%) than in the first (25.3%) and second (27.2%) trimesters. 2 Persistent insomnia poses long-term risks, including gestational hypertension, 3 perinatal depression, 4 lower health-related quality of life, 5 miscarriage, 4 and low infant birth weight. 4 Addressing insomnia may help mitigate these risks and improve maternal and neonatal health outcomes.
Existing research has examined diverse contributors to insomnia during pregnancy, including demographic factors (eg, age, education, economic status, occupation, body mass index [BMI]),5-7 pregnancy-related factors (eg, trimester, pregestational insomnia, physical discomfort),5,7 and psychological factors (eg, depression, anxiety, sleep-related cognitions, pregnancy pressure).7,8 However, findings are inconsistent, and variable selection often lacks grounding in established theoretical models, limiting comprehensive exploration of insomnia contributors.
The three-factor (3P) model of insomnia, a widely accepted model, 9 posits that insomnia results from a combination of predisposing (inherent characteristics that increase susceptibility, such as female sex and personality traits), precipitating (external or internal events that trigger initial episodes, such as health-related changes, stress, and psychiatric conditions), and perpetuating factors (maladaptive cognitive and behavioral strategies that maintain insomnia). 10 Within this model, cognitive factors refer to dysfunctional sleep-related cognitions (eg, unrealistic sleep expectations, catastrophizing sleeplessness) and presleep arousal (eg, cognitive and somatic arousal), while behavioral factors encompass maladaptive sleep habits (eg, irregular schedules, extended time in bed, daytime napping).10,11 During pregnancy, physiological and psychosocial changes may act as precipitating factors, while maladaptive cognitive and behavioral patterns, as perpetuating factors, may sustain chronic insomnia. 12 Given the potential risks of pharmacological treatments during pregnancy, non-pharmacological approaches, especially those targeting modifiable cognitive and behavioral factors, are particularly pertinent.13,14 However, prior studies have predominantly focused on predisposing and precipitating factors, with limited and inconsistent examination of perpetuating factors. Thus, the role of sleep-related cognitive and behavioral factors in insomnia symptoms among pregnant women remains understudied.
While some studies indicate that positive sleep beliefs and attitudes are linked to adequate sleep duration,13,14 the existing evidence comes primarily from nonclinical populations (eg, undergraduates). Whether these associations extend to pregnant women remains unclear. Kalmbach et al. (2020) found that pregnant women with insomnia reported higher nocturnal cognitive arousal and pregnancy-specific rumination than those without insomnia. 15 However, this study was limited to mid-to-late pregnancy, with only a few confounders (eg, poverty, race, BMI) controlled. Conversely, Wang et al. (2020) identified factors such as physical discomfort, depressive symptoms, and later gestation as associated with insomnia, but found no significant link with sleep-related cognitions 7 ; this study applied strict DSM-IV and ICD-10 diagnostic criteria (excluding subthreshold cases). The inconsistent findings regarding cognitive factors are possibly due to methodological differences, including strict diagnostic criteria and limited assessment of cognitive-behavioral factors, highlighting the need for further research that comprehensively examines modifiable psychological and behavioral contributors to insomnia during pregnancy.
We aimed to address this gap by investigating factors associated with subthreshold and clinically significant insomnia symptoms within a comprehensive theoretical framework. We selected variables theoretically aligned with the 3P model components: pregnancy-specific rumination as a predisposing factor; physical discomfort, depressive symptoms, and anxiety symptoms as precipitating factors; and presleep arousal, dysfunctional cognitions about sleep, and maladaptive sleep habits as perpetuating factors. This selection was guided by the 3P model of insomnia, 9 its perinatal adaptation, 12 and Morin’s cognitive-behavioral model. 11 Elucidating these factors’ contributions to insomnia, particularly the understudied perpetuating cognitive and behavioral elements, may inform targeted non-pharmacological interventions to improve sleep health in pregnant women.
Methods
Study Design
A cross-sectional design was employed, and the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) checklist for cross-sectional studies was used to guide the reporting of information.
Participants
The study was conducted in 2 tertiary hospitals in Yangzhou City, Jiangsu Province, Eastern China, between December 2023 and March 2024. The inclusion criteria included Chinese pregnant women who were as follows: (1) aged 18 years or older, (2) in any trimester of pregnancy, and (3) able to communicate in Mandarin. The exclusion criteria included participants who: (1) were currently taking sleeping pills or other sleep-affecting medications, (2) had crossed time zones during flights or worked night shifts during pregnancy, and (3) had active medical or psychiatric conditions likely to substantially disrupt sleep (eg, uncontrolled hypertension, unstable diabetes, major depressive disorder, or bipolar disorder). These criteria isolated pregnancy-related insomnia symptoms from pharmacological, circadian, and primary medical/psychiatric confounders.
Sample size for prevalence estimation was calculated using a single proportion formula based on a meta-analyzed insomnia prevalence of 38.2%, 2 95% CI, and 5% margin of error, yielding a sample of 363. Accounting for 10% nonresponse, the required sample size was 404. We recruited 545 participants, exceeding prevalence estimation requirements. For the logistic regression analysis involving 27 candidate predictors, the event per predictor variable (EPV) was calculated as 147 (insomnia cases in this study) ÷ 27 ≈ 5.4, which meets the minimum threshold (EPV ≥5) recommended for exploratory analyses. 16 The final model retained 5 significant predictors (EPV = 147/5 = 29.4), ensuring stable coefficient estimates.
Study Procedures
Participants were recruited using convenience sampling; pregnant women receiving prenatal care at the obstetrics clinics were consecutively approached and invited to participate. A registered nurse with a master’s degree approached interested women to assess eligibility and explain the study. After obtaining written informed consent, paper questionnaires were distributed to eligible participants, who completed them independently on-site. The nurse collected the questionnaires and promptly reminded participants to complete any missing or unclear responses.
Ethical Considerations
Ethics approvals were granted by the Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster (UW 23-588) and the Ethics Committee of the School of Nursing, Yangzhou University (YZUHL20230103).
Measures
Insomnia Symptoms
The validated Chinese version of the 7-item Insomnia Severity Index (ISI) was used to assess insomnia symptoms.17,18 Participants rated the severity of their symptoms over the past 2 weeks on a 5-point scale (0 = not at all to 4 = extremely), resulting in total scores ranging from 0 to 28. Higher scores indicated greater severity of insomnia, with the following classification: absence of insomnia (0-7), subthreshold insomnia (8-14), moderate insomnia (15-21), and severe insomnia (22-28). 17 The original validation study 17 reported an internal consistency (Cronbach’s alpha) of 0.74. Per established ISI criteria, participants were categorized into 2 groups: those with insomnia symptoms (ISI >7) and those without insomnia symptoms (ISI ≤7). 19 Cronbach’s alpha in this study was 0.881.
Pregnancy-Related Rumination
Two questions adapted from the work of Kalmbach et al were used to assess the positive and negative thoughts about pregnancy. 15 Participants rated the intensity of “happy thoughts about pregnancy when trying to fall asleep,” and “worry or stressful thoughts about pregnancy or the new infant.” Both items were rated on a 5-point scale (1 = not at all to 5 = extremely), resulting in a total score range of 2 to 10. 15 Although the two-item scale demonstrated a moderate reliability, with a Spearman-Brown coefficient of 0.585 in this study, 20 it may be considered acceptable given the limited number of items.
Physical Discomforts
The 16-item pregnancy symptoms questionnaire, developed based on a comprehensive review of prevalent pregnancy symptoms in the literature,21,22 was used to assess physical discomforts during pregnancy. Participants rated the frequency of each symptom on a 4-point scale (0 = never, 3 = often), with total scores ranging from 0 to 48. Higher scores indicated greater frequency of pregnancy-related physical discomfort. The content validity of the questionnaire was evaluated by a multidisciplinary expert panel (N = 8), comprising 2 obstetricians, 4 midwives, and 2 sleep medicine specialists. The scale-level content validity index (S-CVI) was 0.92. Cronbach’s alpha in this study was 0.803.
Participants who reported experiencing any symptom (scored “1” or above) were further asked to rate the extent to which the symptom impacted their sleep. Responses were scored on a 3-point scale, ranging from 1 (not limited at all) to 3 (limited a lot), with total scores ranging from 16 to 48. Higher scores indicated greater physical discomfort affecting sleep.
Anxiety Symptoms
The validated Chinese version of the 7-item Generalized Anxiety Disorder-7 (GAD-7) was used to assess anxiety symptoms.23,24 Participants rated the frequency of symptoms experienced over the past 2 weeks on a 4-point Likert scale (0 = not at all, 3 = nearly every day), with total scores ranging from 0 to 21. Higher scores indicated greater severity of anxiety symptoms, and a score of 5 or higher was used to identify the presence of mild or more severe anxiety. 23 The GAD-7 reported excellent internal consistency (Cronbach’s alpha = 0.92) and good test-retest reliability (intraclass correlation = 0.83). 23 Cronbach’s alpha in this study was 0.889.
Depressive Symptoms
The validated Chinese version of the 5-item short form of the Edinburgh Postnatal Depression Scale (EPDS-Dep-5) was used to assess depressive symptoms.25,26 Participants with a total score of 4 or higher were identified as having depressive symptoms. The Chinese validation study of the EPDS-Dep-5 demonstrated good internal consistency, with a Cronbach’s alpha of 0.759. 26 Cronbach’s alpha in this study was 0.654.
Presleep Arousal
The validated Chinese version of the 16-item Pre-Sleep Arousal Scale (PSAS) was used to measure participants’ level of arousal at bedtime.27,28 Participants rated each item based on their experiences using a 5-point scale, ranging from 1 (not at all) to 5 (extremely), with higher scores indicating more severe arousal. The Chinese version of the PSAS has demonstrated strong internal consistency, with Cronbach’s alpha coefficients ranging from 0.80 to 0.89 for the total score. 28 Cronbach’s alpha in this study was 0.881.
Dysfunctional Cognitions
The validated Chinese version of the 16-item Dysfunctional Beliefs and Attitudes about Sleep (DBAS-16) scale was used to assess dysfunctional sleep-related cognitions.29,30 For the Chinese version of the DBAS-16, participants rated each item on a 5-point Likert scale, from 1 (strongly agree) to 5 (strongly disagree). 29 The total scores ranged from 16 to 80. Lower scores indicated higher levels of dysfunctional sleep-related cognitions. The Chinese version has demonstrated satisfactory psychometric properties, including a Cronbach’s alpha of 0.786 and a test-retest reliability coefficient of 0.928. 29 Cronbach’s alpha in this study was 0.886.
Maladaptive Habits
The validated Chinese version of the 30-item Sleep Hygiene Practice Scale (SHPS) was used to assess maladaptive habits related to sleep. 31 Participants rated their engagement in these practices on a 6-point Likert scale (1 = never to 6 = always), resulting in total scores ranging from 30 to 180. Higher scores indicated poorer sleep hygiene practices. The SHPS subscales demonstrated acceptable internal consistency, with Cronbach’s alpha values ranging from 0.58 to 0.82. 31 Cronbach’s alpha in this study was 0.874.
Sociodemographic and Pregnancy-Related Factors
Sociodemographic characteristics and pregnancy-related factors included age (years), educational level (high school or below, associate’s degree, bachelor’s degree, master’s degree or higher), employment status (employment-paid leave, employment-working, unemployment), prepregnancy BMI, trimesters (first, second, third), insomnia symptoms before this pregnancy (no or yes), marital relationship (very satisfied, satisfied, neutral), and other variables as detailed in Table 1.
Demographic and Clinical Characteristics of the Included Participants by Insomnia Symptoms Category (N = 545).
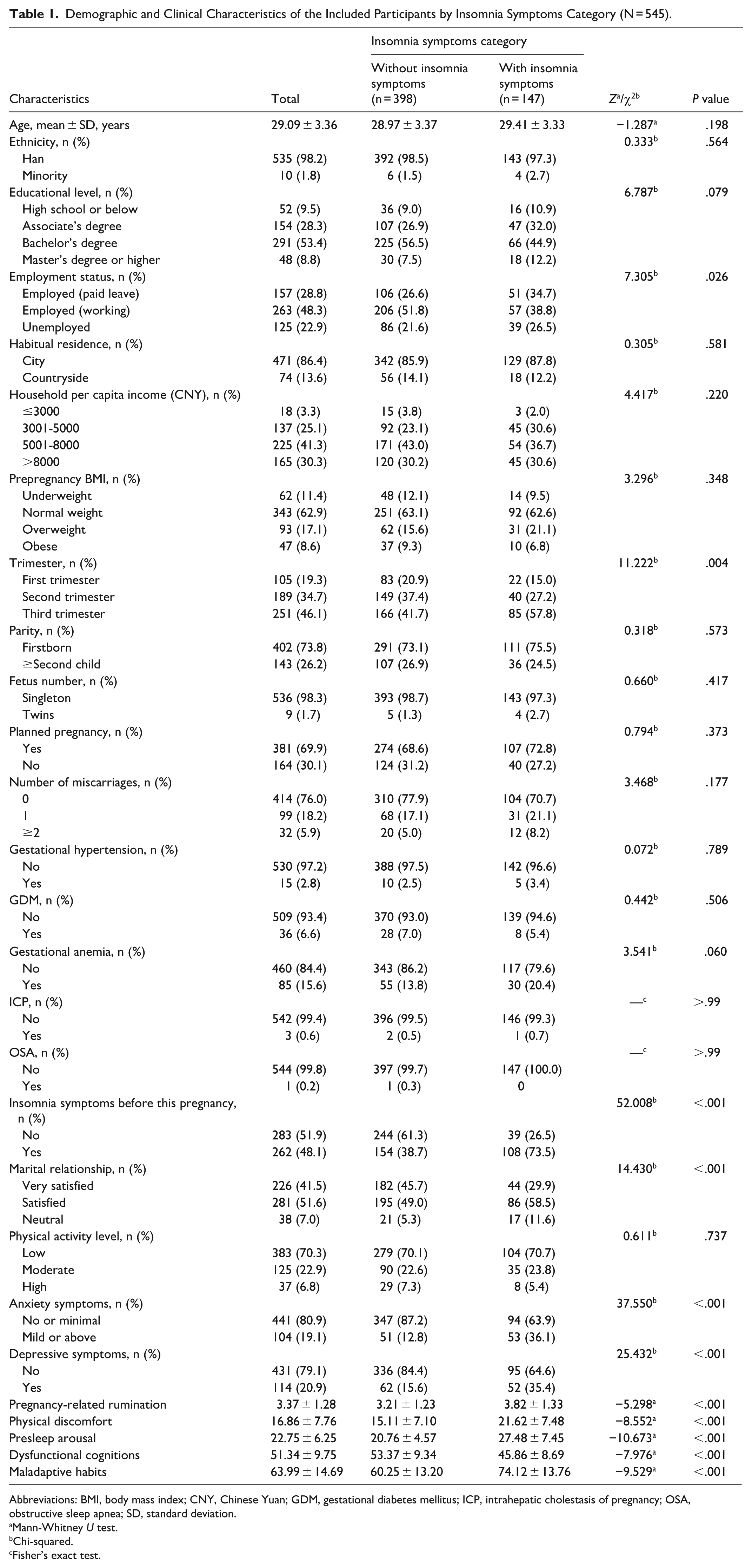
Abbreviations: BMI, body mass index; CNY, Chinese Yuan; GDM, gestational diabetes mellitus; ICP, intrahepatic cholestasis of pregnancy; OSA, obstructive sleep apnea; SD, standard deviation.
Mann-Whitney U test.
Chi-squared.
Fisher’s exact test.
Data Analysis
Data analyses were conducted using IBM SPSS Statistics for Windows, version 30.0 (IBM Corp., Armonk, N.Y., USA). Respondents with missing data were excluded to ensure the integrity and reliability of the study findings. For univariable analysis, differences in continuous independent variables between participants with (ISI >7) and without insomnia symptoms (ISI ≤7) were assessed using independent-samples t-tests for approximately normally distributed variables or the nonparametric Mann-Whitney U test for skewed variables. Categorical variables were compared using chi-squared or Fisher’s exact tests to identify preliminary group differences. Binary logistic regression analysis included variables screened from univariable analysis at P < 0.2, a widely used liberal screening threshold to minimize type II error and retain potential confounders. 32 Multicollinearity was assessed using variance inflation factors (VIF), with VIF >5 indicating potential multicollinearity. 33 Model fit was evaluated using the Hosmer-Lemeshow goodness-of-fit test, with P ≥ .05 indicating adequate fit. 34 Statistical significance was determined at P < .05 (two-tailed).
Results
Participant Characteristics
Among the 575 pregnant women initially enrolled, 30 did not complete the questionnaire, resulting in a final sample size of 545 and a completion rate of 94.8%. The average age of participants was 29.1 ± 3.4 years. The numbers of participants in the first, second, and third trimesters were 105 (19.3%), 189 (34.7%), and 251 (46.1%), respectively. Most women were experiencing their first pregnancy (73.8%) and carrying a singleton (98.3%). Most had planned their current pregnancies (69.9%), reported no history of miscarriage (76.0%), and had no comorbid pregnancy conditions. The demographic and clinical characteristics of the participants are presented in Table 1.
Insomnia Severity, Predisposing, Precipitating, and Perpetuating Factors
The average ISI score among pregnant women was 5.27 ± 4.04, with 27.0% (n = 147) categorized as having insomnia symptoms. Among all pregnant women, 24.4% (n = 133) had subthreshold insomnia, 2.6% (n = 14) had moderate insomnia, and none had severe insomnia.
The average pregnancy-related rumination score for predisposing factors was 3.37 ± 1.28. Concerning precipitating factors, the average score was 16.86 ± 7.76 for physical discomfort. The top 5 physical discomforts that significantly disrupted pregnant women’s sleep were urinary frequency (n = 77, 14.1%), difficulty finding a comfortable sleep position (n = 50, 9.2%), hip/pelvic pain (n = 41, 7.5%), joint/back/rib pain (n = 24, 4.4%), and reflux/heartburn (n = 20, 3.7%). Approximately 20% of participants experienced symptoms of anxiety or depression. Regarding perpetuating factors, the average scores were 22.75 ± 6.25 for presleep arousal, 51.34 ± 9.75 for dysfunctional sleep-related cognitions, and 63.99 ± 14.69 for maladaptive sleep habits.
Factors Related to Insomnia Symptoms
Univariable analysis showed that employment status (χ2 = 7.305, P = .026), trimesters of pregnancy (χ2 = 11.222, P = .004), insomnia symptoms before pregnancy (χ2 = 52.008, P < .001), and marital relationship (χ2 = 14.430, P < .001) had significant differences between pregnant women with and without insomnia symptoms. Mild or worse anxiety symptoms were more prevalent in the insomnia group (36.1%) than in the non-insomnia group (12.8%) (χ2 = 37.550, P < .001). Similarly, depressive symptoms were more common in participants with insomnia symptoms (35.4%) than in those without (15.6%) (χ2 = 25.432, P < .001). Pregnant women with insomnia symptoms had more frequent physical discomfort, higher levels of pregnancy-related rumination, presleep arousal, dysfunctional sleep-related cognitions, and maladaptive sleep habits than those without insomnia symptoms (all P < .001). Table 1 shows the full results.
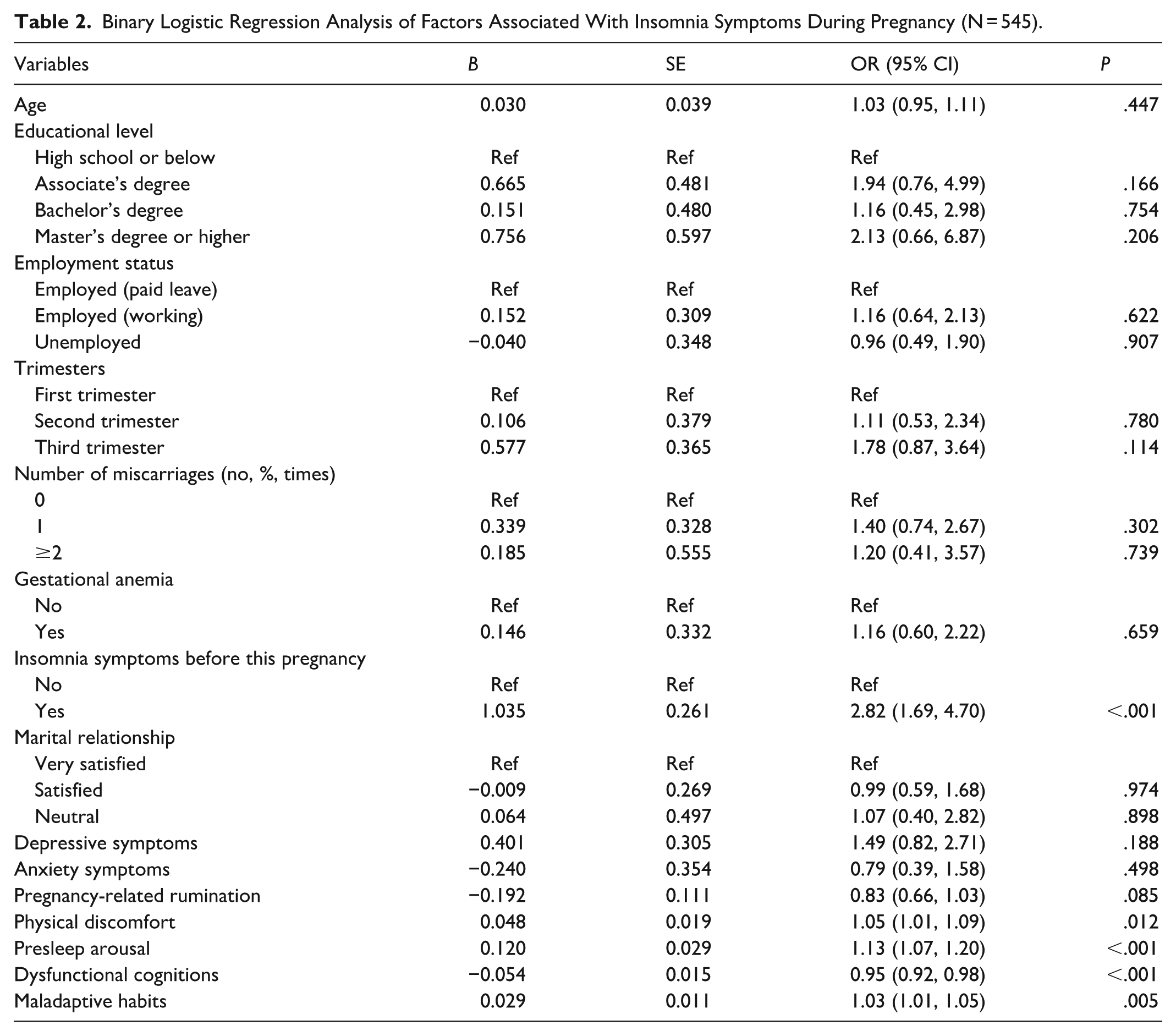
All VIF values ranged from 1.08 to 2.35, indicating no significant multicollinearity among independent variables. The nonsignificant Hosmer-Lemeshow test (χ2 = 6.74, df = 8, P = .565) suggests no major discrepancies between model predictions and observations.
Table 2 shows the results of binary logistic regression analysis. In the multivariable model, 5 factors were independently associated with insomnia symptoms during pregnancy. Prepregnancy insomnia symptoms were associated with higher odds of insomnia (OR = 2.82; 95% CI, 1.69-4.70; P < .001). Greater physical discomfort was positively associated with insomnia symptoms (OR = 1.05; 95% CI, 1.01-1.09; P = .012). Higher presleep arousal was associated with increased odds of insomnia symptoms (OR = 1.13; 95% CI, 1.07-1.20; P < .001). More dysfunctional sleep-related cognitions (lower DBAS-16 scores) were associated with greater insomnia risk (OR = 0.95; 95% CI, 0.92-0.98; P < .001). Maladaptive sleep habits were positively associated with insomnia symptoms (OR = 1.03; 95% CI, 1.01-1.05; P = .005).
Binary Logistic Regression Analysis of Factors Associated With Insomnia Symptoms During Pregnancy (N = 545).
Discussion
Our study found a high prevalence of insomnia symptoms during pregnancy, especially among women with a pre-gestational history of insomnia and those reporting greater physical discomfort. In the Chinese pregnant population, these results provide empirical support for the 3P model’s perpetuating factors by identifying 3 modifiable, independently associated targets: pre-sleep arousal, dysfunctional sleep-related cognitions, and maladaptive sleep habits. By quantifying these associations in Chinese pregnant women, our study offers an evidence base for tailoring interventions.
We observed that pre-gestational insomnia history was associated with insomnia symptoms during pregnancy, consistent with a Spanish cohort study on prior insomnia and its persistence across all gestational trimesters. 6 This finding aligns with the 3P model’s predisposing factors,9,12 which theoretically include heritable vulnerabilities and personality traits (eg, neuroticism, introversion, and perfectionistic concerns) conferring insomnia risk. 35 While personality was not directly measured in this study, women with prepregnancy insomnia likely carry such predisposing characteristics, explaining their elevated odds of insomnia persistence during pregnancy. A history of insomnia also reflects prior exposure to precipitating and perpetuating factors of insomnia. For example, individuals with insomnia symptoms often tend to adopt maladaptive strategies to obtain more sleep. 12 Without addressing these maladaptive strategies, women may continue to use them, leading to persistent insomnia.
Our finding that physical discomfort is linked to insomnia symptoms is consistent with that of prior research. 7 We found that several pregnancy-related physical symptoms were frequently reported and associated with insomnia symptoms; the 5 most commonly endorsed sleep-disrupting complaints in our sample were urinary frequency, difficulty finding a comfortable sleep position, hip/pelvic pain, joint/back/rib pain, and reflux/heartburn. This ranking provides a specific target for symptom management in Chinese clinical settings. Such symptoms contribute to insomnia by directly causing nocturnal awakenings and sleep fragmentation. 12 Consequently, the proactive identification of these physical symptoms by both pregnant women and health care providers is crucial. While many physical discomforts are difficult to eliminate, practical lifestyle adjustments (eg, reducing evening fluid intake, using a pregnancy pillow, mindful meal timing, and posture) may attenuate their impact on sleep 36 ; the specific effectiveness and acceptability of these measures during pregnancy remain to be tested.
Higher levels of presleep arousal were significantly associated with insomnia symptoms in our study, consistent with prior cross-sectional research. 15 Presleep arousal typically consists of cognitive and somatic arousal. 27 Elevated cognitive hyperarousal often leads pregnant women to exert excessive effort to fall asleep, accompanied by heightened worry about sleep. Paradoxically, such efforts can inadvertently disrupt the natural sleep process.12,37 Meanwhile, heightened somatic arousal activates the stress-response system, increasing alertness and inhibiting relaxation, often manifested as muscle tension. 27 This tension itself contributes to physical discomfort, making it harder to find a restful position and further exacerbating sleep initiation and maintenance problems. Accordingly, interventions that reduce pre-sleep cognitive and somatic arousal, such as relaxation techniques and mindfulness-based approaches,13,38 are plausible strategies to relieve insomnia in pregnancy. The effectiveness of these techniques in reducing pre-sleep arousal and insomnia symptoms among pregnant women requires further evaluation.
Dysfunctional sleep-related cognitions were independently associated with insomnia symptoms in our study, which was not consistent with another Chinese cross-sectional study. 7 This discrepancy may be due to differences in participant eligibility criteria. Our study included participants regardless of prepregnancy sleep problems, whereas the other study excluded those who had sleep disturbances before pregnancy. Consequently, pregnant women in our study exhibited more dysfunctional sleep-related cognition (mean = 51.34) than those in the other study (mean = 70.40), since lower scores indicate greater dysfunction. This suggests that dysfunctional sleep-related cognitions may be particularly pronounced in pregnant women with a preexisting vulnerability to insomnia, a subgroup that is often excluded from research but highly relevant for clinical practice. Dysfunctional beliefs about sleep can promote catastrophizing and maladaptive compensatory behaviors that perpetuate insomnia, 39 so cognitive interventions such as cognitive restructuring are reasonable clinical targets. 13
Maladaptive sleep habits showed a substantial correlation with insomnia symptoms in our sample. Sleep hygiene includes recommendations for general health practices (eg, diet, exercise, and substance use), environmental conditions (like light, temperature, and noise), and behaviors related to sleep (like the regularity of sleep schedule and presleep activities). 31 Maladaptive sleep hygiene practices are believed to disrupt sleep and contribute to sleep disturbances. Chinese pregnant women commonly adhere to traditional beliefs that “pregnancy is a time for rest” to protect fetal health and stability. 40 In our study, most pregnant women were on leave or unemployed, and this cultural predilection for rest is also reflected in the high rates of sedentary behavior, with 70.3% reporting low physical activity levels. Extended rest often precipitates excessive daytime sleep and reduces energy expenditure. This, in turn, diminishes the homeostatic sleep drive and can lead to insomnia.10,41 This specific behavioral pattern of prolonged rest coupled with low physical activity observed in our cohort may be particularly amenable to intervention in this population. Pregnant women are typically receptive to lifestyle changes that improve health. 42 Health care providers could utilize this opportunity to inform and promote beneficial sleep practices among pregnant women. Although sleep hygiene education is commonly used to address maladaptive behaviors, evidence indicates it is insufficient as a standalone treatment for insomnia.1,43 Integrating sleep hygiene education with other strategies to manage insomnia symptoms during pregnancy effectively is recommended.
Factors such as age, trimester, depressive and anxiety symptoms, pregestational high BMI, physical activity, smoking habits, and pregnant nocturnal rumination were not found to be associated with insomnia symptoms during pregnancy in this study. These findings were inconsistent with previous studies.6,7,15 This may be explained by several reasons: the differences in these studies’ cultural and demographic contexts, different eligibility criteria of participants, and different criteria for insomnia.
Our results emphasize the role of perpetuating factors in the persistence of insomnia symptoms during pregnancy. The independent associations we observed with pre-sleep arousal, dysfunctional cognitions, and maladaptive habits empirically support these factors as key treatment targets in our sample. Cognitive-behavioral therapy for insomnia (CBT-I) is a multicomponent, evidence-based intervention that addresses these behavioral and cognitive drivers and has demonstrated efficacy in perinatal populations.14,44 Our findings provide empirical grounding for delivering such non-pharmacological interventions to Chinese pregnant women. Importantly, Chinese cultural and lifestyle factors, such as traditional beliefs that pregnancy is a time for rest and cultural conflicts between clinical recommendations and traditional practices around diet,40,45 may necessitate culturally adapted protocols to enhance intervention acceptability and effectiveness.
Given the high prevalence of insomnia symptoms and the strong association with pre-gestational insomnia, routine antenatal screening should be integrated into prenatal visits, with midwives and obstetric nurses trained to identify and triage high-risk women. Nurses can deliver brief, evidence-based interventions (eg, CBT-I components such as sleep restriction, stimulus control, sleep hygiene, relaxation training, and cognitive restructuring) 46 and refer complex or refractory cases to perinatal mental-health or sleep specialists. Implementing nurse-led protocols targeting these modifiable perpetuating factors may improve maternal sleep and mental health; however, randomized or longitudinal trials are needed to confirm effectiveness before broad policy adoption.
Limitations
This study has several limitations. First, the cross-sectional design used in this study does not allow for the determination of causality between independent variables and insomnia symptoms during pregnancy, as confounding factors cannot be excluded. Longitudinal studies are needed to verify the results and examine the dynamic nature of factors influencing insomnia symptoms as pregnancy progresses. Second, this study only used a self-reported questionnaire to evaluate insomnia symptoms, which may introduce bias. Future studies could utilize objective measures of insomnia to validate these findings. Third, the generalizability of our results may be limited due to the inclusion of participants from only 2 hospitals in China. Convenience sampling during routine prenatal clinic visits may introduce selection bias by systematically underrepresenting rural pregnant women or those with limited health care access. Population-based or multi-site sampling strategies are recommended for future studies to enhance representativeness.
Conclusion
The findings from our survey suggest that insomnia symptoms during pregnancy are associated with preexisting insomnia, increased physical discomfort that affects sleep, elevated levels of presleep arousal, dysfunctional cognitions, and maladaptive habits.
Footnotes
Acknowledgements
We acknowledge all participants in this study for their dedication and time.
Ethical Considerations
This study follows the guidelines of the Declaration of Helsinki. Ethics approval was obtained from the Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster (UW 23-588) and the Ethics Committee of the School of Nursing, Yangzhou University (YZUHL20230103).
Consent to Participate
Written informed consent was obtained from all participants included in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (72204117). The funding body was not involved in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of the study are available from the first author upon reasonable request.