
Abstract
Background:
Patients with diabetes often experience significant psychological distress, contributing to poor diabetes self-management and complications. Meditation may reduce psychological distress, but most meditation interventions have been lengthy and burdensome to both participants and interventionists.
Purpose:
The purpose of this study was to evaluate the preliminary effects of a 4-week compassion meditation intervention with recorded Zoom sessions (30-40 minutes/session) on psychological factors (depressive symptoms, diabetes distress, self-compassion, resilience, self-esteem, and self-efficacy) in patients with type 1 or type 2 diabetes.
Methods:
In this pilot randomized controlled trial, participants were recruited via ResearchMatch. Baseline and 4-week follow-up data on all the study variables and demographic characteristics were collected via Research Electronic Data Capture from April to July 2025. After baseline, each participant was randomly assigned to the intervention or control group based on a computer-generated list of random numbers. Independent samples t-tests, Mann-Whitney U tests, paired samples t-tests, Wilcoxon signed-rank tests, and analysis of covariance were used for data analysis.
Results:
Between-group analyses showed higher levels of diabetes self-efficacy and lower diabetes distress in the intervention group (n = 17, mean age: 51.8 years) at 4-week follow-up compared with the control group (n = 29, mean age: 51.7 years). Within-group analyses showed reductions in diabetes distress and improvements in self-compassion and self-efficacy in the intervention group, while self-esteem decreased in the control group from baseline to follow-up.
Conclusions:
This brief, virtual compassionate meditation intervention showed favorable effects on several psychological factors. It may be implemented to enhance psychological statuses in patients with diabetes.
Introduction
Patients with diabetes commonly experience negative psychological states, including diabetes distress and depressive symptoms.1-4 Approximately 38% of veterans with type 2 diabetes experience moderate to high levels of diabetes distress, 2 with a mean score of 2.39 (≥2 indicating moderate-to-severe distress). 1 Depressive symptoms affect 25% to 28% of Chinese patients with type 2 diabetes.3,4 Higher levels of these negative psychological states are associated with poorer self-management and more severe diabetes complications.1,5,6 Furthermore, negative psychological status (eg, more severe diabetes distress) and poor self-management have also been associated with more severe diabetes complications, such as macrovascular (eg, cardiovascular diseases and heart failure) and microvascular diseases (eg, retinopathy, nephropathy, and neuropathy).6-9 Therefore, interventions to reduce negative psychological states are needed.
Positive psychological states are often low in this population. 10 Standardized mean scores for self-compassion, resilience, self-esteem, and self-efficacy ranged from 40 (self-esteem) to 70 (resilience) in patients with type 1 or type 2 diabetes. 10 Lower levels of positive psychological factors are associated with poorer self-management in diabetes.5,10-14 Among adult patients with diabetes, self-compassion has been most consistently associated with better self-management. 13 Resilience and self-esteem are also linked to self-management in patients with type 1 or type 2 diabetes.5,11,12 Finally, self-efficacy was related to self-management in patients with diabetes or type 2 diabetes.5,10 In diabetes, self-management is known to be poor to moderate. 10 The mean standardized scores for overall self-management and the components, including blood glucose testing, diet, foot care, and exercise, ranged from 33 (exercise) to 71.4 (blood glucose testing). 10 Therefore, positive psychological states also need to be enhanced to improve poor self-management in patients with diabetes.
Meditation is “a mind and body practice focused on interactions between the brain, mind, body, and behaviour.” 15 (p1) Meditation has been shown to reduce depressive symptoms and diabetes distress and to improve diabetes self-efficacy, self-compassion, and resilience in patients with diabetes.16-23 However, the effects of meditation on all of the negative and positive psychological states that may impact diabetes self-management, and diabetes complications have been rarely examined in patients with diabetes. More importantly, most interventions are lengthy (8-12 weekly sessions totaling 13.5-25 hours), mainly delivered in person, and may impose burdens on patients and the interventionist.16,17,19-22,24 These limitations not only reduce accessibility and feasibility for patients, particularly those with transportation difficulties, competing responsibilities, or limited financial resources, but also restrict the scalability of such interventions in real-world health care settings. As a result, patients who may benefit most from meditation-based approaches (eg, those with high levels of distress or limited self-management capacity) are often the least able to participate in or complete these intensive programs. Furthermore, the high demand for interventionists’ time and resources hinders broad implementation and sustainability. Thus, more effective meditation interventions with less burden to both patients and interventionists are needed to enhance positive psychological states and reduce negative psychological states in patients with diabetes.
We developed an asynchronous virtual weekly 4-session compassionate meditation intervention (30-40 minutes/session) to improve psychological states in patients with diabetes. In a prior study of patients with hemodialysis, 25 5 weekly virtual meditation sessions reduced depressive symptoms. The intervention of this study consists of common meditation techniques, such as breathing and relaxation with additional components of compassion.26,27 Compassionate meditation techniques, including breathing with positive phrases, compassionate body scan, and compassionate friends, are designed to enhance compassion toward the self, self-care, and the world. 28 These techniques contribute to improvements in psychological states by strengthening the desire for self-improvement, empowering own self-care, reducing rumination, and modulating sympathetic and parasympathetic nervous system activity.19,29-33 The virtual delivery of the intervention is designed to reduce the participant and interventionist burden as well as delivery costs. Therefore, the purpose of this study was to examine the preliminary effects of the short, virtual compassionate meditation on depressive symptoms, diabetes distress, self-compassion, resilience, self-esteem, and self-efficacy in adult patients with diabetes, regardless of type.
Methods
Study Design and Setting
This was a 2-arm parallel superiority randomized controlled trial to examine the effects of a 4-week compassionate meditation intervention on psychological status compared with no intervention. Potential participants were recruited from ResearchMatch, which is a national research volunteer registry in the United States. 34 The intervention group received links to prerecorded Zoom meditation sessions and educational materials on meditation, diet, and physical activities.35,36 The control group did not receive the intervention during the study period.
Randomization and Blinding
After baseline data collection, participants were assigned in a 1:1 ratio to either the intervention or control group according to a computer-generated simple randomization list developed by the study statistician. Participants could not access the randomization list. Blinding could not be implemented for participants due to the nature of the intervention. Although blindness was not implemented for the data analyst (the principal investigator), outcome bias in this study could be minimized because it was difficult for the data analyst to modify the data collected online.
Sampling Method and Sample
A convenience sampling method was used. Inclusion criteria were adults (≥18 years) with a diagnosis of diabetes; the ability to read, hear, and understand English; and with access to a smart phone, tablet, or computer. All inclusion criteria were based on self-report. No additional exclusion criteria were applied. Sample size was determined based on recommendations for pilot studies, which suggest 12 to 34/group.37,38 The planned sample size for this study was 60 (30/group). Considering an anticipated attrition rate of ~43%, 10 based on our previous recruitment experience with ResearchMatch, the final target enrollment was 104 (52/group).
Intervention and Delivery
The intervention group received the 4-week intervention sessions. We selected a 4-week format (30-40 minutes/session) to examine whether the short sessions could positively impact psychological states in patients with diabetes. Each intervention group member received the weekly intervention link to watch the prerecorded Zoom sessions and also received a standard participant manual for meditation and self-care techniques and the educational materials on medication, diet, and physical activities during week 1.35,39 The first author of this study, a trained meditation teacher, recorded the sessions according to the standard manual adapted from the interventionist manual used in our previous study. 26 The topics of session 1 included introduction of the intervention, meaning of life, and compassionate body scan 1, as well as introduction and practice of compassionate breathing techniques with positive phrases and compassionate body scan techniques. Session 2 focused on compassion, diet, and difficult emotions and introduced and practiced breathing techniques, labeling emotion techniques, and pleasure eating techniques. Session 3 focused on compassion, compassionate body scan 2, difficult relationships, emotions, and compassionate friends and introduced and practiced breathing techniques, compassionate body scan techniques, labeling emotion associated with difficult relationships techniques, and compassionate friend meditation techniques. Finally, session 4 focused on compassion, self-care meditation techniques, and the future; practicing breathing techniques, writing a self-compassion letter, and self-care meditation techniques; and discussing future plans. The research team called intervention and control groups 2 to 3 times, although the majority of them did not answer phone calls. For the control group, the research team only discussed study procedure, the participant’s progress, and/or notification of follow-up data collection; while for the intervention group, the research team discussed the intervention sessions they watched. When participants did not receive phone calls, the research team sent e-mails and/or text messages for greetings, notification of next phone call, and notification of follow-up data collection.
Procedure
This study was approved by the Mercer University Institutional Review Board (H25-04007). Research participants were recruited via announcements on ResearchMatch between April and July 2025. Written informed consent was obtained electronically from all participants after presenting the study purpose and procedure, potential benefits and risks, confidentiality, voluntary participation, and the right to withdraw without penalty. This study was conducted according to the ethics principles of Helsinki declaration. 40 Data collection was conducted online through online Research Electronic Data Capture at baseline and 4-week follow-up between April and August 2025.
Measures
Depressive symptoms were defined as the presence of affective and somatic disturbances, such as disturbances in mood, interest, energy, sleep, appetite, and concentration, and were assessed by the Patient Health Questionnaire-8 (PHQ-8). 41 The PHQ-8 consists of 8-items with a 4-point Likert scale, ranging from 0 (not at all) to 3 (nearly every day). The potential scores range from 0 to 24, with higher scores indicating more severe depressive symptoms. The PHQ-8 has been used in patients with diabetes, and the validity was supported by their relationships with diabetes distress and self-care. 1 In this study, the reliability was supported by a Cronbach’s alpha of 0.87.
Diabetes distress referred to the emotional burden and worries specific to living with and managing diabetes and was assessed by the Diabetes Distress Scale. 42 The Diabetes Distress Scale consists of 17 items with a 6-point Likert scale, ranging from 1 (not a problem) to 6 (a very serious problem). The potential total scores range from 1 to 6, with higher scores interpreted as more diabetes distress. 42 The validity was supported by its relationship to depressive symptoms assessed by the Center for Epidemiologic Studies—Depression Scale. 42 The reliability was supported by a Cronbach’s alpha of 0.93 in the previous study 6 and a Cronbach’s alpha of 0.95 in this study.
Self-compassion was defined as the tendency to be kind and understanding toward oneself in instances of pain or failure and assessed by the Self-Compassion Scale—Short Form. 43 It consists of 12 items with a 5-point Likert scale ranging from 1 (almost never) to 5 (almost always). The potential total scores range from 1 to 5 (calculated as the mean score), with higher scores indicating higher levels of self-compassion. The validity was supported by satisfactory structural validity. 43 The reliability was supported by a Cronbach’s alpha of 0.87 in a prior diabetes study 6 and in this study.
Resilience referred to the ability to cope with and adapt to stress, adversity, or challenges and was measured by the revised version of the Connor-Davidson Resilience Scale.44,45 It consists of 10 items with a 5-point Likert scale ranging from 0 (not true at all) to 4 (true nearly all the time). The potential total scores range from 0 to 40, with higher scores indicating greater resilience. 45 The validity was supported by its relationship to diabetes stigma. 46 The reliability was supported by a Cronbach’s alpha of 0.90 in a prior diabetes study 6 and a Cronbach’s alpha of 0.87 in this study.
Self-esteem was defined as an individual’s overall evaluation of their own worth and assessed by the Rosenberg Self-Esteem Scale.47,48 It consists of 10 items with a 4-point Likert scale ranging from 1 (strongly agree) to 4 (strongly disagree). The potential total scores range from 10 to 40 with higher scores indicating higher levels of self-esteem. The validity was supported by its relationship to diabetes self-management. 5 The reliability was supported by a Cronbach’s alpha of 0.93 in a prior study 6 and a Cronbach’s alpha of 0.89 in this study.
Self-efficacy referred to an individual’s confidence in their ability to manage diabetes-related tasks and behaviors effectively and was assessed by the Perceived Diabetes Self-Management Scale. 49 It consists of 8 items with a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). The potential total scores range from 8 to 40, with higher scores indicating greater perceived self-efficacy in diabetes self-management. The validity was supported by satisfactory structural validity. 49 The reliability was supported by a Cronbach’s alpha of 0.88 both in a prior diabetes study 6 and in this study.
Demographic characteristics, including age (years), education (years), and duration since diabetes diagnosis (years), were collected using a standard Demographic Questionnaire. In addition, data on body weight (pounds) and height (feet and inches) were collected using the same instrument via self-report. Body weight was converted to kilograms, and height was converted to meters. Body mass index was then calculated using the formula: weight (kg)/height (m2).
Data Analysis
All data analyses were performed using SPSS Statistics for Windows (version 31.0; IBM Corp, Armonk, NY, USA). Means with standard deviations and medians with interquartile ranges were calculated to describe sample characteristics and study outcome variables. Normality was tested for all continuous variables using the Kolmogorov-Smirnov test.
For between group comparisons, Mann-Whitney U tests were used to compare the medians of education, duration since diabetes diagnosis, depressive symptoms, diabetes distress, and self-compassion between the intervention and control groups at baseline. Independent samples t-tests were used to compare the means of age, body mass index, resilience, self-esteem, and self-efficacy between the 2 groups at baseline.
For between group comparisons, independent samples t-tests were used to compare means of diabetes distress, self-compassion, resilience, and self-efficacy between the 2 groups at follow-up. Mann-Whitney U tests were used to compare medians of depressive symptoms between the 2 groups at follow-up. Analysis of covariance was used to compare the means of self-esteem between the 2 groups, controlling for the baseline score due to a significant group difference.
For within-group comparisons, paired samples t-tests were used to compare mean changes in the outcomes from baseline to follow-up within each group, and Wilcoxon signed-rank tests were used to compare median changes where appropriate. A significance level <.05 and 2-tailed tests were applied to all analyses.
Results
In total, 87 participants completed baseline data collection, but 1 participant assigned to the intervention group was excluded due to more than 30% missing items on each of several instruments, 50 before receiving the intervention links. Forty-six out of 86 (17 in the intervention group and 29 in the control group) completed follow-up data collection (Figure 1). There were no statistical differences in the demographic characteristics or study outcomes between completers and non-completers at baseline.
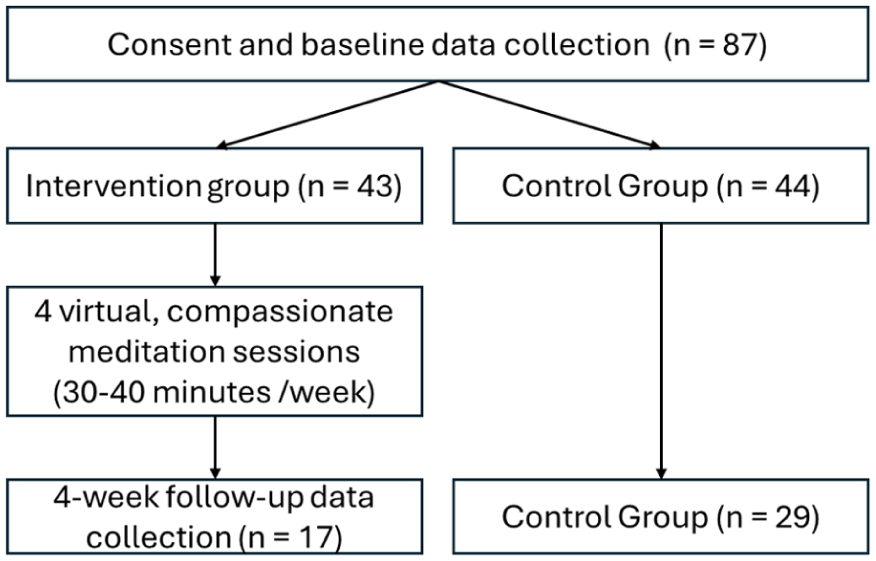
Study flow.
The descriptive data of continuous sample characteristics and study outcomes in the total sample, in the intervention group, and in the control group are presented in Table 1. There were no group differences in the sample characteristics, including age, education level, body mass index, and duration since diagnosis of diabetes. The mean age in the intervention group (n = 17) and the control group (n = 29) was 51.8 and 51.7 years, respectively (P = .984). The median education level in both groups were 16.0 and 16.0 years, respectively (P = .918). The mean body mass index in both groups was 33.9 and 30.9 kg/m2, respectively (P = .239). The median duration since diagnosis of diabetes between the 2 groups was 12.0 and 8.0 years, respectively (P = .254). There was no group difference in race and ethnicity (58.8% white in the intervention group vs 65.5% white in the control group, P = .650).
Sample Characteristics and Study Variables.
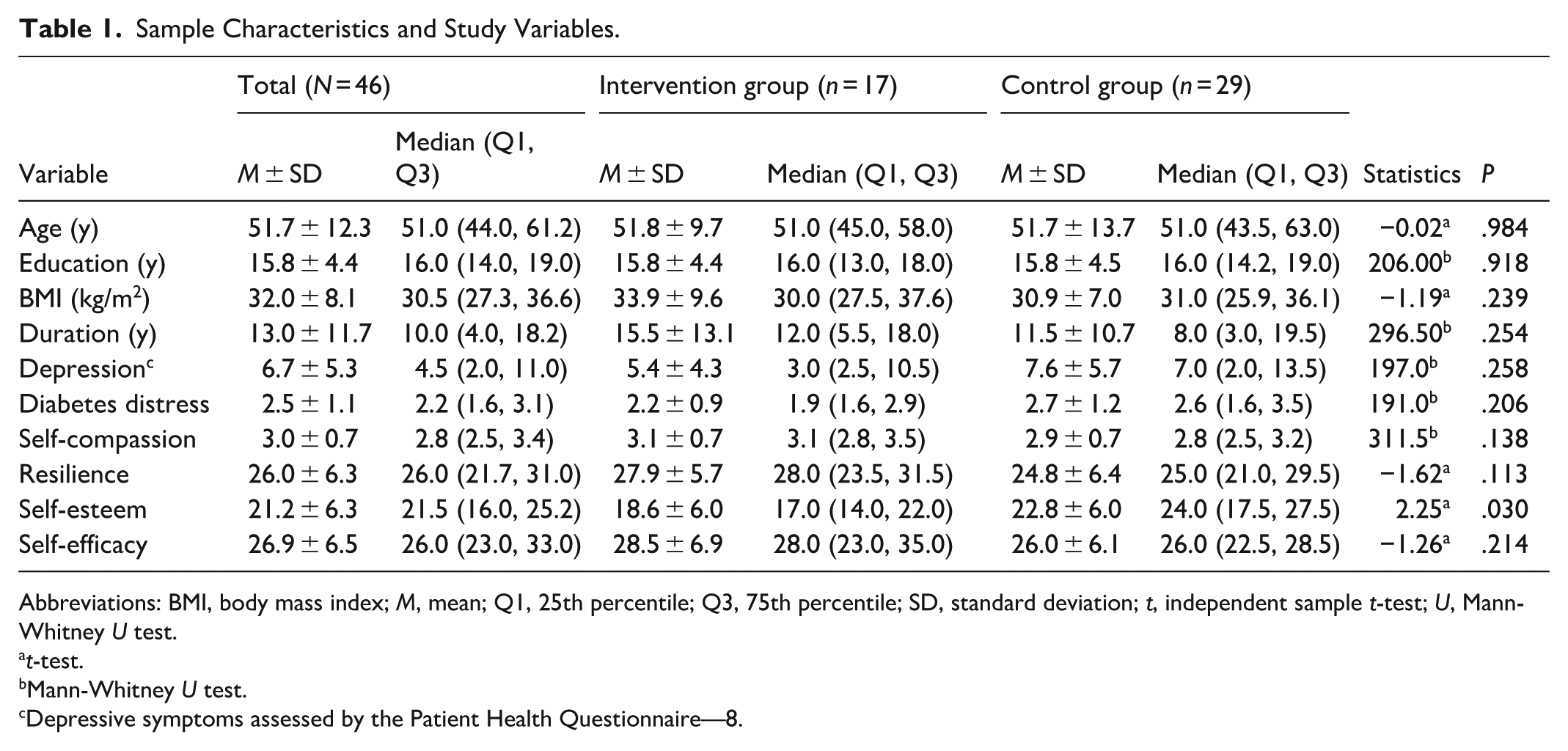
Abbreviations: BMI, body mass index; M, mean; Q1, 25th percentile; Q3, 75th percentile; SD, standard deviation; t, independent sample t-test; U, Mann-Whitney U test.
t-test.
Mann-Whitney U test.
Depressive symptoms assessed by the Patient Health Questionnaire—8.
The levels of depressive symptoms were relatively low (mean = 6.7; cutoff for depressive symptoms = 10), whereas the levels of diabetes distress were relatively moderate to high (mean = 2.5; cut point for moderate and severe distress ≥2). The standardized scores for self-compassion, resilience, self-esteem, and self-efficacy were 50.0, 65.0, 37.3, and 59.1 out of 100, respectively, suggesting relatively lower levels of these positive psychological attributes. Among all the outcome variables, only self-esteem showed group difference at baseline (P = .030).
In between-group analyses, the mean score of diabetes distress in the intervention group at follow-up was lower than that in the control group (1.8 vs 2.5, P = .030), indicating a favorable intervention effect (Table 2). The mean score of diabetes self-efficacy in the intervention group at follow-up was higher than that in the control group (31.4 vs 27.2, P = .037), indicating a favorable intervention effect.
Effects of Meditation Intervention on Psychological Factors (N = 46).
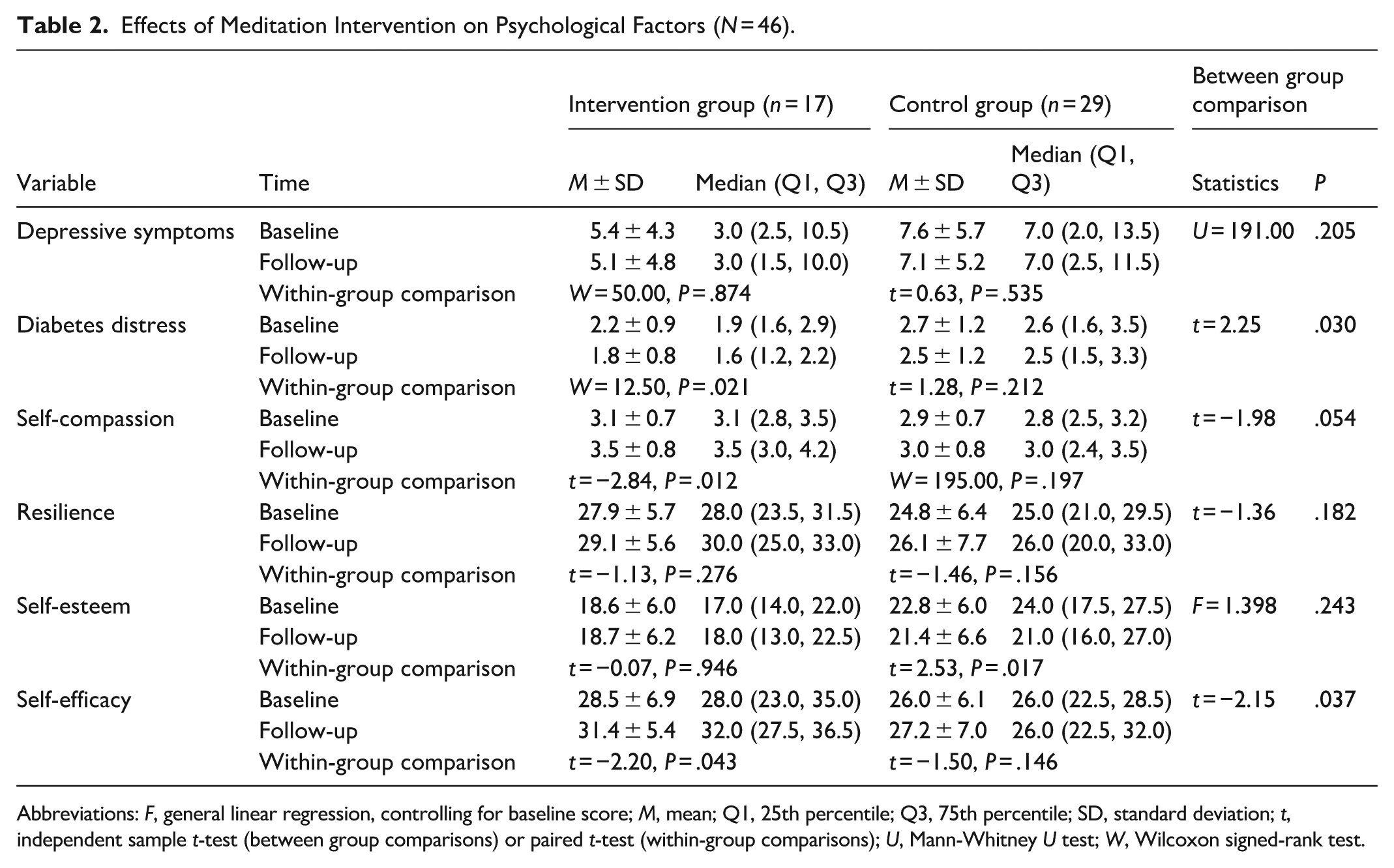
Abbreviations: F, general linear regression, controlling for baseline score; M, mean; Q1, 25th percentile; Q3, 75th percentile; SD, standard deviation; t, independent sample t-test (between group comparisons) or paired t-test (within-group comparisons); U, Mann-Whitney U test; W, Wilcoxon signed-rank test.
In within-group comparisons, the intervention group showed significant intervention effects in diabetes distress from baseline to follow-up (median: 1.9 vs 1.6, P = .021), self-compassion (mean: 3.1 vs 3.5, P = .012), and self-efficacy (mean: 28.5 vs 31.4, P = .043). The control group did not show any significant improvements in these variables. In contrast, the control group showed significant reduction in self-esteem from baseline to follow-up (mean: 22.8 vs 21.4, P = .017).
Discussion
The findings of this study suggest that a brief, asynchronous virtual compassionate meditation intervention may have beneficial effects on both negative and positive psychological factors. Delivered through prerecorded Zoom sessions, the intervention could reduce time, effort, and cost burdens for both participants and investigators. Participants could access the sessions at their convenience, allowing them to practice from home or any location that suited their schedule. This study makes an important contribution by demonstrating the feasibility of delivering a low-cost, flexible, and scalable psychological intervention for patients with diabetes. Unlike more resource-intensive in-person and lengthy interventions, the prerecorded virtual format may broaden accessibility while still improving key psychological outcomes. In this study, participants reported low levels of depressive symptoms. However, levels of diabetes distress were moderate to severe, and those of all the positive psychological factors were relatively low. These findings highlight the need for interventions aimed at improving both negative and positive psychological states in patients with diabetes. Therefore, this virtual compassionate meditation intervention could be a feasible and effective approach to enhancing psychological states in this population.
The recruitment method used in this study was feasible. Recruitment via ResearchMatch proceeded without any issues, recruiting the target sample in ~3 months. Thus, this recruitment method may be implemented to recruit patients with diabetes. The weekly intervention sessions were delivered to the intervention group via e-mail without any problems or complaints. However, intervention participation was not monitored in this study. Thus, the dosage could not be assessed. In future studies, it would be beneficial to monitor intervention participation to examine the impact on study findings. One challenge in this study was a high attrition rate at the follow-up data collection. We tried to contact participants in both groups by phone to reduce attrition rate, but only a small percentage of participants received phone calls. In future studies, establishment of regular contacts may be required to reduce attrition rates.
At follow-up, the intervention group showed less severe diabetes distress than both the control group at follow-up and its own baseline score. In this sample, the mean diabetes distress scores in the intervention and control groups (2.2 vs 2.7) at baseline and the mean score in the control group (2.5) at follow-up indicate that patients with diabetes had at least moderate levels of diabetes distress, considering the cut point for moderate and severe diabetes distress of ≥2. In the intervention group, the score at follow-up decreased to 1.8. These high levels of diabetes distress without interventions are consistent with the findings in prior studies (2.1-2.4).1,51 High levels of diabetes distress were associated with poor self-management and more diabetes complications.1,3,6 Therefore, a reduction in diabetes distress may contribute to improvements in self-management and reductions in diabetes complications. This intervention reduced the mean score of diabetes distress in the intervention group to below the cut point for at least moderate distress. In a prior study, diabetes distress was also reduced from 3.6 to 1.7 at the 8-week follow-up. 52 However, that study delivered a considerably more intensive mindfulness intervention with 8 daily in-person sessions and additional 8 weeks of maintenance practice sessions. 52 These findings suggest that either prerecorded or intensive in-person meditation sessions could be effective for reducing diabetes distress in patients with diabetes.
At follow-up, the intervention group showed higher levels of diabetes self-efficacy than both the control group and its own baseline score. In this sample, the level of diabetes self-efficacy at baseline was low (59.1 out of 100), similar to that in a prior study (64.3). 51 Lower levels of diabetes self-efficacy have been associated with poor self-management.5,10,53 These findings highlight the need to enhance diabetes self-efficacy in this population. At follow-up, the intervention group showed higher levels of diabetes self-efficacy than the control group (31.4 vs 27.2) and higher than its own baseline score (28.5). In a prior intensive meditation intervention (8 in-person sessions plus 8 technology-based maintenance sessions), diabetes self-efficacy also improved from 2.3 to 4.1 (total score range not reported). 52 Therefore, both brief prerecorded meditation sessions and intensive in-person sessions may be effective strategies to improve diabetes self-efficacy in patients with diabetes.
Self-compassion did not differ between the intervention and control groups at follow-up (3.5 vs 3.0, P = .054). However, self-compassion in the intervention group improved significantly (3.1-3.5), while the control group did not. In both groups, the levels of self-compassion were low (50.0 out of 100). Prior studies have linked self-compassion to better diabetes self-management.13,54 Thus, enhancing self-compassion is important. In a prior pre-post diabetes study, 8 weeks of mindfulness sessions (2.5 hours/session) plus 1 retreat session improved self-compassion from 3.2 to 3.4. 27 These findings suggest that even a relatively short, prerecorded meditation may enhance self-compassion.
In this study, the intervention did not improve self-esteem, depressive symptoms, or resilience. However, in the control group, self-esteem decreased significantly, whereas the intervention group maintained its baseline level. The levels of self-esteem in this study were very low (standardized mean score was 37.3 out of 100), similar to that in a prior study (35.7). 51 In both studies, the majority of the participants were white. Lower levels of self-esteem have been associated with poorer diet and exercise self-management in Mexican and Finnish patients with diabetes, respectively.14,55 Therefore, enhancing self-esteem remains an important goal. The effects of meditation on self-esteem in patients with diabetes have not been frequently examined. However, in a prior study of patients with breast cancer, 56 an 8-session mindfulness-based meditation and yoga (90 minutes/session) improved self-esteem at follow-up. These findings imply that meditation may help improve or at least protect against reductions in self-esteem in patients with diabetes. Depressive symptoms have improved in a systematic literature review 57 and in a study of 8 in-person meditation sessions (2.5 hours/session). 19 One potential reason for no improvement in depressive symptoms in this study may be the relatively low baseline levels in the intervention group (5.4 out of 24; cutoff for depressive symptoms = 7 or 10).41,58 By contrast, in the prior study that showed reductions in depressive symptoms in the intervention group, the mean baseline score was 14.0 out of 27. 19 Thus, future studies should test this meditation intervention in patients with diabetes who have more severe depressive symptoms. In this study, baseline resilience was relatively high (standardized score 70 out of 100) compared with other positive psychological factors, which may explain why resilience did not improve further. In a prior meditation study, resilience improved when the intervention group’s baseline mean was lower (63.6 out of 100). 23 That study required more intensive practice, including 30 minutes of formal meditation practice daily, informal practice, and listening to prerecorded sessions for 20 to 60 minutes twice daily for 8 weeks. These findings suggest that meditation can enhance resilience, but the current intervention may need further testing among people with diabetes who have lower baseline resilience.
A limitation of this study was the high attrition rate, with different rates between groups. This might have influenced the findings, although no differences were found in baseline sample characteristics or study outcomes. Interestingly, the control group was more likely to complete follow-up than the intervention group. Several control group participants contacted the research team to request intervention links. The likely reason for high attrition was the lack of direct contact with participants; most did not receive phone calls because this was not a required procedure. All participants were research volunteers from ResearchMatch, whose characteristics may differ from community patients with diabetes, which can limit the generalizability of the findings. However, participants were recruited from multiple states, which may enhance generalizability. The research team could not implement blinding due to the nature of the intervention, asynchronous virtual delivery, and online data collection and could not verify actual intervention participation, which may influence study findings and validity. Future studies should consider including at least 1 direct interaction with participants to reduce attrition and potentially strengthen intervention effects by building rapport with patients with diabetes with diverse settings and monitoring intervention participation.
Conclusions
The brief, virtual compassionate meditation intervention showed promising effects on psychological factors, including diabetes distress, diabetes self-efficacy, and self-compassion. Therefore, this intervention may be a feasible approach for patients with diabetes to improve their psychological states. The research process may need to be modified to include direct communication between the research team and the participants to reduce attrition rates and enhance the intervention effects. In addition, more studies are needed to test the intervention among patients with diabetes who have more severe depressive symptoms and lower levels of resilience, and with longer follow-up periods.
Footnotes
Ethical Considerations
This study was approved by Mercer University Institutional Review Board (H25-04007). This study was conducted according to the ethics principles of Helsinki declaration.
Consent to Participate
Written informed consent was obtained electronically from all participants after presenting the study purpose and procedure, potential benefits and risks, confidentiality, voluntary participation, and the right to withdraw without penalty.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Mercer University Seed Grant was given to Georgia Baptist College of Nursing (Principal Investigator: Dr Seongkum Heo) for this research.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, Seongkum Heo, upon reasonable request.