
Abstract
Background:
Transitions from home to long-term care facilities are critical and emotionally challenging for people living with dementia. Although person-centred care is widely advocated in dementia care, how staff experience and enact person-centred care throughout the transition process remains insufficiently synthesised.
Purpose:
This study explored staff experiences in implementing person-centred care during the transition of people living with dementia from home to long-term care facilities.
Methods:
Seven databases were searched, yielding 10 eligible studies. These studies were analysed using qualitative content analysis, guided by a person-centred care framework. The transition process was conceptualised into three phases: pre-transition, mid-transition, and post-transition.
Results:
Ten studies met the inclusion criteria. Four overarching themes with nine subthemes were identified, reflecting staff experiences in implementing person-centred care during the pre-transition, mid-transition, and post-transition phases, as well as barriers encountered across the transition process. The nine subthemes were (1) pre-transition professional competence; (2) pre-transition facilitating participation and shared decision-making; (3) post-transition professional competence; (4) post-transition interpersonal communication; (5) post-transition commitment to work; (6) post-transition supportive organisational systems; (7) post-transition understanding and respecting the values of people living with dementia; (8) post-transition facilitating participation; and (9) post-transition empathy.
Conclusions:
This meta-synthesis highlights that implementing person-centred care during transitions to long-term care is a dynamic and relational process. Both individual staff and organisations experienced attitudinal shifts towards person-centred care across the transition. Importantly, staff are required to implement person-centred care principles, particularly during the mid-transition phase when people living with dementia move into facilities.
Review Protocol Registration:
CRD42024622455.
Introduction
Dementia is a syndrome of cognitive decline accompanied by impairments in memory, language, and physical functioning, leading to increased dependence on others for care. 1 The number of people living with dementia is expected to increase from 57.4 million in 2019 to 152.8 million globally by 2050. 2 The physical and psychological stresses associated with caring for people living with dementia can force family caregivers to seek alternative care arrangements. 1 Transferring people living with dementia from their homes to long-term care facilities to receive care from formal nursing staff is common, with transfer rates of 48% in the United States, 3 54% in Australia, 4 and 70% in the UK. 5
Transitions from home to a long-term care facility are often seen as major life events for people living with dementia and their families. 6 Successful transitions enable people living with dementia to adapt to their new living environment and achieve a sense of well-being. 7 Nevertheless, people living with dementia who are in transition are often vulnerable and at risk of reduced well-being. 8 Transition is defined as the beginning of the period before admission to the adjustment period after actual admission. 6 The transition from home to a long-term care facility is a multistage process, that is, composed of the pre-transition decision-making phase, the mid-transition relocation phase, and the post-transition adjustment phase. 9 However, there are certain issues at each stage of the transition process, such as uncertainty among people living with dementia and their families about when and how to make the transition, 10 the distressing feelings of family members deciding to make the transition, 6 and the intense feelings of helplessness that the person may experience after the transition. 11 Although there has been an increased focus on people living with dementia in transition, previous studies have focussed on the factors that influence the decision of people living with dementia and their family caregivers to initiate the transition from their homes to long-term care facilities1,12 and the needs of these individuals. 6 Very few qualitative reviews have integrated the experiences and perspectives of facility care staff during the transition process.
Person-centred care is considered the gold standard of care for people living with dementia, 13 with key aspects including physical, spiritual, and emotional support; targeted communication; caregiver and family involvement; and access to care pathways. 14 The World Health Organization’s action plan on the public health response to dementia recommends implementing person-centred care in long-term care facilities to address current care gaps. 15 The role of nursing staff is critical to the successful implementation of person-centred care in long-term care settings, as they are both direct care providers and care managers. 16 However, it remains unclear how staff can provide person-centred care for people living with dementia who are in the transition phase. In this study, the person-centred care framework 17 was adopted to understand the content related to person-centred care from a holistic structural perspective. This framework consists of four constructs: prerequisites, the care setting, the person-centred process, and outcomes.
In this study, qualitative evidence on the experiences of nursing staff in implementing person-centred care during the transition of people living with dementia from home to long-term care facilities was synthesised. A qualitative meta-synthesis was conducted using a systematic literature search and qualitative content analysis, guided by the person-centred care framework proposed by McCormack and McCance. By integrating and interpreting findings from existing qualitative studies, this review achieved a comprehensive understanding of how person-centred care is experienced and enacted by nursing staff across different phases of the transition process. Additionally, this review provided evidence to inform practice and organisational support in long-term care settings.
Methods
Synthesis Methodology
Meta-synthesis, which is not the sum of the individual studies but rather an interpretive synthesis of the data that leads to new interpretations of the results in the study and greater effects on practice, was used in this study. 18
Protocol Registration and Reporting Guidelines
This meta-synthesis was registered in the International Prospective Register of Systematic Reviews (no: CRD42024622455) and was conducted on the basis of the guidelines provided by Enhancing Transparency in Reporting the Synthesis of Qualitative Research. 19
Search Methods
The search strategy for this paper was developed on the basis of the PICO principle, which consists of participants, the phenomenon of interest, context, and type of study. 20 In this review, the participants were nursing staff in long-term care facilities. The phenomenon of interest was the experiences of the nursing staff in implementing person-centred care for people living with dementia, the context was the stage of transition of people living with dementia from their home to a long-term care facility, and the types of studies were all types of qualitative studies and the qualitative component of mixed studies.
Given that the initial search revealed few qualitative studies explicitly examined the transition process of people living with dementia from a person-centred care perspective, the study extracted data relevant to the person-centred framework 17 using four keywords, namely “transitional care,” “long-term care facilities,” “dementia,” and “qualitative research.” A total of seven databases were searched: Web of Science, PubMed, MEDLINE, PsyclNFO, CINAHL, Embase, and Cochrane. Please refer to Supplementary Table S1 for the search strategy. As the implementation of person-centred care for people with dementia was first proposed in 1998, we searched the English language literature published from January 1998 to December 2024.21,22
Eligibility and Study Selection
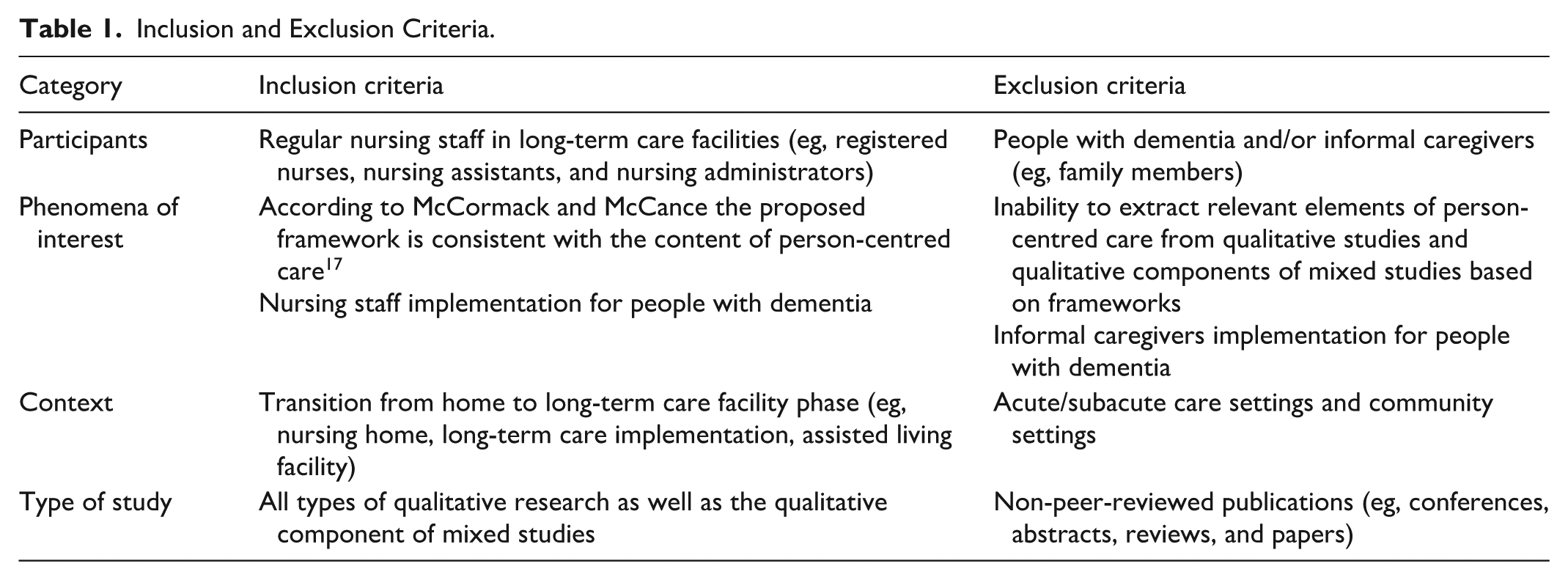
Relevant studies were selected or excluded on the basis of the inclusion and exclusion criteria. The results of the literature search were imported into EndNote 20 software (Clarivate, Philadelphia, PA, USA), and after eliminating duplicates, the titles and abstracts of the remaining studies were read and screened. The inclusion and exclusion criteria were shown in Table 1.
Inclusion and Exclusion Criteria.
Data Extraction and Analysis
Basic information from the articles (study title, year of publication, country, etc), purpose of the study, research methodology, and content related to the person-centred care framework 17 were extracted and coded into the NVivo14 software (Lumivero LLC, Denver, CO, USA) by two authors.
The data were analysed using qualitative content analysis, which includes both deductive and inductive analysis. 23 The extracted content was deductively based on the existing person-centred care framework. 17 Afterwards, the content was inductively categorised and further enriched with the existing framework. 24
The specific data were analysed as follows: During the initial reading process, two authors repeatedly read one third of the articles and, after discussion, developed an unconstrained categorisation matrix based on the person-centred care framework. 17 The first author then coded according to the four constructs within the framework (prerequisites, care setting, implementation process, and outcomes). After all the codes were reinterpreted and modified, the extracted codes were analysed inductively (ie, by grouping, categorising, and abstracting). All the authors actively participated in the entire coding and summarising process.
Quality Assessment
A quality appraisal was conducted to enhance transparency and to describe the methodological strengths and limitations of the included studies rather than to exclude studies on the basis of quality. The methodological quality of the included studies was investigated using the Critical Appraisal Skills Programme (CASP)-Qualitative Research Checklist, 25 which consists of nine items assessing the suitability of the study for qualitative research (eg, appropriateness of purpose and methodology) and whether the methods and outcomes of the qualitative research (eg, design, recruitment strategy, data collection, researcher-participant relationships, ethical issues, data analysis, and clear description of the findings) were adequately considered. After the full-text review, all ultimately selected studies were assessed by two independent authors. Furthermore, discussions were held during team meetings to resolve any disagreements. After this stage, no studies were excluded because of quality issues.
Researcher Reflexivity
To ensure research reliability, all the researchers were involved in screening, material selection, and data integration. Throughout the research, we held a weekly seminar where team members exchanged thoughts, determined the research direction, and discussed the data analysis conclusions. Additionally, through self-critical thinking, we examined views and preconceptions in dementia care to reduce the impact of personal biases on research outcomes.
Results
A total of 6717 records were retrieved. After the records were imported into EndNote 20, duplicate records were identified and removed, resulting in the exclusion of 1901 duplicates. After the titles and abstracts were screened, 40 records remained. After full-text review, nine studies met the inclusion criteria. An additional study was identified through reference list screening, resulting in a total of 10 studies included in the review (Figure 1). The methodological quality of the included studies, assessed using the CASP-Qualitative Research Checklist, is summarised in Supplementary Table S2. Overall, seven studies (70%) did not report on reflexivity regarding the researcher-participant relationship, and two studies (20%) did not clearly report their qualitative methodological approach.
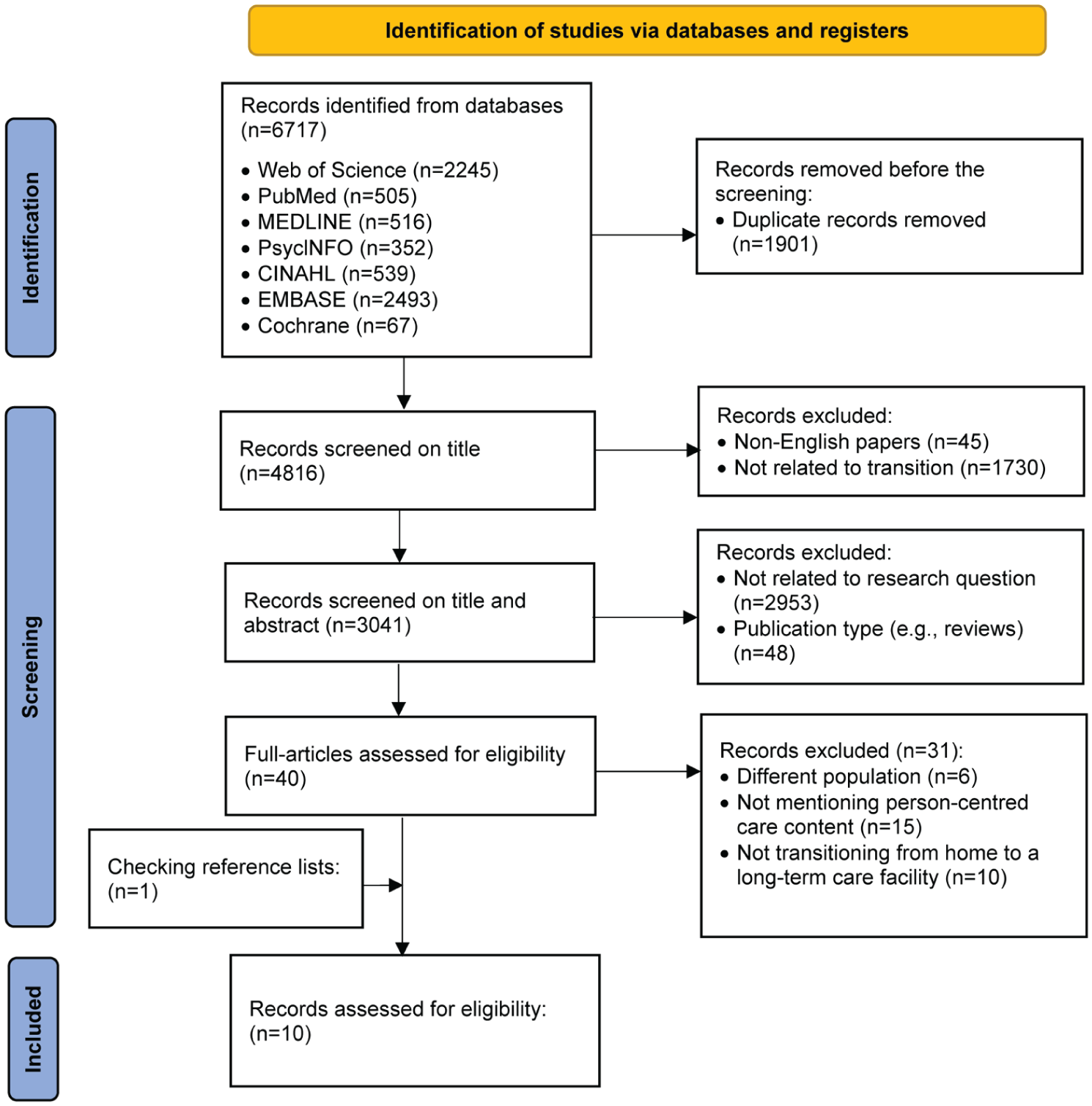
Search flow diagram.
The characteristics of the included studies are shown in Table 2. All the studies were published between 2009 and 2022, with the majority (n = 8) published in 2014 and beyond. The 10 studies had sample sizes ranging from 2 to 81 participants, for a total sample size of 310 participants. The participants in 3 of the studies were only long-term care facility staff. The participants in 2 studies each included people living with dementia and agency staff; family caregivers and agency staff; and family caregivers, agency staff, and non-long-term care agency staff (eg, general practitioners, community health nurses, and community psychiatric nurses). The participants in 1 study were people living with dementia, family caregivers, and agency staff. The long-term agency staff in each of the 10 studies comprised a variety of occupations and positions (eg, registered nurses, nurse aides, and agency administrators). Three studies included nursing homes as the transition sites, and the other studies included long-term residential care facilities as the transition sites. In terms of qualitative research methods, 7 studies were traditional qualitative studies, 1 was a case study, and the remaining 2 were mixed studies.
Characteristics of the Included Studies.
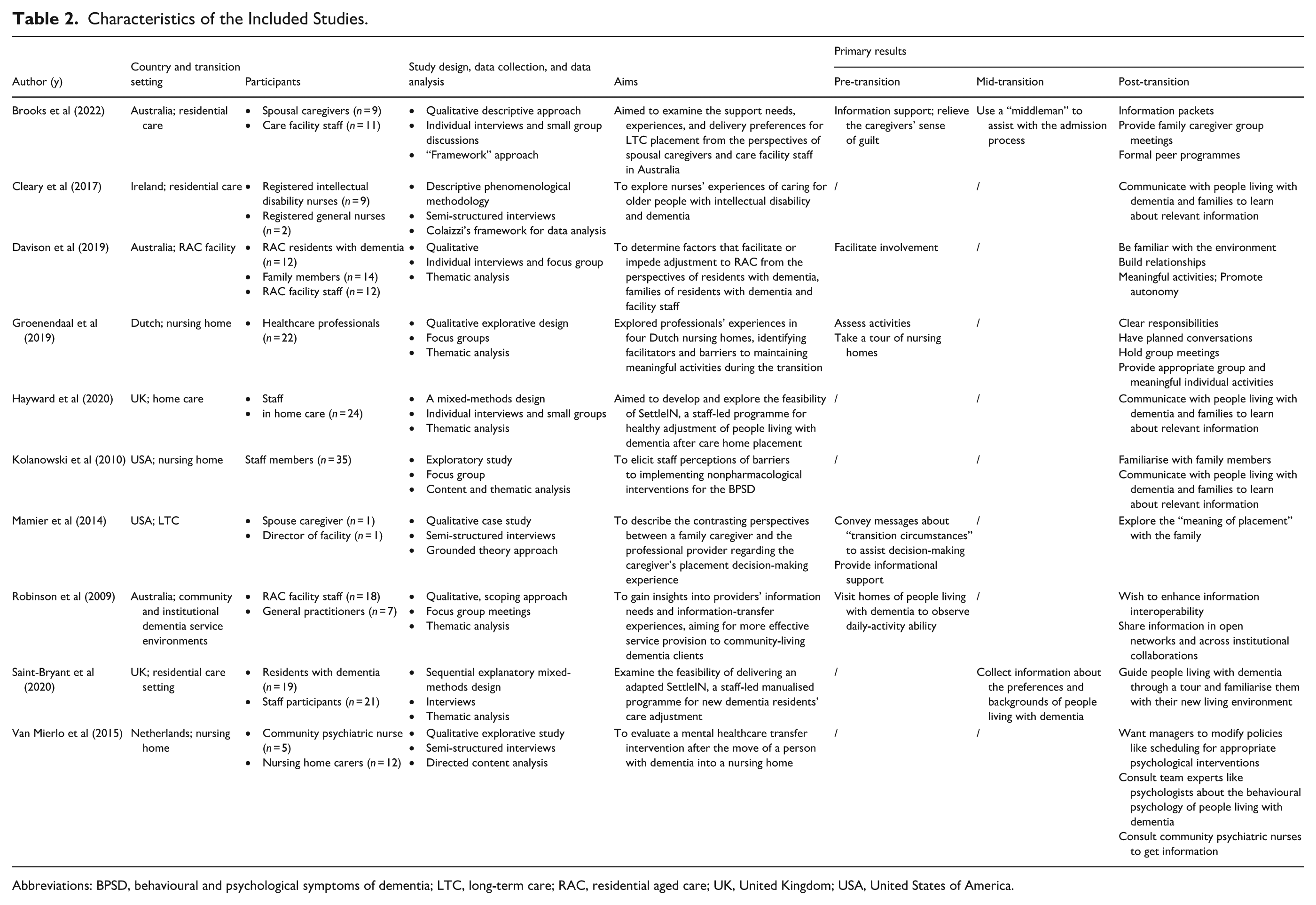
Abbreviations: BPSD, behavioural and psychological symptoms of dementia; LTC, long-term care; RAC, residential aged care; UK, United Kingdom; USA, United States of America.
To enhance clarity and analytical transparency, Table 2 summarises the key aims and principal findings of each included study according to the three phases of transition—pre-transition, mid-transition, and post-transition. Rather than reproducing original text, the table provides a concise synthesis of how each study addressed person-centred care practices within specific transitional contexts.
Guided by the person-centred framework 17 and a 3-phase transition model, 26 nine outcome domains were generated from staff experiences in implementing person-centred care and encountering barriers across the transition process. These outcomes are conceptually illustrated in Figure 2, while the primary and secondary analytical findings are further detailed in Table 3.
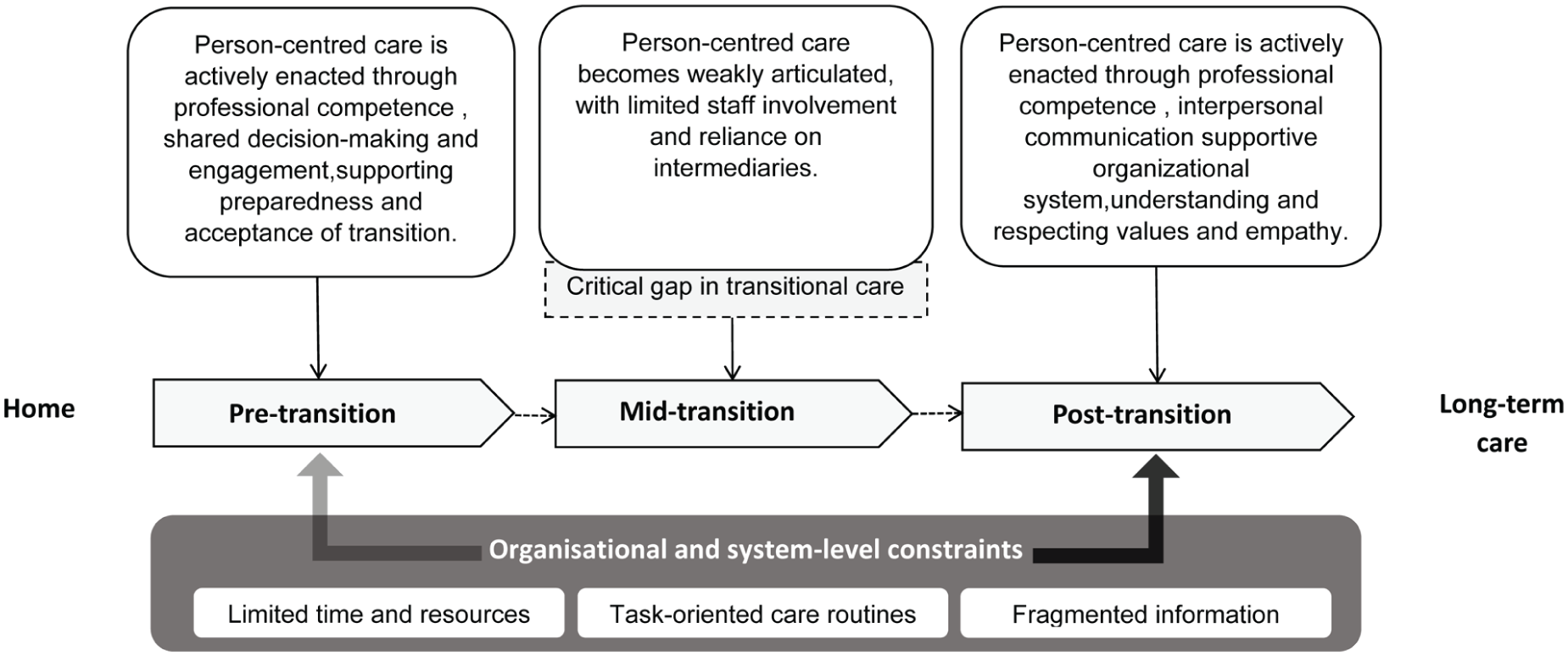
A person-centred care-informed transition model for people living with dementia.
Primary and Secondary Results.
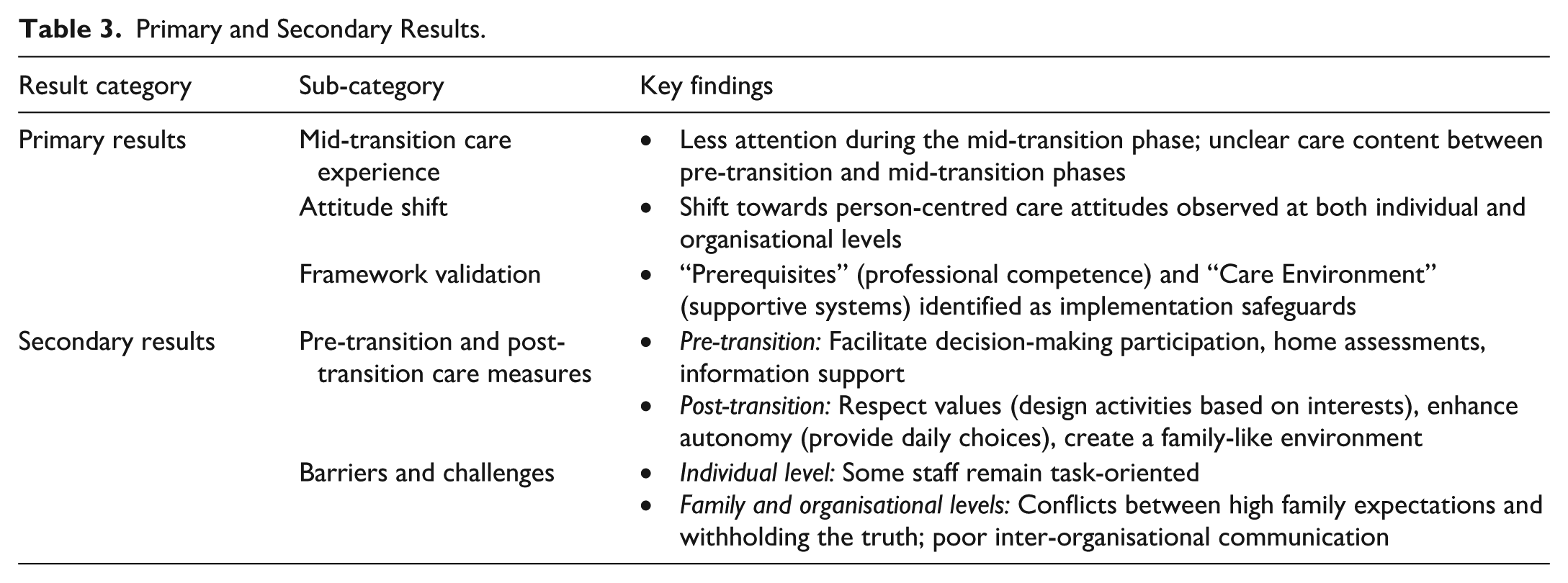
Ten qualitative studies were included in this meta-synthesis. Four themes were identified, corresponding to staff experiences during the pre-transition, mid-transition, and post-transition phases, as well as barriers encountered across the transition process. Across these themes, nine subthemes were identified, reflecting staff experiences in implementing person-centred care, including professional competence, participation and shared decision-making, interpersonal communication, commitment to work, supportive organisational systems, understanding and respecting individual values, facilitating participation, and empathy.
Importantly, the findings show that person-centred care practices were clearly articulated during the pre-transition and post-transition phases, whereas the mid-transition phase—from the decision to relocate to the day of admission—was consistently underdescribed, with few clearly defined staff roles or care practices reported across studies. In addition, staff reported uncertainty regarding how to provide person-centred care on the move-in day and during the initial adjustment period, highlighting a critical gap between decision-making and post-admission care.
Pre-transition
The pre-transition phase refers to the period that begins when moving into a long-term care facility is first discussed and ends with the decision to move into a long-term care facility.10,27 Two subthemes were identified during this phase: professional competence and promoting participation and shared decision-making.
Prerequisites—Professional Competence
During the pre-transition phase, staff members used their professional expertise to support people living with dementia and their family caregivers in relocation decision-making. Several studies, particularly those conducted in Australia, reported that nursing or care staff affiliated with long-term care services conducted home visits prior to admission. Staff reported that individuals were often more relaxed in their home environment, enabling more accurate observation of daily routines and functional abilities.28,29
Through these home-based assessments, staff evaluated daily activities; involved family caregivers in the assessment process; and identified meaningful activities aligned with individuals’ interests, habits, and routines.29,30 Such activities were perceived as contributing to residents’ well-being. 31 Staff also communicated transition-related information to family caregivers to support informed decision-making. 32
Person-Centred Processes—Promoting Participation and Shared Decision-Making
The involvement of people living with dementia in transition decision-making and planning may be associated with greater acceptance of the move. 33 Prior to the transition of people living with dementia to a long-term care facility, staff members took them on a tour of the nursing home to familiarise them with the new environment, 29 to help them understand the reasons for the move, and to encourage them to voice their own thoughts and opinions in the decision-making process. 34 With respect to the severity of dementia, the family caregiver’s decision is also critical when people living with dementia have severe cognitive impairment and are therefore unable to participate in decision-making. 35 Staff members recognised the caregiver’s guilt in deciding whether to transition and provided informational support while reassuring the family member32,36 to recognise himself or herself and participate in decision-making. 32
Mid-transition
The mid-transition phase begins when people living with dementia decide to transition and ends with admission to a long-term care facility.10,27 Compared with the pre-transition and post-transition phases, staff experiences related to person-centred care during this period were rarely described across the included studies. Only two types of staff involvement were mentioned in existing articles: staff advising family caregivers to use a “middleman,” such as a geriatric care placement counsellor, to help with procedures such as admissions, 36 and staff collecting information about the preferences and backgrounds of people living with dementia as they moved into the facility. 37
Across studies, staff narratives suggested that they were unclear on how person-centred care should be implemented during the period between relocation decision-making and actual admission. In particular, practices surrounding the move-in day and the early adjustment phase were rarely specified,10,38 indicating ambiguity in staff roles and responsibilities during this critical transition window. Although people living with dementia were frequently described as experiencing confusion, anxiety, or insecurity at the time of admission, staff accounts provided little detail on corresponding care strategies aimed at relational engagement, environmental orientation, or emotional support during this phase.10,38
Post-transition
The post-transition phase begins when people living with dementia move into a long-term care facility and continues until they and their caregivers accept and adapt to the new environment.10,27,35 Multiple subthemes were identified during this phase, including professional competence, interpersonal communication, commitment to work, supportive organisational systems, understanding and respecting values, facilitating participation, and empathy.
Prerequisites
Professional Competence
Staff members enhanced the ability of people living with dementia and their family caregivers to adapt to long-term care facilities through their own expertise. Staff members had clear responsibilities, and each person on the team was accountable for what they were responsible for. 29 This helped people living with dementia and caregivers understand dementia-related knowledge in the form of counselling, information packets, and workshops in the facility. 36 For family caregivers, staff members also provided family caregiver group meetings, 36 formal peer programmes, 36 and other ways to help caregivers adjust to life after transition.
Interpersonal Communication
In the transition process, staff improved their communication skills, built positive relationships with newly admitted people living with dementia, and recognised the importance of maintaining good communication with family caregivers. 34 They achieved this through planned conversations with family members 29 and by familiarising themselves with those who visited regularly, 39 thus gaining a deeper understanding of the people living with dementia.
Commitment to Work
Commitment to work reflects staff members’ dedication to people living with dementia, 17 and reflects their perspectives and recommendations for person-centred care. To help people living with dementia and family caregivers adapt to new environments, staff consistently implemented person-centred care 29 by focussing on them and providing appropriate group and meaningful individual activities.29,34 In this process, staff members made suggestions and expressed needs to provide better care. They wanted medical, medication, and service information 29 to assess people living with dementia more appropriately. At the organisational level, staff also developed new needs and wanted managers to modify policies, such as scheduling for appropriate psychological interventions. 40
Environment of Care—Supportive Organisational Systems
Supportive organisational systems feature an atmosphere of staff communication and collaboration. Multidisciplinary collaboration and regular team meetings enabled shared understanding and coordinated care. 29 Staff actively consulted team experts, such as psychologists, about the behavioural psychology of people living with dementia 40 and collaborated to advise them. This communication extended beyond the institution; staff members consulted community psychiatric nurses (CPNs), building a link with external institutions. Staff valued the information provided by CPNs, which helped them understand the needs of people living with dementia and adjust their care. 40 Staff also wished to enhance information interoperability, sharing it in open networks and across collaborating institutions. 28
Person-Centred Processes
Understanding and Respecting Values
Respecting the beliefs and values of people living with dementia reinforces the basic principles of person-centred care. 17 Staff members help people living with dementia adjust to institutionalised life values, strive to understand the values in their lives, 17 and put the information gained into daily practice.
At the beginning of the stay in the institution, staff communicated with people living with dementia and their families. In the process of communication, they learned about the previous occupations, interests, and other relevant information of people living with dementia.39,41,42 After becoming familiar with their personal experiences, they tried to create a warm home environment for them. 34 They encouraged family members to bring in their favourite personal belongings, photographs, and so forth, 34 thus increasing their comfort level. Based on the interests of people living with dementia, staff developed meaningful activities for them,29,34 helping them find meaning in the “little things.” 29 Staff also placed new residents at the same table as people living with dementia who had some similarities, 34 promoting the development of peer relationships and friendships among them.
Promotion of Participation
On the basis of understanding and respecting the values of people living with dementia, staff incorporated person-centred care principles into the promotion of participation, further recognising the uniqueness and value of people living with dementia. 17 On the first day of admission, staff guided them on a tour and familiarised them with their new living environment 37 to facilitate their integration into institutional life. During the adaptation process, staff realised the importance of granting autonomy to people living with dementia and viewed increased autonomy as a core component of person-centredness. 34 This view enhances the sense of ownership by providing people living with dementia with daily choices, such as engaging in activities and daily labour tasks. In this way, people living with dementia appreciated the contributions they made to the institution, and their sense of self-identity was strengthened. 34 The implementation of this framework helped facilitate their participation in the new living environment.
Empathy
Staff empathy not only facilitates better adjustment to institutionalised life for people living with dementia but also helps family caregivers navigate complex psychological changes. As people living with dementia gradually transition to a new life, their family caregivers also experience complex emotional changes. Staff members perceived and understood feelings of guilt and distress associated with the cognitive decline of people living with dementia, the perceived lack of competence of the caregiver, and a variety of other reasons for the family caregiver to decide to transition their relatives from home to a care facility. 35 By exploring the “meaning of placement” with the family, 32 listening to the caregiver, 36 providing reassurance and relief when needed,34,36 giving the caregiver up-to-date information about their loved one, 34 and encouraging and guiding caregivers to visit their loved ones regularly, 34 staff could help them adjust to life after transition.
Obstacles to Overcome
In terms of prerequisites, despite the staff’s efforts to implement person-centred care practices, some staff members were task-oriented34,36,37 and perceived that many fixed tasks related to the body of people living with dementia needed to be accomplished every day, leaving no time for other activities.34,37 This phenomenon was also reflected in care settings, where staff generally reported limited time and resources,37,40,42 which hindered their ability to provide meaningful activities and information mastery for people living with dementia. 40 In addition, some staff members felt that their division of labour was currently not clear and that there was ambiguity in the division of responsibilities. 34 In terms of staff communication, there was miscommunication and poor information sharing,28,40 with some staff failing to obtain valid information about people living with dementia prior to their admission to the programme,28,39 resulting in staff being unable to conduct appropriate assessments. There were also some contradictions in the implementation of person-centred care, which existed primarily between staff and family caregivers. Family caregivers may persuade people living with dementia that the transition was temporary prior to their admission, resulting in staff having to tell people living with dementia the truth, 34 which posed a challenge to the adjustment of people living with dementia to the new environment as well as the staff’s implementation of person-centred care. Moreover, in some instances, families had high expectations of the staff, which, in reality, were often difficult to fulfil. 36
Discussion
In this study, the experiences of nursing staff in implementing person-centred care during the transition of people living with dementia from home to long-term care facilities were synthesised within a person-centred care framework. The findings highlight person-centred care as a continuous process shaped by staff prerequisites, organisational contexts, and care processes throughout the transition continuum. By integrating staff experiences across pre-transition, mid-transition, and post-transition stages within a person-centred care framework, this study deepens the understanding of transitional dementia care.
Person-Centred Care Across the Transition Continuum
Consistent with the person-centred care framework, 17 this study demonstrates that staff prerequisites, particularly professional competence, communication skills, and commitment to work, are foundational to implementing person-centred practices in the transition of people living with dementia from home to a long-term care facility. During the pre-transition period, the staff used professional attributes such as competence and communication skills to offer information and support to people living with dementia and their family caregivers. This helped families decide on transition and reduced their psychological burden, which aligns with previous findings on the importance of early information provision.1,6
Importantly, staff’s efforts to involve people living with dementia in the decision-making process—such as facilitating facility visits and encouraging expression of preferences—reinforce earlier work emphasising participation as central to person-centred transitions. 10 These findings suggest that person-centred care during transition should be conceptualised not as a single intervention, but as an ongoing relational process.
Reconsidering the Mid-transition Phase as a Critical Gap
The results of the present study reveal that, during the mid-transition period, few care measures exist for people living with dementia in the period between their decision to move into a facility and the actual move. There are only recommendations for family caregivers to use a “middleman” and gather information of people living with dementia. In this phase, people living with dementia and their families are in the preparatory stage of the move and face difficulties. At the institutional level, they may be uncertain about the waiting time for admission 43 or be suddenly informed without enough preparation time.10,43 At the personal level, they may experience worry about decisions and confusion about their new life. 10 This implies that staff should focus on the needs of people living with dementia and caregivers during mid-transition. They can offer an information packet on moving to a nursing home, 44 help family caregivers plan for a sudden move, 32 continue pre-transition care practices such as visiting people living with dementia or giving them tours of the facility to familiarise them with the environment, and implement person-centred care on the admission day through a welcoming ceremony, staff and peer introductions, and similar approaches.
Previous research categorised the moving phase into pre-move preparation and the day of the move. 10 This study reveals ambiguity about care during the move-in day and the initial adaptation phase after transition. Previous studies did not clarify specific time points and corresponding care measures—such as building relationships, creating a home environment, and organising activities—even though people living with dementia are often confused and insecure on the move-in day.10,38 In the future, staff should focus on psychological changes of people living with dementia on the move-in day and develop appropriate admission plans. These plans should include introducing the institution’s daily routine, providing personalised spatial support, and building a relationship with people living with dementia to enhance their sense of belonging and homecoming and facilitate the establishment of a new identity.
Family Involvement as an Extension of Person-Centred Care
The findings further indicate that staff conceptualised person-centred care as encompassing not only people living with dementia but also their family caregivers. For family caregivers, they offered emotional and informational support to aid adjustment after the transition and valued communication to maintain trust.39,42 These findings indicate that the staff’s concept of person-centredness includes the family of people living with dementia and treating the whole family as the care unit.
However, tensions between staff and family caregivers—such as conflicting narratives about the permanence of placement—highlight the complexity of shared decision-making in the transition of people living with dementia from home to a long-term care facility. 34 This further highlights the need for staff to focus on the issues and needs of people living with dementia and caregivers before the move and to gather more information for person-centred care.
Barriers to Person-Centred Care Within the Framework
Despite staff’s commitment to person-centred values, multiple barriers constrained implementation. Owing to limited time and resources, some staff choose task-oriented work. There are also challenges in staff information communication, with poor information sharing between organisations. Task-oriented work patterns, limited time, and resource constraints reduced opportunities for relational care.16,45 Organisational barriers, including fragmented information systems and limited interorganisational communication, further hinder staff members’ ability to deliver individualised care.
These barriers reflect misalignments across the prerequisites, care environment, and care processes of the person-centred care framework. Further training and support should be provided to staff, and appropriate systems, support, and guidance need to be prioritised to optimise the care environment. 17
Limitations
There are several limitations to this study. Because non-English and unpublished studies were not included in the review, important articles written in other languages may have been overlooked or omitted, and the study may suffer from reporting bias. In addition, most of the studies were conducted in developed countries, and future studies should consider the global scope and conduct a broad search to explore more person-centred care experiences. Therefore, the generalisability of the findings may be limited to other developed countries. Finally, the person-centred care framework used in this paper was originally developed for the general population; further in-depth research is needed to adapt and validate it specifically for people living with dementia.
Implications
This review emphasises the importance of the care environment in the implementation of person-centred care, suggesting that future efforts should prioritise appropriate systemic support and guidance for staff in long-term care facilities. Currently, less attention is given to the mid-transition phase, indicating that staff should pay attention to the needs of people living with dementia from the time they decide to transition until the day they move to a long-term care facility. A more diverse range of supportive measures should be developed to help them navigate this critical period.
Conclusion
The findings of this review provide new insights into the experiences of nursing staff in long-term care facilities regarding the implementation of person-centred care for people with dementia during the transition from home to a care facility. However, these shifts in attitudes and practices are not consistently translated into care delivery across all transition stages.
In particular, the mid-transition phase—from the decision to relocate to the day of admission—emerges as a critical yet underdeveloped period. It is characterised by limited nursing interventions and uncertainty regarding care responsibilities on move-in day and during the early adjustment period.
To promote smoother and more person-centred transitions, care practices should be extended into the mid-transition phase. Organisations should strengthen communication, staff training, and interdisciplinary teamwork for person-centred support on the move-in day and during the initial adaptation period.
Supplemental Material
sj-pdf-1-wjn-10.1177_01939459261454861 – Supplemental material for Experiences of Staff in the Transition of People Living With Dementia From Home to Long-term Care Facilities Based on Person-Centred Care: A Meta-synthesis
Supplemental material, sj-pdf-1-wjn-10.1177_01939459261454861 for Experiences of Staff in the Transition of People Living With Dementia From Home to Long-term Care Facilities Based on Person-Centred Care: A Meta-synthesis by Jiaxin Li, Wei Li, Shengze Zhi, Shuyan Fang, Mengyuan Li, Huizhen Zhang, Jianing Lang, Yifan Wu, Qiqing Zhong, Daiyao Li and Jiao Sun in Western Journal of Nursing Research
Footnotes
Acknowledgements
The authors thank AJE for the language of the document.
Ethical Considerations
This work was a literature review using previously published information, and ethical review was not required.
Author Contributions
Jiaxin Li: conceptualisation, methodology, writing—original draft, formal analysis, data curation, validation. Wei Li: visualisation, writing—review and editing. Shengze Zhi: writing—review and editing, validation. Shuyan Fang: data curation, writing—original draft. Mengyuan Li: methodology, validation. Yifan Wu: conceptualisation, writing—original draft. Qiqing Zhong: conceptualisation, validation. Huizhen Zhang: methodology, validation. Jianing Lang: formal analysis. Daiyao Li: formal analysis. Jiao Sun: supervision, writing—review and editing. All the authors reviewed the final draft, and were willing to take responsibility for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Department of Science and Technology of Jilin Province, grant number 20250601034RC and 2025 Jilin University Doctoral Research Innovation Capability Enhancement Program, grant number: 2025KC112.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.