
Abstract
Objective. To determine the level of sentinel lymph node sectioning necessary to accurately detect nodal micrometastasis.
Study Design. Cross-sectional.
Setting. Tertiary care university medical center.
Subjects and Methods. Fine sections of oral squamous cell carcinoma sentinel lymph nodes previously sectioned at 2-mm intervals in a prospective clinical trial were reexamined. The results yielded from prior hematoxylin and eosin and immunohistochemical staining were compared with results following exhaustive serial sectioning at 150-µm intervals using identical staining methods. These experimental findings were compared with pathologic results of immediate completion selective neck dissection, previously recorded prospectively.
Results. Reexamination of 35 sentinel nodes at 150-µm intervals has not revealed any missed micrometastatic disease at 2-mm intervals used initially. Both comparisons of 150-µm sectioning analysis to the original 2-mm section samples and to the neck dissection pathology reports demonstrate a 100% negative predictive value.
Conclusion. These data suggest that sentinel lymph node sectioning at 2-mm intervals for oral carcinoma using hematoxylin and eosin staining and then immunohistochemical analysis maximizes efficiency, accuracy, and expenditure for the detection of micrometastasis.
Keywords
The current standard of care for staging the clinically node-negative (N0) neck for mucosal head and neck squamous cell carcinoma is selective neck dissection. Routine evaluation of neck dissection specimens generally involves a longitudinal cross section of the lymph nodes and evaluation of a limited number of sections cut from the 2 sides. Extensive literature exists on the use of sentinel node biopsy as a means of both reducing the extent of neck surgery and more accurately staging the neck. The accuracy is gained by clearly identifying a smaller number of lymph nodes at risk and evaluating these nodes with more extensive sectioning. Several groups have recommended sectioning at 150-µm intervals. 1,2 However, the actual extent of the fine sectioning is controversial, and there are significant implications in terms of cost. A recently completed multi-institutional cooperative group trial indicated that the negative predictive value of sentinel node biopsy in a group of surgeons of mixed experience levels was 96%. 3 This trial involved sectioning sentinel lymph nodes at 2- to 3-mm intervals with immunohistochemical evaluation of the sentinel node. In addition, traditional formal lymphadenectomy may miss a lymph node at risk for harboring micrometastases, as illustrated in Figure 1 , due to unexpected drainage patterns not anticipated by this standard lymphadenectomy. Sentinel node biopsy, while extensively used in Europe, is not considered standard in North America. One of the issues requiring clarification before sentinel node biopsy becomes a standardized procedure for oral cancer is the proper pathological management of the lymph nodes.
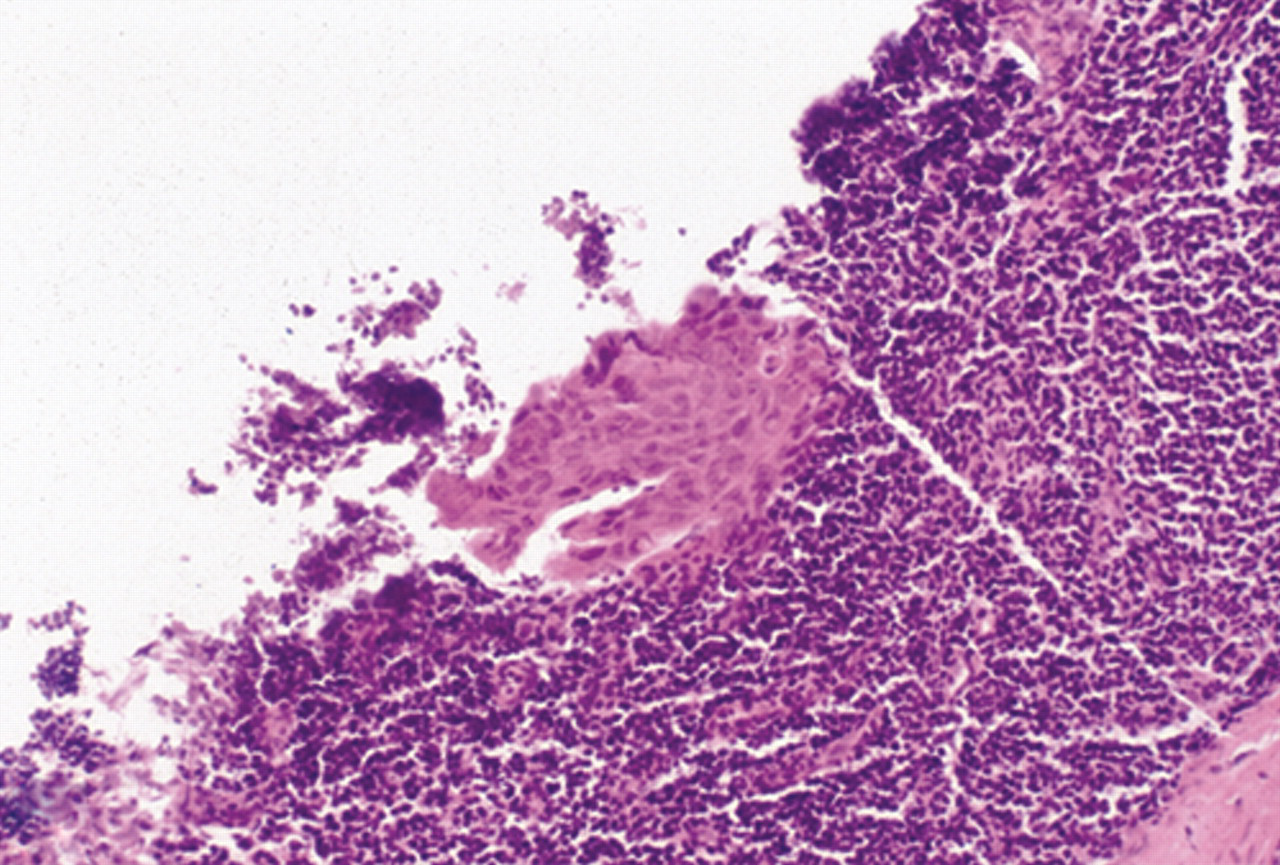
Sentinel lymph node demonstrating micrometastasis at high-power magnification.
Therefore, it is our aim to establish a standard sentinel lymph node sectioning protocol with appropriate hematoxylin and eosin (H&E) and immunohistochemical (IHC) staining. This will contribute to the efficiency and accuracy in the detection of micrometastasis in the sentinel lymph node for a clinically N0 oral squamous cell carcinoma.
Methods
Our study was approved by the University of Miami Human Subjects Research Office Institutional Review Board, and patients included in this study provided appropriate consent. We retrospectively reexamined sentinel lymph node tissue samples of oral squamous cell carcinoma obtained from patients treated between 1996 and 2004 that were previously sectioned at 2- to 3-mm intervals in our pathology department. Patients who had previously received finer sectioning on an internal protocol were naturally excluded, as no tissue was available. Patients who had undergone thicker 2-mm sections were obtained primarily from a group placed on a multi-institutional trial from our institution. These tissue blocks originally generated and processed with H&E and IHC staining were now reexamined following exhaustive serial sectioning and staining at 150-µm intervals. The experimental findings were then compared with the patient status after selective neck dissection, as documented in the medical record and prospectively collected data file, to determine any prognostic significance of the findings obtained through exhaustive sampling of the sentinel node.
Results
Ten patients with oral squamous cell carcinoma who previously underwent sentinel lymph node biopsy (SLNB) with sentinel lymph node (SLN) examination at 2-mm intervals were exhaustively fine sectioned at 150-µm intervals. These SLNs were reexamined using H&E and IHC staining at this finer section interval. A total of 35 SLNs were reexamined using this protocol. Table 1 provides the primary tumor sites, tumor stage, number of sentinel lymph nodes obtained, and sentinel lymph node positivity.
Characteristics of Primary Tumor and Sentinel Lymph Node Examination
Abbreviations: H&E, hematoxylin and eosin; SLN, sentinel lymph node.
No additional micrometastatic disease was discovered during the more extensive fine sectioning performed at 150-µm section intervals in these 10 patients’ 35 SLNs. The validity of SLNB in comparison with the gold standard cervical lymphadenectomy as documented in patient charting further demonstrates congruity of results with no missed metastatic disease in the SLNs.
Discussion
To date, there is no standard sentinel lymph node processing for examination of the SLN of clinically negative necks of patients with early T-stage oral mucosal squamous cell carcinoma. The Second International Conference on Sentinel Node Biopsy in Mucosal Head and Neck Cancer recommends step serial sectioning of the entire SLN at 150-µm intervals. 1 However, other authors use sectioning of the sentinel lymph node at 2- to 3-mm intervals. 4,5 The significant difference in labor involved led us to transition away from finer sectioning at our institution. Our retrospective reexamination of SLNs obtained to evaluate the clinically negative neck for early T-stage oral squamous cell carcinoma suggests that finer sectioning of the SLN at 150-µm intervals would improve the diagnosis of micrometastatic disease infrequently in comparison to SLN sectioning at 2-mm intervals, and the significant additional cost needs to be carefully considered. These results suggest that exhaustive fine sectioning of the SLN at 150-µm sections may not actually contribute to a change in clinical decision making; that is, with no change in SLN status based on finer sectioning, the patient would still not be offered a therapeutic neck dissection and his or her regional disease control would remain the same as if 150-µm SLN sections were employed.
A limitation of this study is the number of patient specimens that were reprocessed. An extensive amount of time and resources is necessary to exhaustively fine section the SLN, stain the sections with H&E and anticytokeratin as per protocol examination of these SLNs, and then subsequently examine all new slides obtained by this protocol. For example, sectioning at 2-mm intervals would generate 3 longitudinal slices from a typical 6-mm-wide SLN, as demonstrated in Figure 2 . These 3 slices are each placed in a separate block, and 4 representative sections are typically taken from each block for H&E and IHC staining. Thus, 3 blocks and 12 slides are generated for each lymph node. If there are 3 sentinel nodes, which is common in the head and neck region, 9 blocks and 36 slides are generated. In contrast, processing of the same 3 SLNs exhaustively at 150-µm intervals ultimately yields 120 slides for staining and evaluation. 6 A protocol of 150-µm intervals can thus become quite time-consuming and labor intensive with an associated increased cost. Significantly increased detection of micrometastasis would indeed justify this increased effort and expenditure.
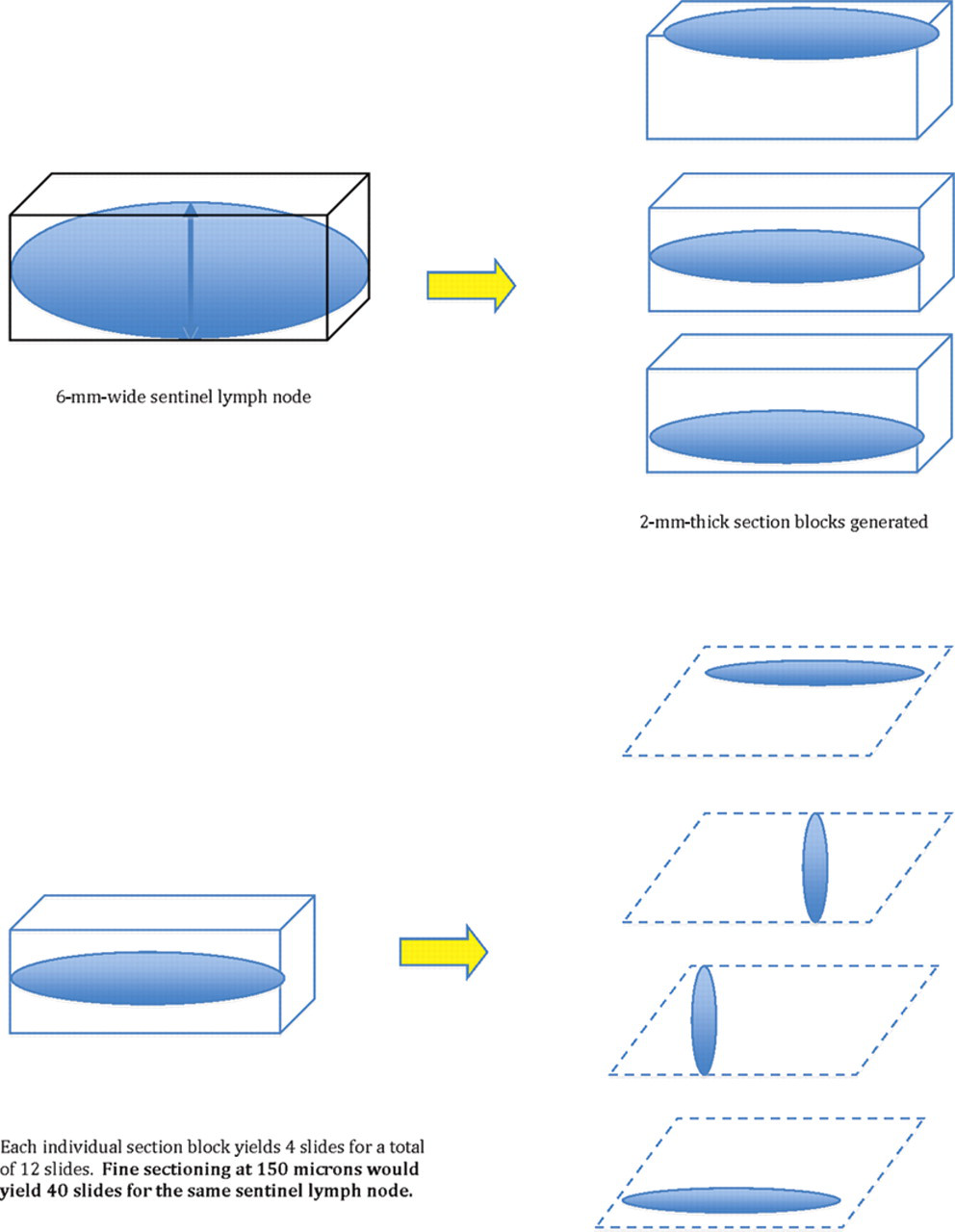
Method of exhaustive fine step sectioning of a sentinel lymph node.
Another limitation of our study is that none of the previously reported false-negative (FN) SLNs were reexamined here. The SLNs previously diagnosed as FN in comparison to the gold standard cervical lymphadenectomy specimen are of particular interest. Should exhaustive fine sectioning and reexamination of those FN SLNs reveal the initially missed micrometastatic disease, the FN rate of SLNB would decrease. This would suggest that the 150-µm sectioning interval would prove useful in the diagnosis of micrometastatic disease. Of note, no statistically significant data would be gleaned, however, because the FN rate is generally very low. At our institution, there were no available FNs processed at 2-mm intervals, as none had occurred since this protocol was instituted. In fact, a significant number of FNs would need to be examined to achieve statistically significant results. A study designed to demonstrate that fine sectioning of an SLN reduces the FN rate would require approximately 100 cases with gold standard neck dissection proven metastasis. Specifically, if there were a 30% rate of occult nodal disease among patients in our study with a 10% SLNB FN rate shown by standard lymphadenectomy, 302 patients are required, of whom 91 are SLNB and standard neck dissection for validation positive. This study design is based on 90% power and 5% significance with a hypothesis that fine sectioning at 150-µm intervals improves the diagnostic capability of micrometastasis in an SLNB (McNemer’s test of proportions for paired data).
It should be noted that in our original pathology reports as well as in the current work, both isolated tumor cells (ITCs) and micrometastases were interpreted as positives; floating intraluminal tumor cells that were not within tissue were not. The incidence of micrometastases and ITCs in oral SLNB has only recently been defined, and pathology reports did not routinely distinguish these 2 pathologic entities in the past. Some investigators based their reports and recommendations on micrometastasis defined using an upper size limit of 3 mm but no specification of the lower size limit. This lack of a formal definition makes evaluation of the incidence and clinical implications difficult to determine from these prior articles. 7 Currently, micrometastasis is defined by the American Joint Committee on Cancer as a metastatic deposit greater than 0.2 mm in diameter but not greater than 2 mm in greatest diameter. Isolated tumor cells are defined as metastatic deposits that are 0.2 mm in diameter or smaller. The incidence of ITCs is quite low, which contributes to the difficulty in determining their true prognostic significance. A recent investigation was published reexamining 86 SLNs and comparing the histopathologic examination to previously performed neck dissection specimens to assess how adoption of the definition of 2 mm as the upper size limit for micrometastasis would affect tumor staging and compare to the formal neck dissection histopathologic diagnosis of micrometastasis and ITCs. The authors identified 5 patients with ITCs within their SLN(s), 1 of whom had metastatic disease in the neck dissection specimen corresponding to an incidence of 20% regional metastatic disease in the presence of a SLN with an ITC. However, given this low number, it is not possible to make a definitive recommendation for performing neck dissection for all patients with the finding of an ITC in their SLNB specimen. 8 Additional investigation is warranted to truly define the prognosis of the ITC. Most surgeons at this point would err on the side of caution, interpret ITC as positive, and proceed with neck dissection.
Our data suggest, but do not prove, that a protocol for evaluation of the sentinel lymph node using 2-mm section intervals maximizes the efficiency, accuracy, and expenditure in the detection of cervical micrometastatic disease. Use of the finer 150-µm section interval did not improve the diagnosis of micrometastatic disease of squamous cell carcinoma in the clinically N0 neck in 35 lymph nodes from 10 patients. In the future, we would like to identify and recut a group of 6 FNs generated at other institutions from the American College of Surgeons Oncology Group multi-institutional trial, in which we participated, to determine if these FNs would have been avoided by finer sectioning, thereby improving the FN rate.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.
Poster presentation at the American Academy of Otolaryngology—Head and Neck Surgery annual meeting, October 6, 2009.