
Abstract
Objective. To determine whether mupirocin (440 µg/mL) and vancomycin otic drops (25 mg/mL) show evidence of ototoxicity in CBA/J mice immediately following a 7-day course of daily intratympanic (IT) injections and 1 month following treatment.
Study Design. Nonrandomized controlled trial.
Setting. Academic hospital laboratory.
Subjects. Twenty CBA/J mice.
Results. Mean auditory brainstem response (ABR) thresholds increased in all drug- and saline-treated ears immediately after 7 days of IT injections but returned to baseline for most stimulus frequencies by 30 days later. This finding appeared to be correlated with the presence and subsequent resolution of tympanic membrane (TM) perforations and granulation tissue at the injection sites. Mupirocin-treated ears showed no significant difference in ABR thresholds compared to saline-treated ears. No significant differences were noted between vancomycin- and saline-treated ears, but there was a significant interaction between testing day and stimulus frequency (P < .001). Further analysis revealed that ABR thresholds at 32 kHz remained significantly elevated in vancomycin-treated mice despite the resolution of TM perforations and granulation tissue 30 days after completion of IT injections (95% confidence interval, −13.5 to −5.5, P < .01).
Conclusion. Although IT application of mupirocin solution (440 µg/mL) caused no significant change in the ABR thresholds in a murine model, vancomycin solution (25 mg/mL) resulted in high-frequency threshold elevations in both the ear directly injected and the contralateral ear. Mupirocin solution may be beneficial in managing otitis externa and media caused by resistant pathogens. Further studies of ototopical vancomycin are needed to define parameters governing its safe use.
Ototopic antibiotic eardrops are frequently used in the management of external and middle ear infections and provide many benefits over systemic antibiotics. Otic drops allow a higher concentration of medication to reach the infection site, reducing antibiotic resistance and preventing the side effects of systemic treatments. 1 The traditional aminoglycoside and fluoroquinolone eardrops provide adequate coverage against the pathogens most commonly involved in ear infections, including Streptococcus pneumoniae, Haemophilus influenzae, Staphylococcus aureus, Pseudomonas aeruginosa, and Moraxella catarrhalis. 2,3
An increase in the number of infections caused by antibiotic-resistant pathogens, including methicillin-resistant S aureus (MRSA), has resulted in the need for alternative treatment modalities. 4-6 In a study of 577 patients with chronic serous otitis media, MRSA was the most frequently identified pathogen, whereas methicillin-susceptible S aureus (MSSA), P aeruginosa, and coagulase-negative staphylococci were less frequently isolated. 5 In addition, the prevalence of community-acquired MRSA in chronic otitis media has increased by more than 10% in an 8-year period. 6 MRSA otorrhea is often resistant to conventional aminoglycoside and fluoroquinolone ototopic drops, resulting in the increased use of intravenous medications, including vancomycin. 7,8 The use of intravenous medications for the management of ear disease has several disadvantages, including inconvenience, cost, adverse effects, and toxicity. 6 Development of treatment alternatives in the form of an ototopical medication would allow avoidance of intravenous medications and their associated side effects.
Both mupirocin and vancomycin have been successful in treating MRSA colonization and infections. However, neither has been used regularly as a topical antibiotic ear drop for the treatment of external or middle ear disease. Prior to investigating the efficacy of the topical use of these medications, the potential for ototoxicity must be considered. Any substance that enters the middle ear can access the inner ear by diffusion through the round window membrane and cause adverse effects to the cochlear and vestibular apparati. 9,10 To our knowledge, no other studies have evaluated the ototoxicity of topical mupirocin and vancomycin solutions using a murine model. The results of this study are translational to humans in that both of these preparations have the potential to treat ear disease caused by resistant pathogens.
Materials and Methods
This study was approved by the University of Connecticut Health Center’s Institutional Animal Care and Use Committee.
Subjects
Twenty CBA/J mice were purchased from The Jackson Laboratory (Bar Harbor, Maine). The mice were all female and 8 weeks old at study onset. The mice were subdivided into groups of 10 mupirocin and 10 vancomycin subjects. In each subgroup, 5 subjects were randomly chosen to receive an intratympanic (IT) antibiotic injection in the left ear, and 5 were chosen to receive an IT antibiotic injection in the right ear. The contralateral ear received IT injections of sterile isotonic sodium chloride solution as a control. In this way, each subject served as its own control to reduce animal numbers. The number of subjects (n = 10 per group) was chosen based on the estimate by Berndtson 11 of replicates needed to detect a 10% difference from control with a coefficient of variability of 5.33% for 95% power at P ≤ .05.
Surgical Procedure
Anesthesia
Auditory testing and IT injections were completed under general anesthesia using an inhalation technique. Using a self-contained closed-circuit setup, each subject was placed into an induction chamber where isoflurane at 4% with an oxygen flow of 2 L/min was administered. After induction, the subject was transferred to a snout mask for maintenance anesthesia with isoflurane delivered at 1.5% to 3%, with an oxygen flow of 2 L/min.
Auditory Testing
All recordings were conducted with the anesthetized animal placed in a soundproof chamber. Prior to recording sessions, subjects were examined for signs of middle ear infections, middle ear effusion, or external auditory canal debris. Auditory brainstem responses (ABRs) were measured using a real-time signal processing system (Tucker-Davis Technologies [TDT], System 3, Alachua, Florida). ABRs were recorded using a precalibrated open sound system by placing a loud speaker (TDT, model FF1) within 2 mm of the test ear while occluding the nontest external auditory canal. Three transcutaneous electrodes were placed in the mouse: an active electrode on the vertex, a reference electrode posterior to the right ear, and a grounding electrode in the animal’s flank. ABR thresholds were determined using pure-tone bursts of 4 milliseconds duration (rise/fall time of 2 milliseconds) delivered in 5-dB steps between 20 and 90 dB SPL (re: 20 µPa) at 8, 16, 24, and 32 kHz. Signal averaging was performed using 512 repetitions, presented at a rate of 21/s. ABRs were completed on days 1, 8, and 38.
Intratympanic Injections
After being anesthetized, the mouse was positioned under an otologic microscope. The external auditory canal and the tympanic membrane (TM) were examined for signs of infection and debris. After optimal visualization of the TM, a sterile 28-gauge needle connected via a polyethylene tube to a Hamilton syringe was passed through the inferior portion of the TM. Five to 10 µL of either mupirocin solution (n = 10 ears), vancomycin solution (n = 10 ears), or 0.9% saline (n = 20 ears) was injected to fill the middle ear space. The mupirocin solution (440 µg/mL) was formulated by dissolving 1 g of 2% mupirocin ointment in 50 mL of sterile isotonic saline. Vancomycin solution (25 mg/mL) was formulated using a 250-mg vial of vancomycin powder reconstituted with 10 mL of sterile isotonic saline. IT injections were performed daily for 7 consecutive days.
Statistical Analysis
The ABR thresholds were obtained at 3 time points and 4 frequencies. The mean ABR threshold at each stimulus frequency and time point was calculated. Three-way (drug, day of testing, and stimulus frequency) and 2-way (day of testing, stimulus frequency) repeated-measures analyses of variance (ANOVAs) were conducted. In addition, single-factor ANOVAs and Student’s t tests for pairwise comparisons were used to follow up significant interactions and main effects. Statistical significance was accepted at a value of P ≤ .05. All calculations were completed using Microsoft Office Excel 2010 and Systat version 13 software (Systat Software, Chicago, Illinois).
Results
Mupirocin
At study completion, for the mupirocin-treated mice, preinjection, day 8, and day 38 ABR thresholds were available in 8 of the 10 mice as 2 mice expired while under general anesthesia. As shown in
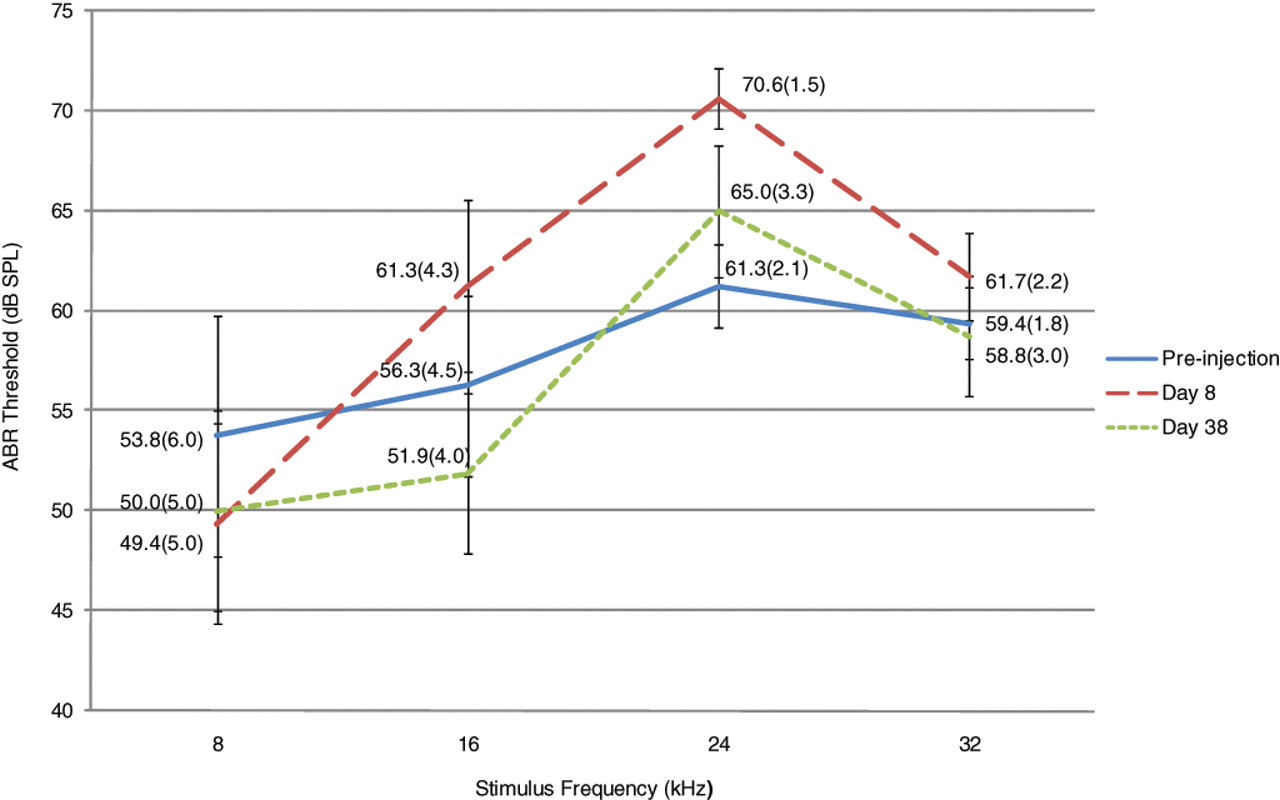
The mean auditory brainstem response (ABR) thresholds of the mupirocin-treated ears (n = 8) increased on day 8. By 1 month, the ABR thresholds returned to baseline values. For this plot and the remaining figures, error bars represent standard deviation (SD), and the mean ABR threshold value (±1 SD) is shown for each data point.

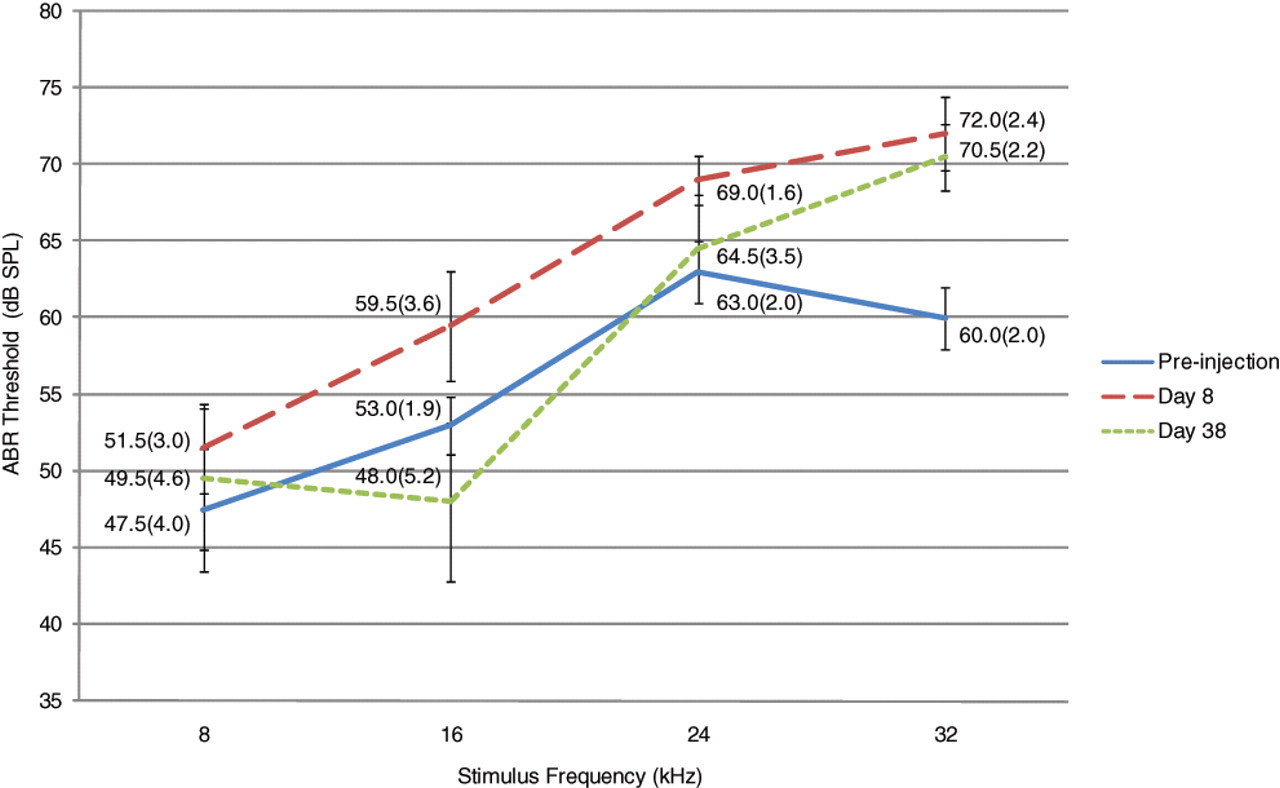
The mean auditory brainstem response (ABR) thresholds of the saline-treated ears (n = 8) in the mupirocin subjects increased on day 8 but returned to baseline values by 1 month.
A 3-way repeated-measures ANOVA showed no statistically significant 3-way interaction between drug, day of testing, and stimulus frequency. However, although the main effect of drug and day of testing was not significant, there was a main effect for stimulus frequency (F(3, 42) = 35.3, P < .001) and a significant interaction between stimulus frequency and day of testing (F(6, 84) = 3.7, P = .003). To follow up on the significant interaction between stimulus frequency and day of testing, separate 2-way repeated-measures ANOVAs were performed for the mupirocin- and saline-treated ears. This analysis showed a significant main effect for stimulus frequency in the mupirocin-treated (F(3, 84) = 11.5, P < .001) and saline-treated (F(3, 84) = 16.1, P < .001) ears but no significant main effect of day of testing. The interaction between these 2 variables also was not statistically significant. Because the difference between the mean ABR thresholds as a function of stimulus frequency was expected and there was no difference as a function of day of testing or drug, no further statistical analyses were carried out. These results suggest that although there was a trend toward increased ABR thresholds on day 8, this increase was temporary and not dependent on the drug injected.
Upon examination of the external and middle ears, there was no difference in the physical exams of the 2 groups on day 8. Both mupirocin- and saline-treated ears displayed TM perforations (62.5%; n = 5/8) and granulation tissue (37.5%; n = 3/8). On day 38, 25.0% (n = 2/8) of the mupirocin-treated ears and 12.5% (n = 1/8) of the saline-treated ears had thickened or sclerotic TMs. The remaining TMs were healthy appearing without any persistent perforations or granulation tissue.
Vancomycin
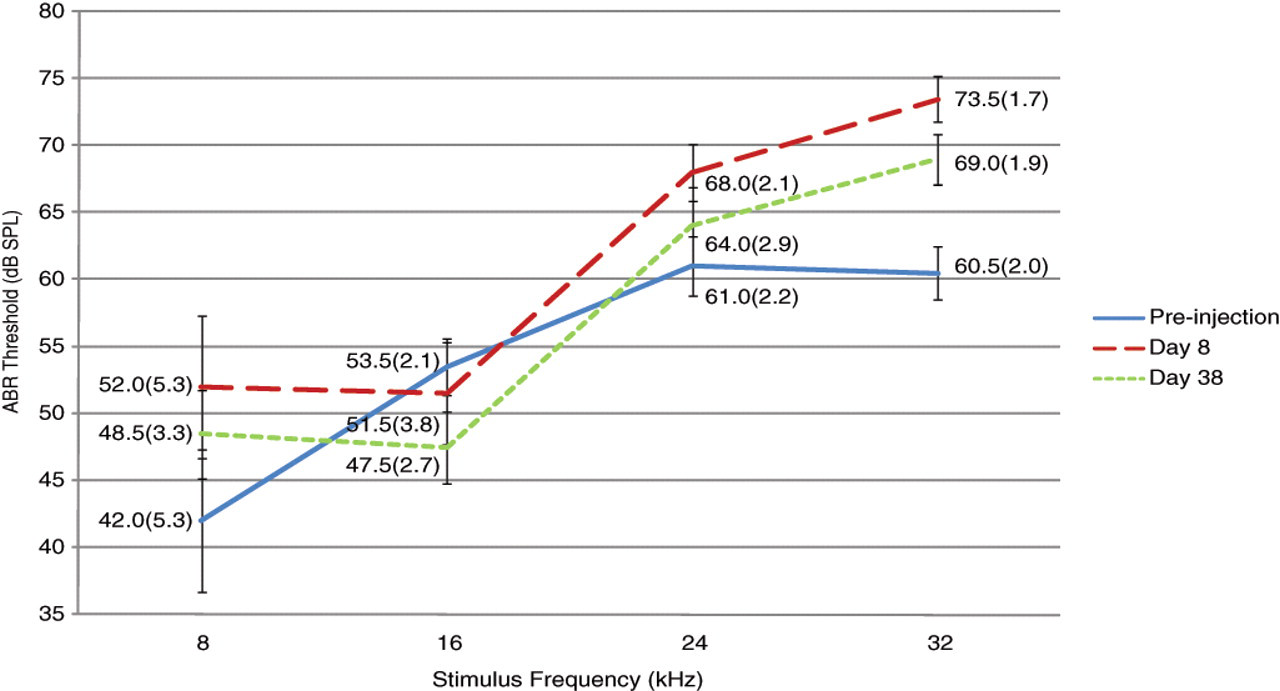
At study completion, for the vancomycin-treated mice, preinjection, day 8, and day 38 mean ABR thresholds were available for all 10 mice. As shown in
The mean auditory brainstem response (ABR) thresholds of the vancomycin-treated ears (n = 10) increased on day 8. By 1 month, the ABR thresholds returned to baseline values at all frequencies except 32 kHz.
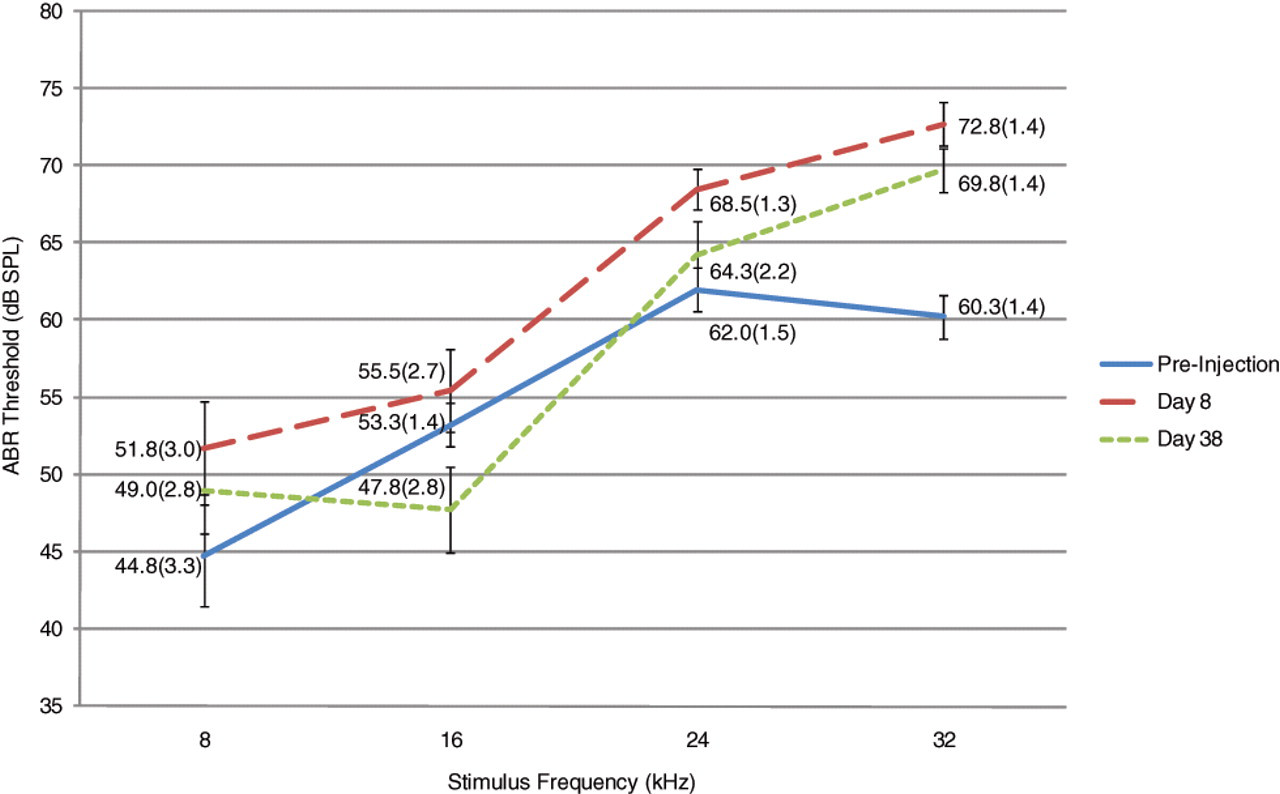
The mean auditory brainstem response (ABR) thresholds of the saline-treated ears (n = 10) in the vancomycin subjects increased on day 8 but, by 1 month, returned to baseline values except at 32 kHz.
A 3-way repeated-measures ANOVA showed no statistically significant 3-way interaction between drug, day of testing, and stimulus frequency. Although the main effect of drug was not significant, there was a main effect of day of testing (F(2, 36) = 13.7, P < .001) and a significant interaction between day of testing and stimulus frequency (F(6, 108) = 2.87, P = .01). The interaction between day of testing and stimulus frequency was further analyzed by combining the mean ABR thresholds for vancomycin- and saline-treated ears. As shown in
The mean auditory brainstem response (ABR) thresholds of all the vancomycin-treated subjects (n = 20) increased on day 8. By 1 month, the thresholds returned to pretest levels, except at 32 kHz, which stayed significantly elevated.
Upon examination of the external and middle ears, 100% (n = 10/10) of the vancomycin-treated ears had granulation tissue on day 8. In the saline-treated ears, 60.0% (n = 6/10) had TM perforations, and 40.0% had granulation tissue (n = 4/10) on day 8. By day 38, 30.0% (n = 3/10) of the vancomycin-treated ears had thickened or sclerotic TMs, whereas the remaining ears had normal-appearing TMs with resolution of all perforations and granulations.
Discussion
Although mupirocin and vancomycin have been effective in the management of MRSA colonization and infections, neither has been used regularly as an ototopical antibiotic for the treatment of otitis media or externa caused by resistant pathogens. In the present study, the objectives were to determine whether mupirocin or vancomycin solution results in ototoxicity immediately following a 7-day course of daily IT injections and 1 month following treatment using a mouse model.
Mupirocin, a topical antibiotic produced by Pseudomonas fluorescens, is effective in vitro against staphylococci, streptococci, and certain gram-negative bacteria, including H influenzae and Neisseria gonorrhoeae. 12 In addition, mupirocin is active against nearly all strains of coagulase-positive and coagulase-negative staphylococci tested, including multiply resistant isolates such as MRSA. 12,13 Although mupirocin is most commonly used to eradicate MRSA colonization of the nares, other otolaryngologic applications have been explored. As a solution, mupirocin irrigations are an effective alternative to intravenous and oral antibiotics in the management of chronic rhinosinusitis. 14-16 To our knowledge, there are no studies of a mupirocin solution used topically in the ear. However, as an ointment, mupirocin has been found to completely eradicate MRSA from the middle ear when applied through a TM perforation or tympanostomy tube and did not significantly change bone conduction thresholds. 17 The application as an ointment may be difficult for children to tolerate and requires administration by a medical professional. Transtympanic application of a solution through a TM perforation or tympanostomy tube would be easier and would not require office visits or hospital admission. However, a solution has increased potential to diffuse through the round window and potentially affect the inner ear.
In this study, we used a mupirocin concentration of 440 µg/mL, which is substantially greater than the mean inhibitory (0.12-1.0 µg/mL) and mean bactericidal (4-32 µg/mL) concentrations of mupirocin against S aureus. In addition, this concentration has equivalent in vitro efficacy as the standard mupirocin preparations against S aureus. 14,15 No significant changes were noted in the ABR thresholds after daily application of mupirocin solution (440 µg/mL) immediately following treatment and 1 month after application when compared to the pretreatment thresholds and to saline-treated ears. Immediately following a 7-day course of daily IT injections, an increase in the mean ABR threshold was noted in both the mupirocin- and saline-treated ears at most frequencies. This difference may be attributable to a temporary conductive hearing loss from repetitive trauma that resulted in TM perforations and granulation tissue in both groups immediately following treatment. One month later, the TMs returned to essentially pretest conditions, as did the ABR thresholds.
As previously mentioned, intravenous vancomycin is being used more frequently in the management of external and middle ear disease due to MRSA. Unfortunately, this is inconvenient, costly, and potentially toxic. The use of vancomycin as an ototopical drop would allow patients to avoid the negative effects of intravenous administration. Previous studies on the efficacy of topical vancomycin solution in treating MRSA otitis media and externa are promising. At a concentration of 25 mg/mL, vancomycin solution applied ototopically significantly reduced MRSA otorrhea in 94% of subjects tested and did not result in a statistically significant change in bone conduction thresholds. 7 Although information regarding the ototoxicity of topical vancomycin solution is limited, data on the ototoxicity of intravenous vancomycin have raised some concerns. In a clinical study of 89 patients receiving vancomycin intravenously, 12% of patients experienced high-frequency hearing loss. 18
In the present study, when using a concentration of vancomycin that has been shown in previous studies to reduce MRSA otorrhea (25 mg/mL), a significant increase in the ABR threshold at high frequencies compared to pretreatment thresholds was noted. In addition, there was no significant difference when comparing the ABR thresholds of the vancomycin-treated ears to contralateral saline-treated ears. Similar to the mupirocin subjects, an increase in the mean ABR thresholds on day 8 in both the vancomycin- and saline-treated ears was observed. Although the ABR thresholds in the mupirocin group and a majority of the vancomycin group returned to pretest levels by 1 month, the ABR threshold at 32 kHz remained significantly elevated for both the vancomycin-treated and their corresponding saline-treated ears. As noted above, the temporary elevation in the ABR threshold immediately following daily IT injections may be attributed to repetitive trauma, thus resulting in a temporary conductive hearing loss. The elevation of ABR thresholds at 32 kHz 1 month following completion of IT injections cannot be accounted for by conductive hearing loss since not all frequencies were affected and all middle ear changes had resolved, indicative of a sensorineural hearing loss. Because this sensorineural hearing loss was also present in saline-treated ears of the same animals, we suspect that vancomycin injected into one ear was absorbed systemically and resulted in ototoxic findings in the opposite ear, as well. Similarly, unilateral IT application of another ototoxic agent, gentamicin, was reported to lead to distribution of the drug bilaterally in the chinchilla inner ear, possibly through the cochlear aqueduct and cerebrospinal fluid. 19
The results of this study bring up many interesting implications. First, ototopic vancomycin produces high-frequency ototoxicity, consistent with previously reported findings in a clinical observational report on ototoxic effects of intravenous vancomycin. 18 However, previous studies examining the efficacy and ototoxicity of topical vancomycin solution through a TM perforation did not show significant hearing loss. 7 In that study, details about the results of audiometric testing and parameters such as frequencies tested and posttreatment interval to testing were not noted. One possible explanation for the divergent findings may be the absence of high- or ultra-high-frequency testing from that study’s assessments. Species differences may be an alternative explanation for the difference in findings and conclusions. For this to be true, mice would have to be more sensitive to ototoxic drugs than humans. However, previous results suggest that mice are considered to be highly resistant to ototoxic drugs than other rodents and humans. 20,21
Prior to use of either medication, further research should be considered. Although mupirocin did not result in ototoxicity in a mouse model, the efficacy as a solution and ototoxicity in humans needs to be further investigated. With regard to vancomycin, we plan to examine systemic absorption of IT application of vancomycin and determine whether lower concentrations of topical vancomycin maintain their antimicrobial efficacy without ototoxic side effects. Also, the otolaryngologic literature lacks significant data on factors that may contribute to the ototoxicity of both intravenous and IT vancomycin. These factors need to be further elucidated.
In conclusion, mupirocin solution caused no significant changes in the ABR thresholds when applied intratympanically in a mouse model, whereas vancomycin solution resulted in an increase in the ABR threshold at high frequencies. The temporary increased ABR threshold noted on day 8 may be attributed to conductive hearing loss resulting from TM perforation and middle ear inflammation that resolved 1 month after completion of IT injections. Although mupirocin solution may be beneficial in managing external and middle ear infections caused by resistant pathogens without producing any ototoxicity, further studies are needed to define parameters that govern safe application of ototopic vancomycin solution.
Author Contributions
Disclosures
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
This article was presented at the 2010 AAO-HNSF Annual Meeting & OTO EXPO; September 26-29, 2010; Boston, Massachusetts.