
Abstract
Objectives. To report improvement of obstructive sleep apnea syndrome (OSAS) and changes of high-sensitivity C-reactive protein (hs-CRP) concentrations after relocation pharyngoplasty (RP), a high variant of uvulopalatopharyngoplasty.
Study Design. Prospective comparative study.
Setting. Tertiary referral center.
Subjects and Methods. Thirty consecutive OSAS patients without a preexisting diagnosis of cardiovascular disease who underwent RP were assessed for body mass index (BMI), Epworth Sleepiness Scale (ESS), sleep apnea-hypopnea index (AHI), and serum levels of hs-CRP at baseline and 6 months postoperatively.
Results. Of the subjects, the mean values of age, BMI, ESS, AHI, and hs-CRP were 39.5 ± 7.0 years, 27.5 ± 4.5 kg/m2, 10.8 ± 4.2, 46.2 ± 22.9 events/hour, and 2.06 ± 1.78 mg/L, respectively. After 6 months postoperatively, RP reduced the ESS (Δ = −4.3 ± 4.5, P < .001) and AHI (Δ = −28.3 ± 21.1, P < .001) and levels of hs-CRP (Δ = −0.67 ± 1.36, P = .012) significantly, whereas BMI measurements were indifferent (Δ = −0.42 ± 1.28, P = .073). Moreover, the changes of AHI and hs-CRP were particularly remarkable in patients with very severe OSAS (AHI ≥60).
Conclusion. Although many OSAS patients remain in the mild-moderate category, equivalent improvements in excessive daytime sleepiness and reductions of hs-CRP concentrations indicate that reduction of AHI is not all that matters after RP.
Keywords
With longer life spans and increases in mean body weight among the general population in recent centuries, obstructive sleep apnea syndrome (OSAS) is steadily rising in prevalence worldwide. In Taiwan, the prevalence of recorded cases of sleep apnea was 3.4% in males older than 15 years. 1 Patients with OSAS are usually unaware of their sleep-disordered breathing but frequently suffer from excessive daytime sleepiness (EDS), which was contributed to by pronounced sleep fragmentation. Patients with OSAS not only experience a negative impact on their interpersonal relationships but also have higher risks of cerebrovascular and cardiovascular dieases. 2,3 Fortunately, the application of continuous positive airway pressure (CPAP) or upper airway surgery (mainly uvulopalatopharyngoplasty [UPPP]), which acts to splint or widen the airway to prevent its collapse, potentially reduces the morbidity and mortality of cardiovascular diseases in OSAS patients. 4-6
The pathogenesis underlying cardiovascular disorders in patients with OSAS is a multifactorial process. Metabolic dysregulation, sympathetic excitation, and endothelial dysfunction have been proposed to explain the possible mechanisms. 7 There is growing evidence that endothelial dysfunction resulting from inflammation processes leads to the development of various cardiovascular complications in OSAS. 8 Several inflammatory markers associated with cardiovascular risk have been demonstrated to be elevated in patients with OSAS, but their clinical values were very limited in the prediction of future cardiovascular events in recent epidemiologic studies. 9,10 High-sensitivity C-reactive protein (hs-CRP) was still the most popularly applied measurement of serum cardiovascular markers for monitoring cardiovascular risks in patients with heart disease or OSAS between 2007 and 2009. 7-20 We found that the sleep apnea–hypopnea index (AHI) was the independent predictor of the increase of hs-CRP levels after adjustment for conventional coronary heart disease (CHD) risk factors. 21 Our study highlighted the need of priority treatment in patients with severe OSAS and elevated hs-CRP.
In our English literature review, at least 3 studies published prior to 2006 demonstrated the potential benefits of airway surgery in decreasing the occurrence of cardiovascular disorders or reducing serum levels of hs-CRP. 22,23 We developed a modified UPPP surgery, which we called relocation pharyngoplasty (RP), for OSAS beginning in 2007. 24 It is unknown whether RP significantly restores daytime spirit and sleep parameters associated with decreased hs-CRP concentrations in patients with OSAS. The aims of this comparative study were (1) to compare changes of daytime spirit, sleep parameters, and hs-CRP levels after 6 months postoperatively and (2) to explore the clinical factors associated with our outcome of RP for OSAS.
Methods
Ethical Considerations
This prospective study was approved by the Institutional Review Board of Chang Gung Memorial Hospital and was conducted in compliance with the Health Insurance Portability and Accountability Act (1996) guidelines and regulations.
Patients
Patients ranging in age from 30 to 65 years who presented to the clinic for surgical evaluation of their newly diagnosed OSAS (AHI ≥5 events/hr) were consecutively investigated by compiling a complete medical history and physical examination between August 2008 and June 2009. Patients intolerant of nasal CPAP or unwilling to use this device and with retropalatal obstruction were further selected for RP.
Exclusion criteria included patients with (1) a previous diagnosis of cardiovascular disease (CHD, congestive heart failure, transient ischemia, stroke, and/or peripheral vascular disease), (2) a previous history of chronic liver disease or renal dysfunction, and (3) long-term use of anti-inflammatory drugs. 21
A total of 30 patients (29 men and 1 woman) who participated in the present study were evaluated for their EDS by a Mandarin Chinese version of the Epworth Sleepiness Scale (ESS), 25 absolute risk of CHD (ARCHD) based on the Framingham risk score system (1998), 26 and serum levels of hs-CRP, and they underwent RP for their OSAS. Details of the surgical procedure of RP are described elsewhere. 24
Evaluation of Clinical Parameters
Demographic and anthropometric characteristics were assessed at baseline and at 6 months postoperatively. The interview evaluated cigarette smoking status, diabetes mellitus, and cardiovascular events. Body weight and height were automatically measured and presented as body mass index (BMI), and tonsil size and tongue-palate position were manually scored according to Friedman’s classification. 27 In addition, patients were assigned a stage (I-IV) based on morphologic findings. 28 The patients measured their blood pressure with a standard sphygmomanometer on 3 different occasions, with the subject in supine position. A Mandarin Chinese version of the ESS evaluated EDS in 8 specific situations and generated a total score ranging from 0 (best) to 24 (worst) and was self-scored by the patients themselves. 25 Patients were categorized as having normal (ESS, 0-10), mild (ESS, 11-15), moderate (ESS, 16-20) or severe (ESS, 21-24) EDS and were placed in respective groups.
In-Laboratory Polysomnography
One to 2 months before this study and at least 6 months after RP, patients underwent a full-night sleep study to characterize their sleep and breathing patterns. Standard criteria were employed to evaluate patient breathing patterns during sleep. 29 The parameters used in this study were AHI, apnea index (AI), oxygen desaturation index (ODI), mean oxygen saturation, and least oxygen saturation. Apnea was defined as a drop in the peak thermal sensor excursion by at least 90% of baseline for at least 10 seconds. Hypopnea was defined as a decrease ≥30% in nasal pressure signal excursions for at least 10 seconds accompanied by desaturation of 4% or more from pre-event baseline or an arousal from sleep. The AHI was calculated as a sum of apneas and hypopneas. Patients were further categorized as having mild-moderate (AHI <30), severe (AHI, 30-59), or very severe (AHI ≥60) OSAS and placed in respective groups in the present study because there were more than one-third of the OSAS patients with AHI ≥60 at our sleep center. 21
Evaluation of hs-CRP and ARCHD
Individuals had fasting blood samples taken in the morning or at the termination of the follow-up sleep study between 7:00 and 7:30
The patients were assessed for the ARCHD by identifying the absolute risk of future CHD events in the next 10 years using a Framingham-based risk calculator 31 at baseline. This risk assessment originally applies to evaluation for primary prevention of CHD in subjects who do not have evidence of established vascular disease. The associated risk factors include sex, age, total cholesterol, high-density lipoprotein (HDL) cholesterol, systolic blood pressure, diastolic blood pressure, diabetes, and smoking.
Statistical Analysis
We used a logarithmic transformation of hs-CRP (log10 hs-CRP) for correlation and regression analyses because its distribution was positively skewed. Relationships between log10 hs-CRP and baseline sleep parameters and ARCHD were assessed through the use of the Pearson correlation coefficient for continuous variables. Univariate logistic regression analysis was tested. Data were compared for continuous variables using the Student t test or the Mann-Whitney nonparametric test when the frequency distribution was skewed. One-way analysis of variance was used to compare differences in AHI and hs-CRP changes among patients at different OSAS severity stages. Statistical analyses were performed using SPSS 16.0 for Windows (SPSS, Inc, an IBM Company, Chicago, Illinois). All statistical tests were 2 tailed. Continuous variables are presented as mean ± standard deviation. Final P values < .05 were considered statistically significant.
Results
Characteristics of the Study Population at Baseline and After a 6-Month Follow-up After Relocation Pharyngoplasty a
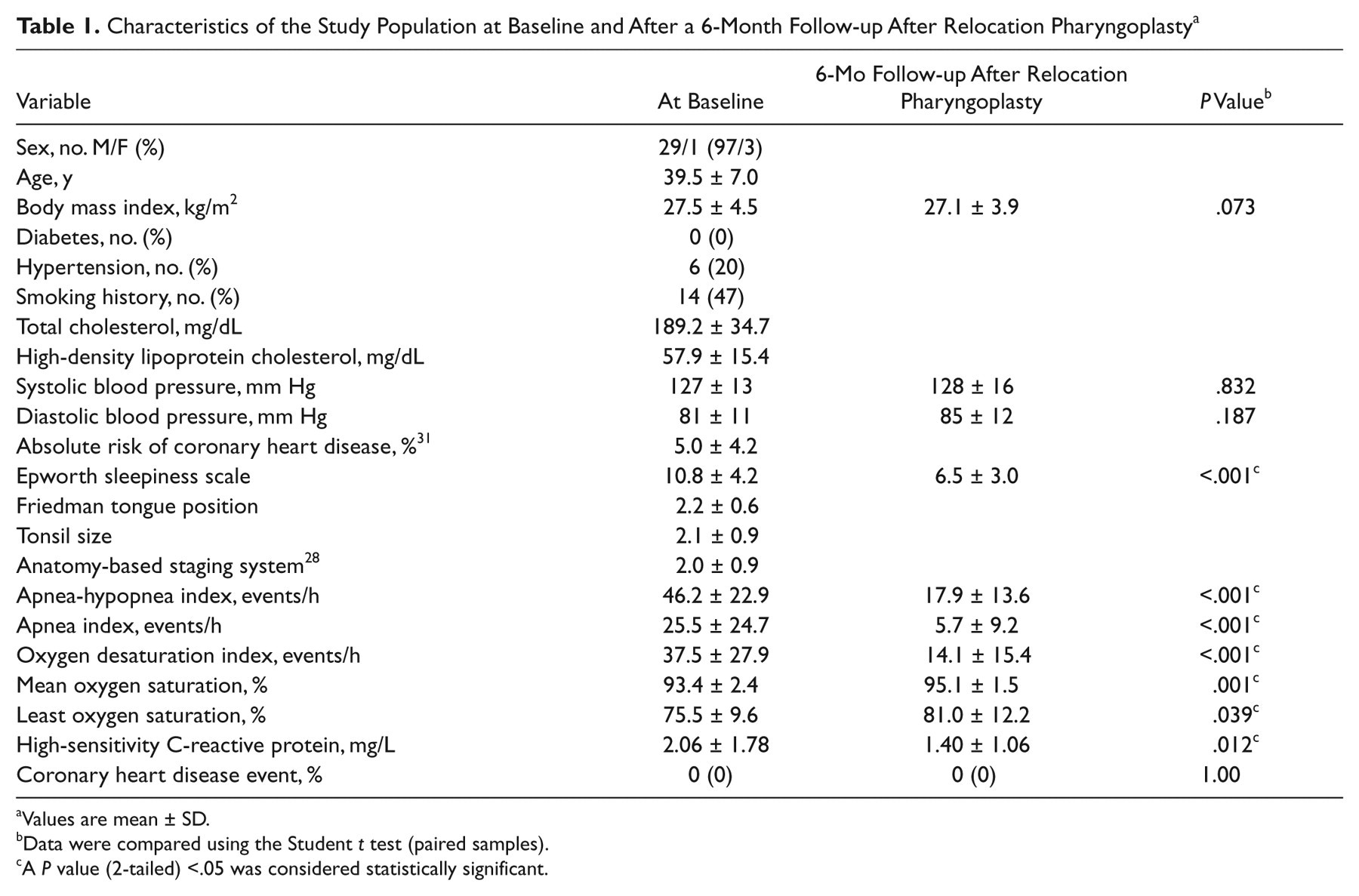
Values are mean ± SD.
Data were compared using the Student t test (paired samples).
A P value (2-tailed) <.05 was considered statistically significant.
BMI changed insignificantly from 27.5 ± 4.5 to 27.1 ± 3.9. Overall, the postoperative AHI decrease was −28.3 ± 21.1; the difference between before and after the operation was statistically significant (P < .001;
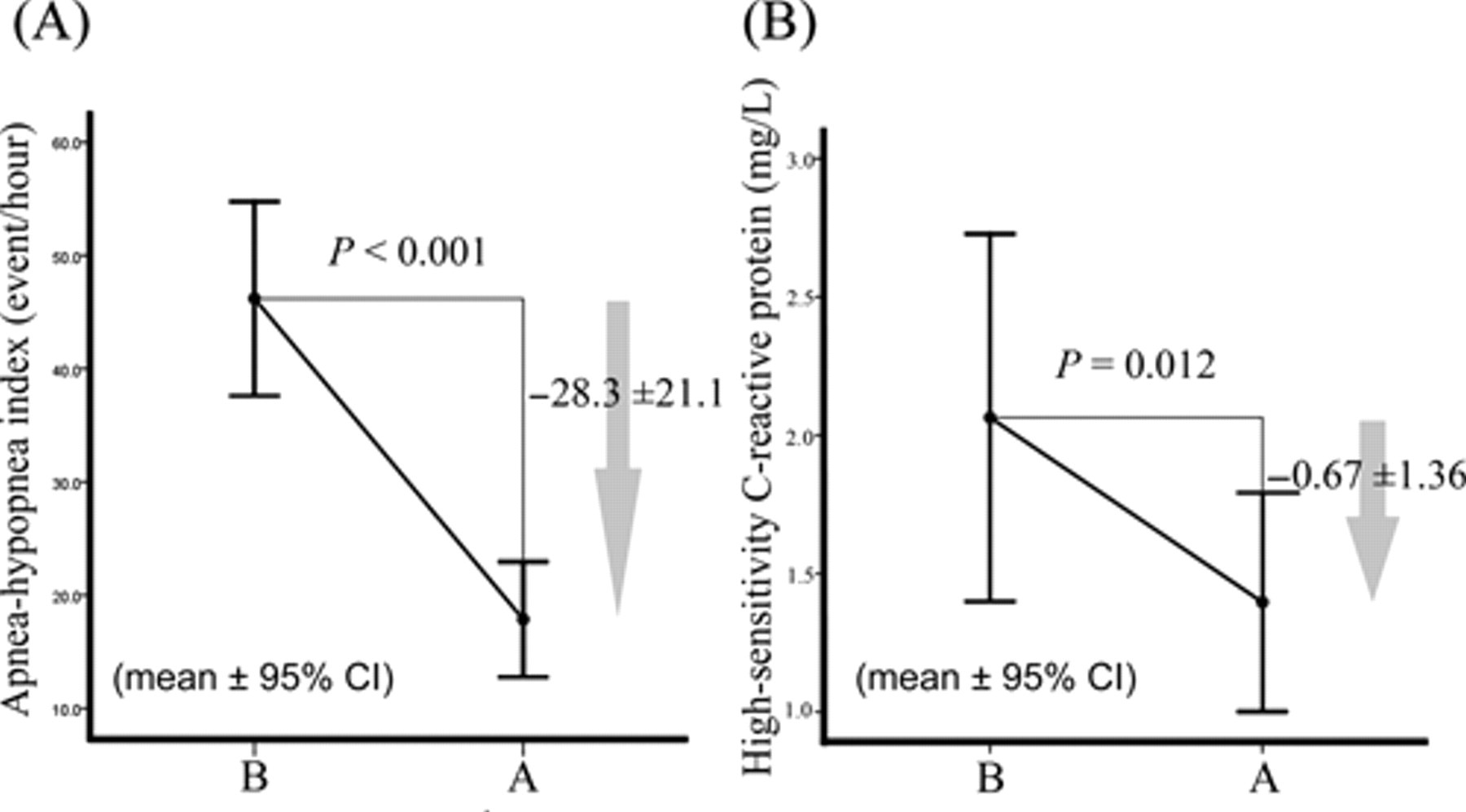
(A) The mean ± standard deviation (SD) of the apnea-hypopnea index (AHI; solid circle and bar) and change in values for each patient at baseline and 6 months after relocation pharyngoplasty. (B) The mean ± SD of high-sensitivity C-reactive protein (hs-CRP) (solid circle and bar) and change in values for each patient at baseline and 6 months after relocation pharyngoplasty. Relocation pharyngoplasty significantly reduced the AHI and serum levels of hs-CRP. CI indicates conference interval; B, baseline; A, after 6 months postoperatively.
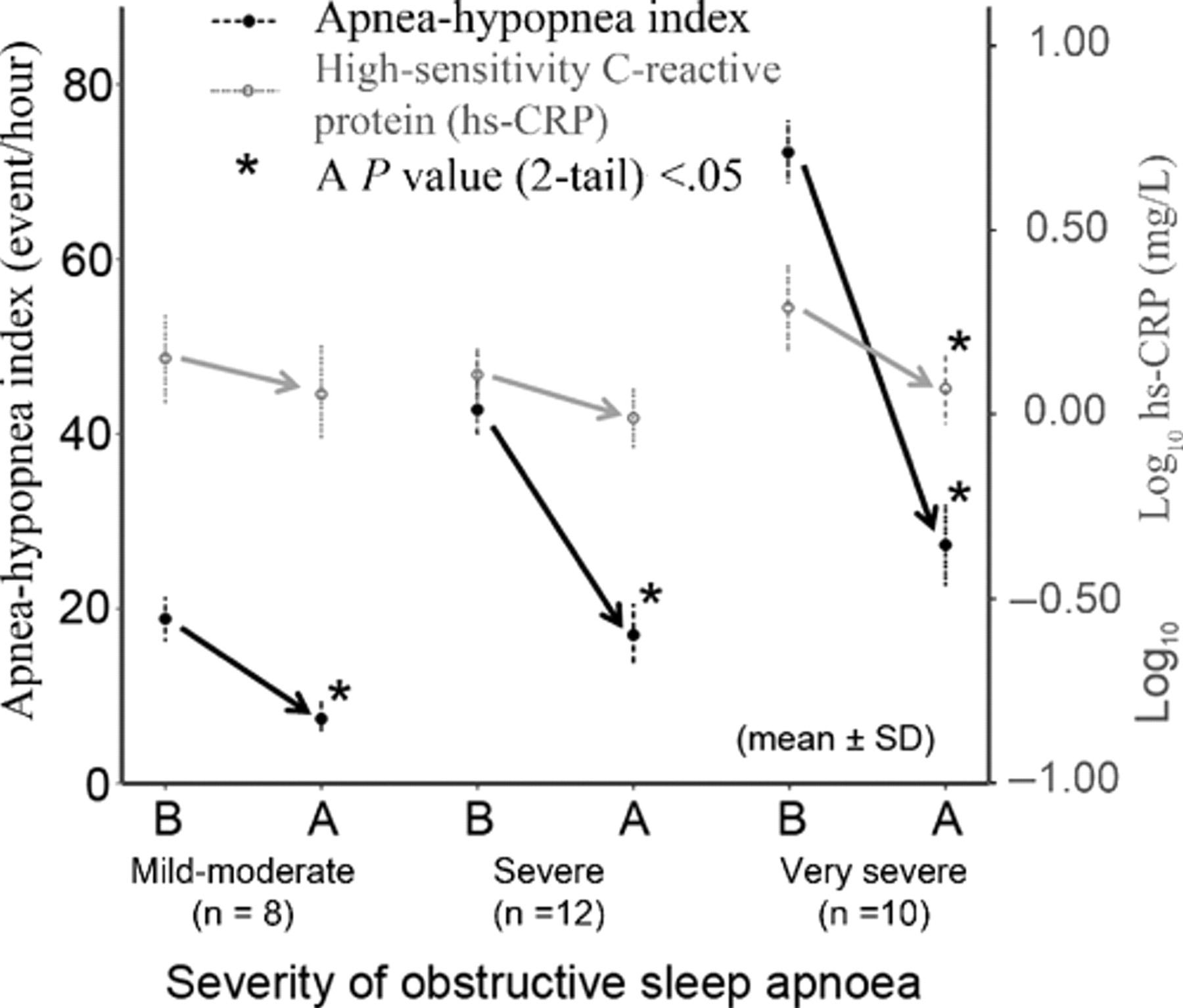
The mean ± SD of the apnea-hypopnea index (AHI; black solid circle and bar) and high-sensitivity C-reactive protein (hs-CRP; gray solid circle and bar) for each obstructive sleep apnea syndrome (OSAS) severity group at baseline (B) and after 6 months postoperatively (A). The AHI was reduced significantly by relocation pharyngoplasty in each OSAS severity group, but serum levels of hs-CRP decreased significantly only in the very severe OSAS group.
For further analyses, we added a “cured” group (AHI <5) according to the followed AHI test in addition to the other 3 OSAS severity groups. There were only 4 patients (13%) cured after RP in the present study. Moreover, treatment outcomes of RP on ESS, AHI, or hs-CRP were categorized as worsening (increasing at least 1 degree after operation), no change (remaining in the same degree postoperatively), or improving (decreasing at least 1 degree after operation). Accordingly, the improvement rates of ESS, AHI, and hs-CRP were 37%, 70%, and 40% after RP, respectively.
In addition, patients were classified in young (aged 30-39 years), middle (aged 40-49 years), or elderly (aged 50-59 years) age groups, whereas patients were triaged to normal (BMI <25 kg/m2), overweight (BMI 25-29 kg/m2), or obese (BMI ≥30 kg/m2) groups according to their baseline BMI measurement.
21
Univariate Analysis of the Treatment Outcomes of Relocation Pharyngoplasty on Apnea-Hypopnea Index and Serum Levels of High-Sensitivity C-Reactive Protein and Baseline Factors
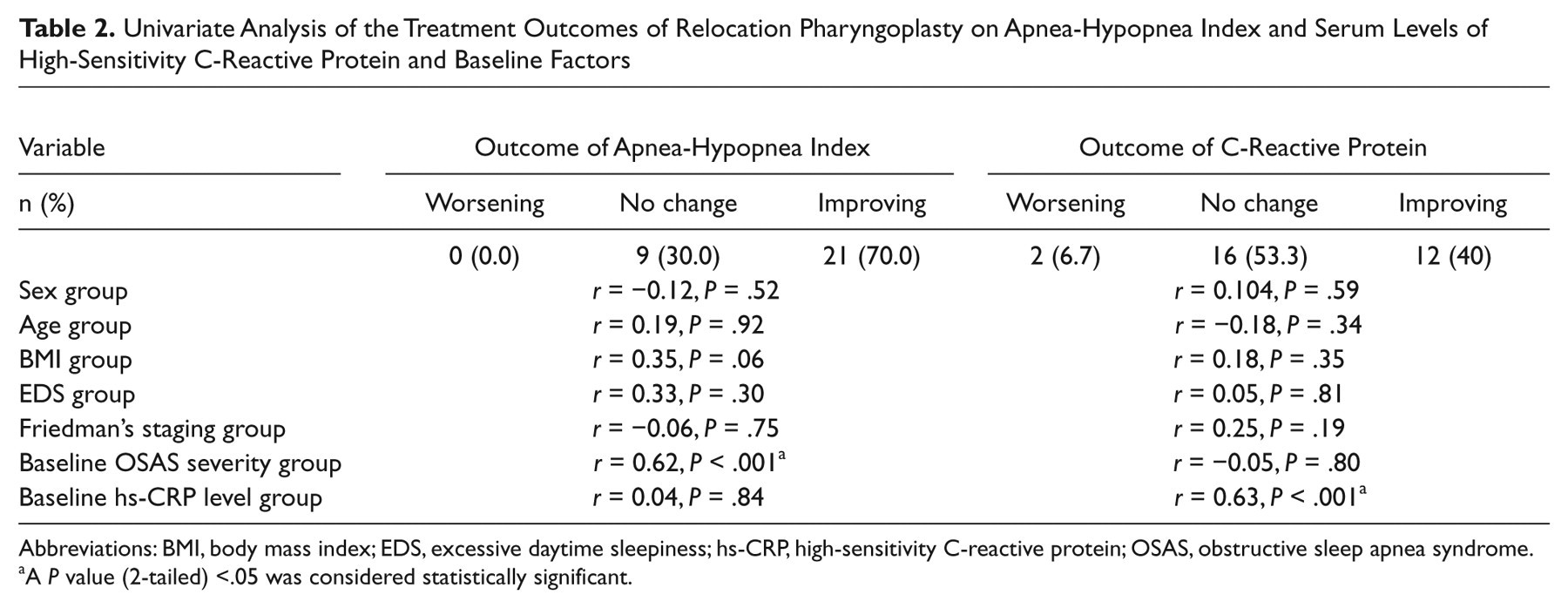
Abbreviations: BMI, body mass index; EDS, excessive daytime sleepiness; hs-CRP, high-sensitivity C-reactive protein; OSAS, obstructive sleep apnea syndrome.
A P value (2-tailed) <.05 was considered statistically significant.
Discussion
In the past, different clinical treatments, including CPAP therapy or upper airway surgeries, were considered to alleviate the severity of OSAS and to reduce cardiovascular risk factors (hs-CRP and/or other biomarkers)
12-15,17,18,20,22,23
or to control associated cardiovascular disease (
English Literature Review of Treatment Outcome of Obstructive Sleep Apnea Syndrome on Apnea-Hypopnea Index and Serum Levels of High-Sensitivity C-Reactive Protein
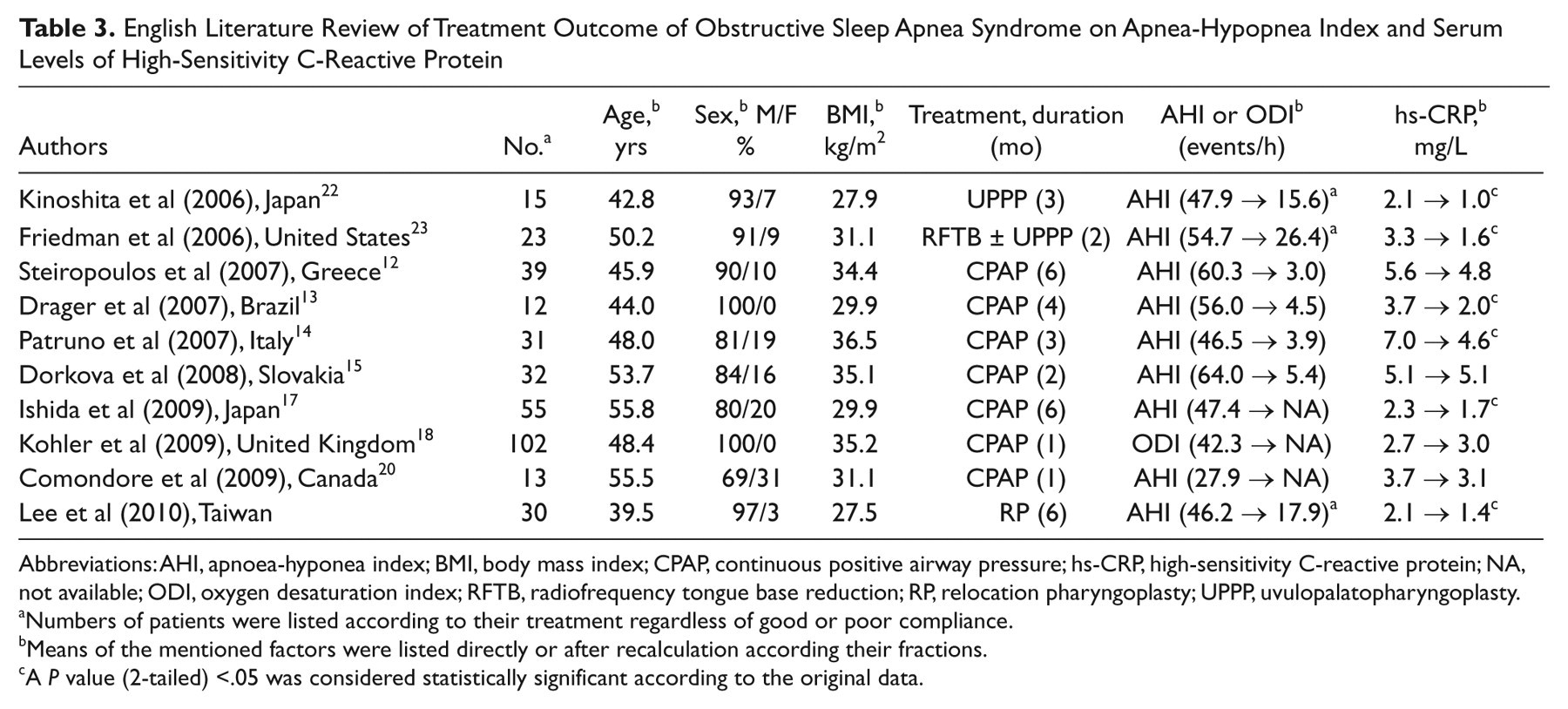
Abbreviations: AHI, apnoea-hyponea index; BMI, body mass index; CPAP, continuous positive airway pressure; hs-CRP, high-sensitivity C-reactive protein; NA, not available; ODI, oxygen desaturation index; RFTB, radiofrequency tongue base reduction; RP, relocation pharyngoplasty; UPPP, uvulopalatopharyngoplasty.
Numbers of patients were listed according to their treatment regardless of good or poor compliance.
Means of the mentioned factors were listed directly or after recalculation according their fractions.
A P value (2-tailed) <.05 was considered statistically significant according to the original data.
In an initial study investigating the role of RP in OSAS patients, a significant reduction of AHI, from 43.4 to 15.7, after 6 months postoperatively was reported. 24 RP includes (1) advancement of the soft palate that increases the retropalatal space without a sequel of velopharyngeal insufficiency 32 and (2) lateral pharyngoplasty that stabilizes the retroglossal space during sleep. 24 In the present study, 37% of OSAS patients experienced a significant correction of their daytime somnolence, 70% had a clinically significant improvement of their AHI, and 40% had a meaningful reduction of their serum hs-CRP levels when defining the improving outcome as reducing at least 1 degree of the EDS, OSAS severity, or hs-CRP level. That is, RP can greatly reduce sleep-related adverse events and proves to be an effective therapy to improve daytime spirits and the level of systemic inflammation in OSAS patients, which is in agreement with previous studies. 22,23
Despite significant improvement in AHI, only 13% of the patients cured their OSAS by RP. This underlies the necessity of long-term follow-up to provide multilevel surgery or multimodality treatment in symptomatic (such as snoring or EDS) or risky (high AHI or high hs-CRP) patients. Traditional UPPP may jeopardize sequential CPAP therapy for residual OSAS due to mouth leak. RP is aimed at enlarging the retropalatal airway by advancing, instead of excision of, the soft palate to ensure the palate-tongue lock during nose breathing. It is therefore possible that RP leads to not only a nondetrimental effect to CPAP use but also an increase of compliance attributable to decreased titration pressure postoperatively.
Although postoperative serum levels of hs-CRP dropped significantly from 2.06 to 1.40 mg/L, only the very severe OSAS patients had significant reductions of serum hs-CRP levels. Moreover, the baseline hs-CRP level was the only predictor of the improving outcome of hs-CRP. We speculate that the low improving rate of hs-CRP (40%) may be attributable, at least partially, to the setting in the present study because 10 (33%) patients presented with a low hs-CRP level at baseline and were not likely to see their levels reduced postoperatively. Similarly, 53% of the studied subjects had no EDS problem. Unlike our previous study, 21 we did not find a significant correlation between hs-CRP and AHI, and their improvement did not correlate in this study. We supposed that a smaller sample size (n =30 vs n = 65 21 ) or selection bias (surgical patients vs pooled patients 21 ) resulted in this dissociation. Therefore, we still need a further large-scale study to confirm their relationship. Nevertheless, serum levels of hs-CRP were particularly high (2.90 ± 2.57 mg/d L) and well correlated to AHI (r = 0.687, P = .028) in the very severe OSAS group of this study. We also found remarkable improvements of AHI and hs-CRP in this group. Accordingly, RP did help the very severe OSAS patients despite a low success rate in terms of AHI.
As expected, the study subjects with a very low ARCHD did not have a CHD event during their follow-up. We did not find a significant association between the ESS, AHI, hs-CRP, or ARCHD at baseline, and the association between the changes of AHI and hs-CRP was insignificant in this study (data not shown). To date, it remains uncertain whether therapies that lower hs-CRP levels will also result in lower cardiovascular event rates. Therefore, we suggest that the outcomes of AHI and hs-CRP may be equally important when engaged to reduce CHD risk in patients with OSAS, similar to the equivalent importance in the presentation of subjective (quality of life) and objective (respiratory disturbance) outcomes in treating OSAS. 33 Because most of the newly diagnosed OSAS patients have a low 10-year ARCHD (<20%), only large randomized studies with long-term follow-up will be able to compare the benefits of OSAS treatment in the prevention of a subsequent CHD event.
We are aware that the present study bares some limitations due to its design. First, this is a comparative, single-center study, and the evidence base might have been low due to lack of a control group. Second, we assessed only the hs-CRP parameter, and we did not measure other novel cardiovascular biomarkers 10 in the studied patients. Finally, other mechanisms that were not considered in this investigation might have played a role in the incidence of CHD. Body weight and proportion of gender (only 1 female in this study) might represent important factors; however, we did not systematically examine their effects in our study.
Conclusions
RP significantly improves disease severity and sleep parameters and reduces hs-CRP concentrations in selected patients with OSAS after 6 months postoperatively. However, on the basis of the current results, it does not represent a simultaneous reduction of ESS, AHI, and serum levels of hs-CRP for a longer follow-up period. Although patients with very severe OSAS are seldom cured by RP, their degree of daytime somnolence and elevated hs-CRP levels can be reduced remarkably. Residual AHI is not all that matters, and all aspects of the results of RP must be evaluated to draw meaningful conclusions. Further studies are needed to evaluate the influences of this operation on long-term changes in ESS, AHI, hs-CRP levels, ARCHD, and the development of CHD. In addition, early surgical intervention such as RP should be considered in OSAS patients with a high serum hs-CRP level to reduce the degree of systemic inflammation.
Author Contributions
Disclosures
Footnotes
Acknowledgements
The present study was supported by the National Science Council, Taiwan (NSC 97-2314-B-182A-064). The authors would like to thank Mrs Shin-Jao Lee, Department of Otolaryngology, Chang Gung Memorial Hospital, Taoyuan, Taiwan, for assisting in data collection.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.