
Abstract
Objectives. Increased levels of fatigue and perfectionism were noted during evaluation of cognitive behavioral therapy for the treatment of functional dysphonia. The investigators thus aimed to explore levels of general fatigue and perfectionism in patients with functional dysphonia and controls.
Study design. Case-control study.
Setting. Teaching hospital, United Kingdom.
Subjects and Methods. Patients recruited through speech therapy were asked to recruit a friend as a control, of the same sex and within 5 years of their age. An 11-point fatigue questionnaire, previously validated on a normal population, was analyzed using both Likert (0123) and bimodal (0011) systems, with a score greater than 4 on the bimodal system implying substantial fatigue. A 35-point perfectionism questionnaire was also completed and analyzed for “healthy” and “unhealthy” perfectionist traits.
Results. There were 75 cases and 62 controls. The mean fatigue score in patients with functional dysphonia was 17.0 and 14.4 for the controls (Likert, P = .009). Under the bimodal scoring system, the mean fatigue scores in functional dysphonia (5.10) and controls (3.01) were also significantly different (P = .003). The mean perfectionism scores were 98.9 for patients with functional dysphonia and 91.2 for controls (P = 0.043).
Conclusions. To the investigators’ knowledge, this is the first substantial report that fatigue and perfectionism scores are significantly elevated in functional dysphonia. Functional dysphonia is shown to be analogous to other medically unexplained physical symptoms that are also marked by generic somatopsychic distress and for which multiple factors are implicated in their onset and maintenance. This has implications for both research and treatment.
The classification of functional dysphonia remains disputed, with some authors using it narrowly to refer to a voice disorder arising from vocal misuse and others using it to refer to any nonorganic dysphonia. In the current study we defined functional dysphonia in this latter, broader sense of a dysphonia or aphonia where there was no detectable organic pathology or where what was detectable was not commensurate with the degree of vocal dysfunction. Defined thus, functional dysphonia (FD) is the most common disorder presenting to voice clinicians in the United Kingdom. 1 In a recent overview of a special issue of the International Journal of Speech and Language Therapy devoted to FD, Oates and Winkworth 2 noted that a consistent theme of the literature is that FD is a multifactorial condition. Although there is continuing debate about terms, models, and the relative importance of factors, all authors agree that the conceptualization and treatment of FD only make sense within a broad biopsychosocial framework and that psychosocial factors are particularly important in this condition. Baker 1 presents a useful summary of the psychosocial findings to date. Demographically, women are 6 to 9 times more likely than men to develop FD. 3,4 Patients with FD report higher levels of trait neuroticism and anxiety and more stress reactivity. 4,5 Roy and Bless 6 found that compared with a vocal nodule group, patients with FD are more introverted. There is mixed and inconclusive evidence on coping style, with some reports suggesting anxious coping and others repressive coping. 2 Psychiatric disorder is rare, but sufferers are more likely to be anxious and depressed and have a history of other medically unexplained symptoms. 5,7-9 Studies show that patients with FD were more likely to experience stressful life events in the year before onset, with House and Andrews 10 specifying that these events are more likely to involve situationally induced difficulty in expressing emotions, which they term concern over speaking out (COSO). Baker’s own recent work adds that patients were significantly more likely to have to have a history of physical or sexual abuse compared with a control group of organic voice disorders. 11
All of these findings are cross-sectional, and as Baker admits, researchers are “still grappling to understand the complex interrelationships” 1 between factors (p. 216). A narrative summary of this literature would be that individuals are predisposed to FD by neurotic and introvert/repressive personality, coping style, and early experience of adversity; that individuals are precipitated into FD by life events and dilemmas, particularly those in which action or expression is difficult; and that once established, FD is maintained by an interplay of physiological and ongoing psychosocial difficulties. This picture of FD is homologous with the emerging understanding of other medically unexplained symptoms (MUS), such as chronic fatigue syndrome (CFS), irritable bowel syndrome (IBS), and chronic pain. There is good evidence that these are also the result of an interplay of multiple factors, are more likely to occur in individuals with a tendency to neuroticism and introversion and with a history of adversity, are precipitated by life events and dilemmas, and tend to be maintained by an interplay of physiological and psychosocial factors ( Figure 1 ; see Deary et al 12 for a full review of this model).
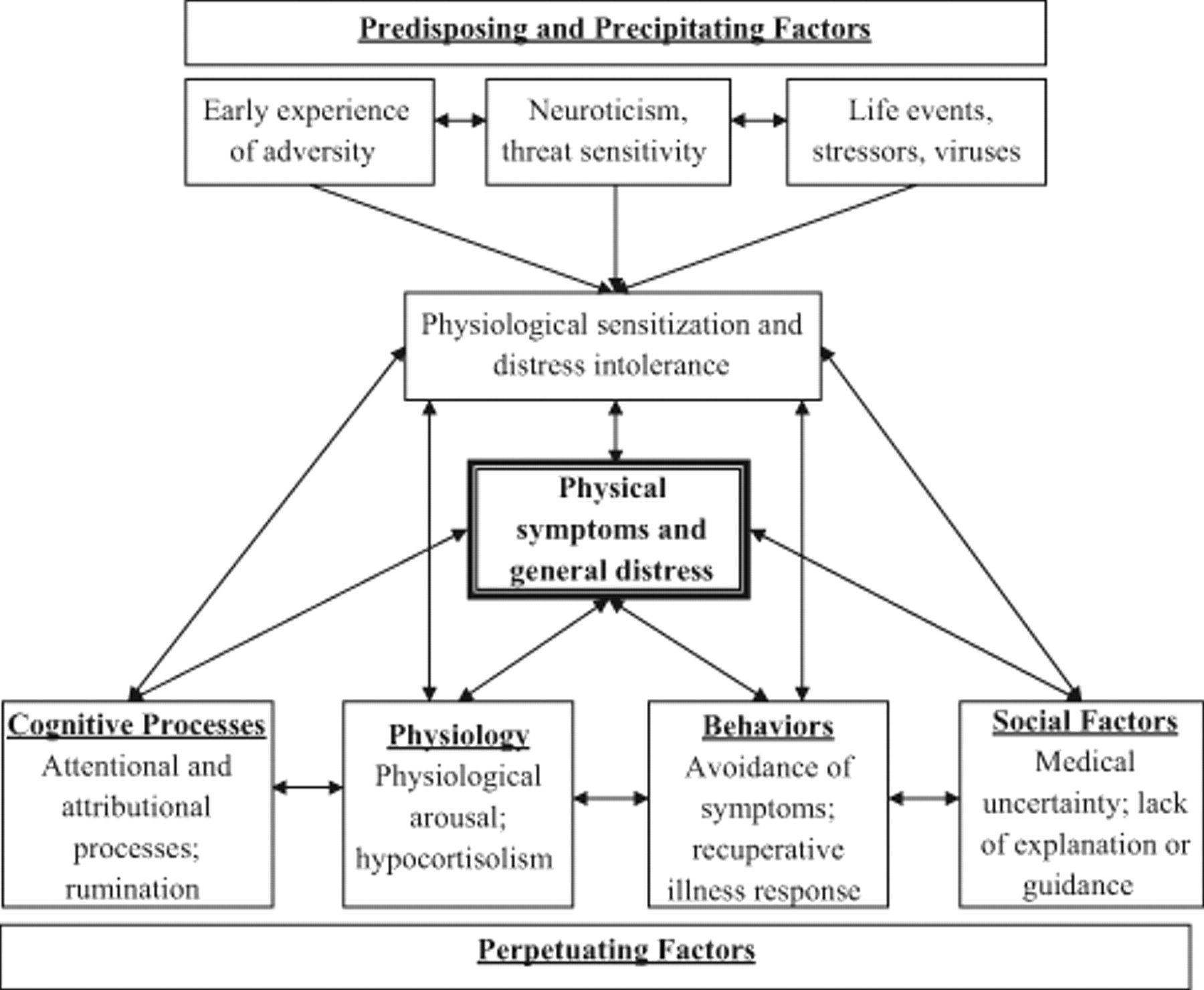
Biopsychosocial model of medically unexplained physical symptoms.
Our ongoing research program has sought to improve the understanding and treatment of FD by adopting a multifactorial approach to research and treatment. In developing our treatment we have used the above broadly cognitive behavioral model, which has been the theoretical basis of successful treatments in other medically unexplained conditions. This model operationalizes the research cited above by giving a framework with which to assess and address the interplay of predisposing, precipitating, and perpetuating factors in any given individual with FD. In the course of a pilot consecutive cohort study 13 and an ongoing randomized controlled clinical trial, cognitive behavioral assessment interviews confirmed the research findings above. These exploratory semi-structured interviews aimed to elicit a wide range of predisposing, precipitating, and perpetuating factors, including personality traits, life events, illness beliefs and behaviors, other physical and emotional symptoms, and interpersonal and social factors. The interviews indicated that FD seemed to present in individuals who were prone to worry and distress and who had gone through difficulties and major life transitions. In addition, these subjects reported 2 factors not highlighted in the FD literature: they felt fatigued, chronically low in energy, and lacking mental and physical stamina and they often described themselves as conscientious/perfectionist individuals who had persisted in trying to deal with life difficulties, perhaps to their detriment. These clinical observations fit with what is known of other MUS, for instance, CFS, where there is a cross-sectional association between CFS caseness and perfectionism. 14 This research conceptualizes perfectionism as comprising 2 related but independent factors: high self-standards and self-criticism concerning achievement of standards. 15 Although considerable attention has been given to the psychosocial well-being of patients with FD, less attention has been paid to their general physical health and levels of fatigue, and almost no research has focused on perfectionism.
The primary aim of the current study was to investigate whether patients with FD did experience fatigue in addition to their voice problems and to ascertain whether, as in other fatigued populations, this was associated with perfectionism. Our hypothesis was that patients with FD would have higher levels of fatigue and perfectionism than matched healthy controls in a cross-sectional survey.
Method
Subjects
Patients with FD were recruited through the speech therapy clinic at The Freeman Hospital, Newcastle upon Tyne, United Kingdom. This diagnosis was used in the widest sense: patients who were dysphonic or aphonic in the absence of organic pathology or for whom the pathology was minor and insufficient to explain the voice. Each subject was issued an information sheet explaining the study’s aims, and written consent for participation was obtained. Subjects were age and sex matched: patients were asked to recruit a friend to act as a control who was within 5 years of their age, was of the same gender, and did not have an altered voice. The controls completed the same questionnaires and returned them by post. No attempt was made to formally assess the voice quality of controls or to screen patients for medical causes of fatigue. The study was granted local research ethics committee approval.
Questionnaires
The Chalder Fatigue Questionnaire (CFQ)
This is an 11-item questionnaire (supplemental online appendix 1) with 4 response options per item, scored either on a Likert scale of 0 to 3 or on a bimodal scale of 0011. This was tested on more than 15,000 members of a general population and produced a mean score of 13.72 (95% confidence interval [CI], 13.65-13.79). 16,17
Multidimensional Perfectionism Scale (MPS)
This is a 35-item measure of 6 different facets of perfectionism (supplemental online appendix 2): doubts about actions, concern over mistakes, parental criticism, parental expectations, organization, and personal standards. 18 Questions are scored on a Likert scale of 0 to 5. The questionnaire breaks down into 2 super-factors: (1) doubts, concerns, and parental influence constitute unhealthy perfectionism and (2) personal standards and organization constitute healthy perfectionism. 19
Sample Size
A sample size calculation using the above general population fatigue scores aimed to achieve 90% power to identify a difference of 0.6 standardized differences. A total of 130 patients were set, which included a 10% surplus to accommodate nonparametric analysis. Given the method with which control data were obtained, it was anticipated that there would be a shortfall in the number of controls compared with cases.
Statistical Analysis
This was carried out using SPSS 15 (SPSS, an IBM Company, Chicago, Illinois). The 2-tailed independent-samples t test was used for the normally distributed data from the Likert-scored CHQ and MPS. When scored using the bimodal system, the CHQ was analyzed using the nonparametric Mann-Whitney U test. It was considered that although cases and controls were approximately matched for age, this would not match stringently enough for other covariables to allow a matched-pair analysis of results. As such the results were analyzed as unequal-sized independent groups.
Results
Cases and controls were well matched for gender and age ( Table 1 ). The mean CFQ fatigue score in patients with FD was significantly higher in the FD group; the difference between means was 2.56 (95% CI, 0.64-4.5.) Using the bimodal scoring system, the mean fatigue scores were also significantly different (P = .003, Mann-Whitney U). The mean total perfectionism scores were significantly higher for the FD group; difference between the means was 7.74 (95% CI, 0.23-15.3). When the MPS was scored for healthy and unhealthy perfectionist traits, the differences between the 2 groups were not significant.
Fatigue and Perfectionism in FD and Control Groups
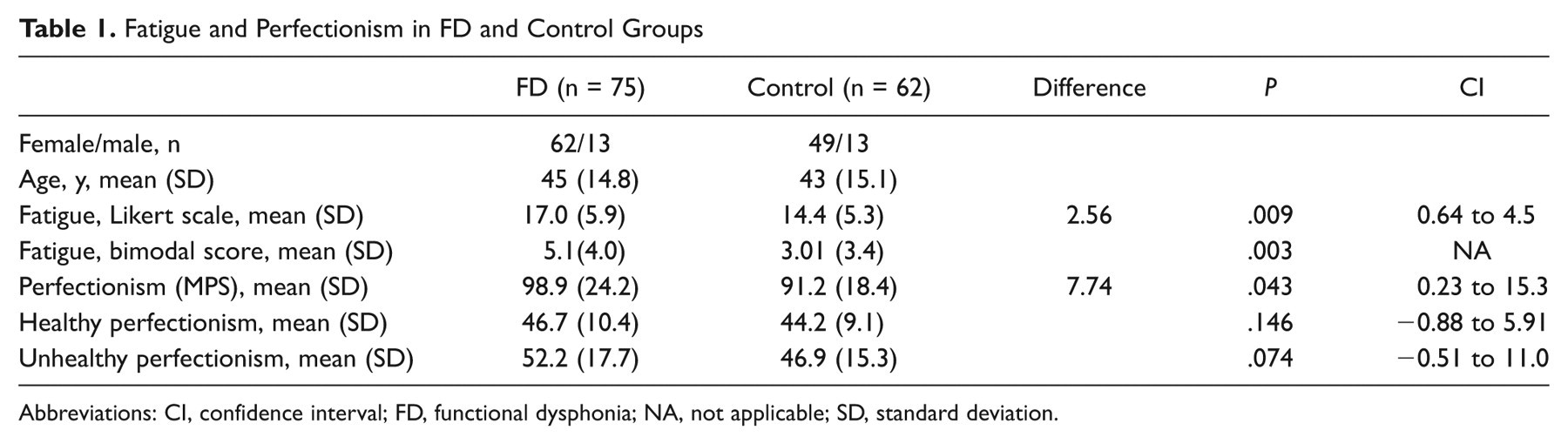
Abbreviations: CI, confidence interval; FD, functional dysphonia; NA, not applicable; SD, standard deviation.
Discussion
Main Findings
This is the first study to demonstrate elevated levels of fatigue and perfectionism among patients with FD. This was in line with our clinical observation and echoes findings in other medically unexplained conditions. Below we discuss these findings individually and the ways they might add to our understanding and treatment of FD.
Fatigue
The fatigue levels in the FD study patients were significantly higher than in healthy controls. To give an idea of the relative clinical significance of this level, comparison with other conditions may be useful. In a similar study of CFS patients, fatigue measured on the same scale was 24.2 (standard deviation [SD] 6.7); in an intervention study of fatigue in multiple sclerosis, fatigue measured on the same scale was 20.94 (SD 4.25). The levels in the current study were 17.0 (SD 5.9) in the FD group and 14.4 (SD 5.3) in the healthy controls. Thus, the level of fatigue is not as severe as in a condition for which fatigue is the primary complaint or one for which fatigue is a significant and recognized symptom, but the fatigue level is more than in the normal population. There are several possible reasons for this: fatigue could precede, coincide with, or be a consequence of the voice pathology (eg, be in part maintained by the effort of vocal production). Without inferring causality, the elevated fatigue would certainly seem to be a marker of a more generic ill health status in these patients, and along with previous studies showing elevated levels of anxiety and depression and high General Health Questionnaire 28 Scores (indicating poorer general health), elevated fatigue would suggest that FD is associated with not only psychological distress but also generic physical impairment.
This also further confirms the similarity of FD to other medically unexplained symptoms for which there are consistent findings of comorbidity with raised levels of anxiety, depression, fatigue, and pain. This has led researchers to suggest that medically unexplained physical symptoms be seen, along with anxiety and depression, as “common distress disorders” marked by a generic somatopsychic distress (ie, both physical and emotional). Some authors have suggested that diagnostic distinctions disguise deep similarities between syndromes, with there being a great deal of shared variance across conditions, particularly the co-occurrence of anxiety, depression, fatigue, and pain. 20-22 Seeing FD in this light has implications for understanding its genesis, maintenance, and treatment, as discussed below.
Perfectionism
Neuroticism/negative affectivity and introversion have been the main personality correlates of FD discussed in the literature. The present study adds the finding of a correlation between perfectionism and FD. Perfectionism breaks down into 2 subtraits: healthy perfectionism, a reasonable investment in doing things well; and unhealthy perfectionism, a preoccupation with self-doubt, self-criticism, and dissatisfaction with personal performance. The present study showed that patients with FD scored higher overall on general perfectionism, with a trend (P = .074) to be more unhealthily perfectionist. This echoes research in other physical and medically unexplained symptoms. Previous studies have shown links between general perfectionism and fatigue in a normal population 23 and in a CFS population. 14 Accounts of this link are necessarily speculative. Perfectionism as a whole may serve as a predisposing vulnerability that causes people to push themselves too hard, particularly to “soldier on” in times of distress. There is evidence of this kind of coping being prospectively associated with the genesis of IBS. 24 In FD this kind of coping may affect both voice and general well-being. Unhealthy perfectionism correlates highly with neuroticism, whereas healthy perfectionism correlates with conscientiousness. As such, a high-scoring perfectionist may combine a tendency to distress and an imperative to “carry on” regardless of distress. However, the focus on personality risks pathologizing the individual, and it may be the interaction of traits with life events, other symptoms, and circumstance that is important, to which we now turn.
Understanding the Genesis and Maintenance of FD
Van Kessel et al 24 showed that all-or-nothing coping predicted later IBS. Attempting to persist in the face of life events, difficulties, and illness could have physiological consequences. A recent publication 25 proposed that this dynamic of stress plus persistence is central to the onset and maintenance of CFS. These authors propose that sustained autonomic arousal, brought on by life events and ongoing attempts to cope with them, has long-term consequences on physiology resulting in fatigue, pain susceptibility, anxiety, and depressed mood. The effects of prolonged stress on physiological and immunological states in MUS in general have been reviewed by Deary et al. 12 Although research is still in its early stages, there is a consensus in this research that the link between stress and symptoms is likely to be mediated by changes in the function of the hypothalamic–pituitary–adrenal axis. This interaction of coping style and life events leading to physiological “burnout” may also be at play in FD. We know that there is likely to be a history of life events; adding perfectionist, all-or-nothing coping to this could have detrimental health consequences and could also explain the current study’s other finding of elevated fatigue levels in this population and previous findings of poor general health. 7 Vocal disability brings these clients to the clinic but may be only one facet of a much more general impairment, the vocal symptom being the most obvious but not the only response to prolonged difficulty.
Turning to maintenance of symptoms once established, we know from other MUS that multiple factors interact to keep them going. For instance, in CFS, all-or-nothing coping, activity avoidance, and beliefs about symptoms being harmful (cognitive and behavioral perpetuating factors) seem to predict long-term fatigue. Within this multifactorial framework, the perfectionism and fatigue findings can be integrated into what we already know about the perpetuation of FD.
Fatigue and poor general health, anxiety, and depression (physiological, affective, and cognitive factors) may all affect behavior, leading to avoidance of anxiety-provoking situations, time off work, reduced activity, and social withdrawal, all of which could cause or perpetuate anxiety, low mood, fatigue, and reduced voice use. Perfectionism, particularly the self-critical aspects of it, could drive ongoing self-defeating attempts to achieve high self-standards despite illness or all-or-nothing withdrawal from previous activities. Both of these coping styles are likely to result in fatigue and low mood caused by dissatisfaction with current ability. This picture certainly fits with common clinical presentations. More specific illness beliefs may be important, with clinical experience suggesting that many individuals have catastrophic beliefs around voice symptoms and the effect of voice use, which may further lead to voice disuse, tension, and general activity avoidance. The latter dynamic remains to be elucidated, but this proposed interacting, multifactorial framework gives the research a coherent basis on which to base future investigation.
Treatment
The current literature on dysphonia has a tendency to paint a rather homogenous picture of distress plus repression as the main pathogenic factor in vocal dysfunction. However, the present work and other research show that, first, this profile is common to many other physical symptoms, and, second, other factors in play must be considered in research and treatment. The 2 most striking things about our study group were how tired and ill they were in general and how each individual had a unique set of reasons for being so. The individualized cognitive behavioral assessments we used on trial patients helped identify these unique factors and target them in treatment by, for instance, breaking the cycle of fatigue by challenging beliefs about symptoms and by encouraging activity resumption. The current study combined with previous research suggests that this multifactorial model is applicable to FD and that to improve our interventions we should move beyond using voice strategies and encouraging emotional expression. 11 Treatment should also target not only anxiety and low mood but also the associated fatigue and unhelpfully high self-standards that may play a part in causing and perpetuating the symptom cluster. This work forms the basis of our current randomized controlled trial.
Limitations
The present study has the primary limitation of all cross-sectional studies: the significant associations tell us nothing about causality. More specifically, it could be argued that the controls—friends of the patient with FD—may be more likely to demonstrate similar personality traits than the general population. However, differences in fatigue and perfectionism scores were very similar to the differences in case and controls in the CFS and perfectionism study cited in the introduction in which controls were recruited through staff. It is also plausible that fatigue is a marker of illness in general (although this is less likely with perfectionism), and future studies should attempt to replicate these findings with an organic voice disorder control group.
Conclusion
Patients with FD are both more fatigued and perfectionist than healthy controls. Understanding how these factors play into the illness experience of people with this condition can improve our understanding of how FD develops and how we can improve the treatment of those affected by it.
Author Contributions
Disclosures
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
This article was presented in part at the AAO-HNSF Annual Meeting & OTO EXPO; September 26-29, 2010; Boston, Massachusetts and the Otorhinolaryngological Research Society in London, September 2009. Winner of the Angell-James best free paper prize.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.