
Abstract
Objective. To determine clinicopathologic predictors of recurrence and survival in patients with spindle cell squamous cell carcinoma (SpSCC).
Study Design. Historical cohort study.
Setting. Tertiary care hospital.
Subjects and Methods. Forty-eight patients (mean age, 65.2 years; 35 men, 13 women) who underwent definitive treatment for pathologically confirmed SpSCC between 1987 and 2009 were identified and reviewed. The main outcome measures were time to recurrence and overall survival, while controlling for clinical and pathologic parameters (age, sex, TNM classification, stage, tumor subsite, smoking status, treatment modality, margin status).
Results. Of 48 patients, there were 25 oral cavity, 15 laryngeal, 7 oropharyngeal, and 1 maxillary sinus tumors. Treatment included surgery in 32, radiation in 9, and concurrent chemoradiation in 7 patients. The 3-year overall survival for the cohort was 62% with a median follow-up of 59 months; 52.1% (25/48) of patients developed a recurrence, and 88% (22/25) recurred locally or locoregionally. Recurrence occurred within 2 years in 72% (18/25) of patients. Age, sex, initial T and N classification, overall stage, tumor subsite, smoking status, treatment modality, and margin status were not predictive of recurrence or overall survival.
Conclusion. Patients with SpSCC are at high risk of developing locoregional recurrence, but no measured clinical or pathologic parameter was predictive of survival. Although overall survival is similar to that of patients with conventional SCC, closer follow-up should be considered in these patients to allow earlier detection and treatment of these locally aggressive tumors.
The spindle cell variant of squamous cell carcinoma (SpSCC) is a type of squamous cell carcinoma (SCC) that occurs at all sites in the head and neck. The majority of these are in the oral cavity, oropharynx, and larynx, but multiple other sites have been described. 1 There are few published series in the literature regarding the prognosis of these patients or risk factors associated with recurrence and survival. 1-4 Although SpSCC has features of both an epithelial and a mesenchymal tumor under microscopy, its behavior can be difficult to predict. 5 These tumors are currently staged within the American Joint Committee on Cancer (AJCC) staging guidelines of conventional SCC, although there may be differences in behavior or prognostic factors. The purpose of this study was to determine clinical and pathologic predictors of recurrence and survival in patients with SpSCC.
Methods
Study Population
We conducted a retrospective review of patients at the University of Michigan who underwent definitive treatment for pathologically confirmed SpSCC between 1987 and 2009. Patients were identified through the university’s pathology department database searching under “squamous cell carcinoma” with either “spindle” or “sarcomatoid” as modifiers. Cases not involving the upper aerodigestive tract (ie, skin) were excluded. Patient information was collected through the electronic medical record. Patients were also excluded if they were never seen or did not follow up at the University of Michigan for their cancer surveillance. There were 62 patients initially identified; 9 of these patients were never seen at the University of Michigan (pathology only review) and 5 did not have follow-up after their initial consultation. These 5 excluded patients had similar age (mean 69.2), sex (4 men, 1 woman), tumor subsite (2 oral cavity, 3 larynx), and tumor stage (1 stage II, 2 stage III, 2 stage IV) as the study cohort. All patients were staged based on the 2002 AJCC staging system, and this study was approved by the Institutional Review Board at the University of Michigan (HUM00033266).
Pathologic Correlation
All cases were confirmed by review of the pathologic specimens. The diagnosis of SpSCC was made when a malignant spindle cell neoplasm was identified arising from a mucosal squamous epithelial surface. Many cases had invasive or in situ SCC associated with them, but these were not requisite for the diagnosis. Routine immunohistochemical staining was not used.
Statistical Analysis
Variables of interest were age, gender, tumor subsite, T stage, N stage, M stage, smoking status (never, ever [quit >6 months ago], current), treatment modality, margin status (recorded as positive or negative), and adjuvant treatment. The outcomes of interest were time to recurrence (TR) and overall survival (OS). TR and OS were defined as the time to event from the beginning of treatment.
Survival estimates were computed using the Kaplan-Meier method. Univariate and multivariate Cox models were used to test the association of tumor subsite and treatment modality with decreased survival and time to recurrence independent of other tested variables. All statistical analyses were performed using SAS (version 9.2) software (SAS Institute Inc, Cary, North Carolina).
Results
Forty-eight patients who underwent definitive treatment for pathologically confirmed SpSCC between 1987 and 2009 were identified. The mean age was 65.2 years (range, 22-86), and the male/female ratio was 35:13. There were 25 oral cavity, 15 larynx, 7 oropharynx, and 1 maxillary sinus tumors. Twelve patients were stage I, 6 patients were stage II, 8 patients were stage III, and 17 patients were stage IV. Primary treatment included surgery in 32, radiation in 9, and concurrent chemoradiation in 7 patients.
The 3-year Kaplan-Meier estimate of OS for the entire cohort was 62% with a median follow-up of 59 months. There was a trend toward a worse overall survival comparing oral cavity vs laryngeal tumors, but this difference was not significant in a univariate Cox model ( Figure 1A , P = .17). There was also no statistically significant difference in recurrence among the different tumor subsites ( Figure 1B , P = .15). The patients who developed a recurrence were relatively equally distributed among the 3 subsites; 52.1% (25/48) of patients developed a recurrence, and 22 of 25 patients recurred locally or locoregionally. One- and 2-year probability of recurrence-free survival for all patients using the Kaplan-Meier method was 79% and 51%, respectively. Among those patients who developed a recurrence, 72% (18/25) of patients did so within 2 years. Whether the tumor treated at the University of Michigan was a primary or recurrent tumor on our initial evaluation was not associated with overall survival (P = .23).
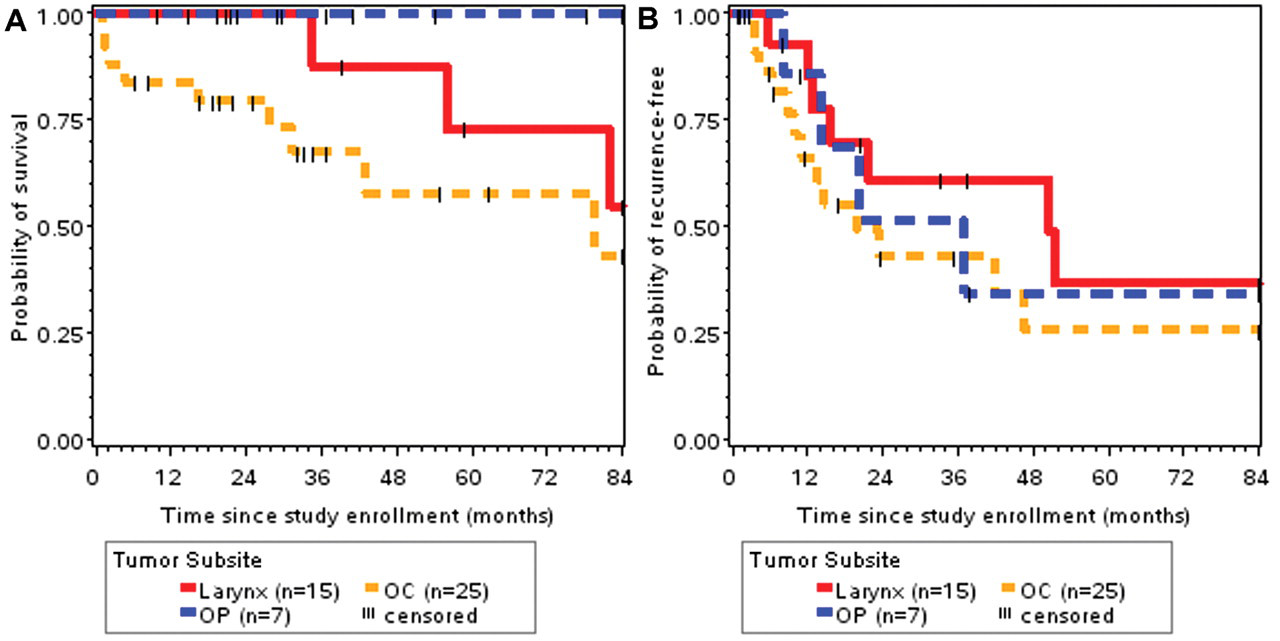
Overall survival (A) and time to recurrence (B) Kaplan-Meier survival plots stratified by tumor site. OC indicates oral cavity; OP, oropharynx.
There were no statistically significant differences in survival when comparing stage at diagnosis (2-year: 100%, 83%, 100%, 76%; and 5-year: 32%, 83%, 80%, 68% for stages I, II, III, and IV, respectively, Figure 2A ) or smoking status (2-year: 85%, 92%, 93%; and 5-year: 71%, 69%, 54% for current, ever, and never, respectively, Figure 2B ). There were no differences in time to recurrence or overall survival for any clinical or pathologic variables in the study.
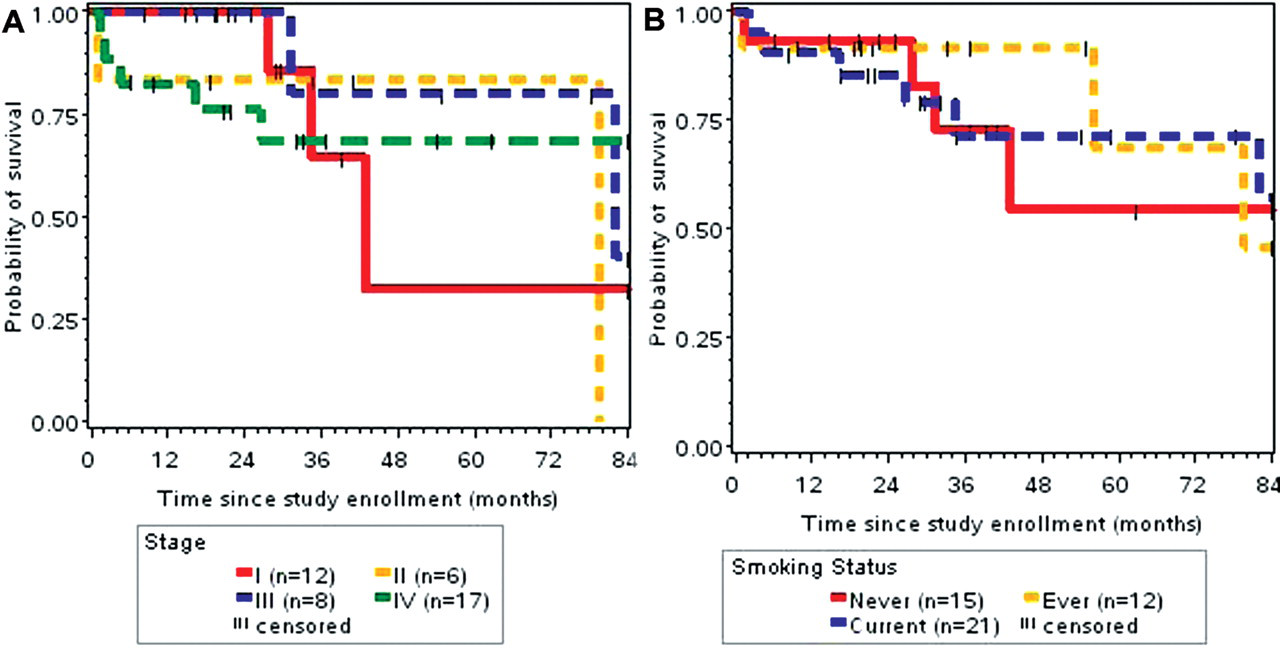
Overall survival Kaplan-Meier survival plots stratified by tumor stage (A) and smoking status (B).
Analysis by tumor subsite revealed no differences in recurrence rates or survival for oral cavity tumors based on any clinical or pathologic variables tested. Within the oropharynx subgroup, there were no differences in survival between patients treated with chemoradiation or surgery with an oropharyngeal primary tumor ( Figure 3A ). Three patients were treated with surgery and 4 patients with chemoradiation. Three of the 4 patients treated with chemoradiation developed a recurrence, and all were salvaged with surgery. There was no significant difference in the development of a recurrence in the oropharynx, although treatment groups were small ( Figure 3B ).
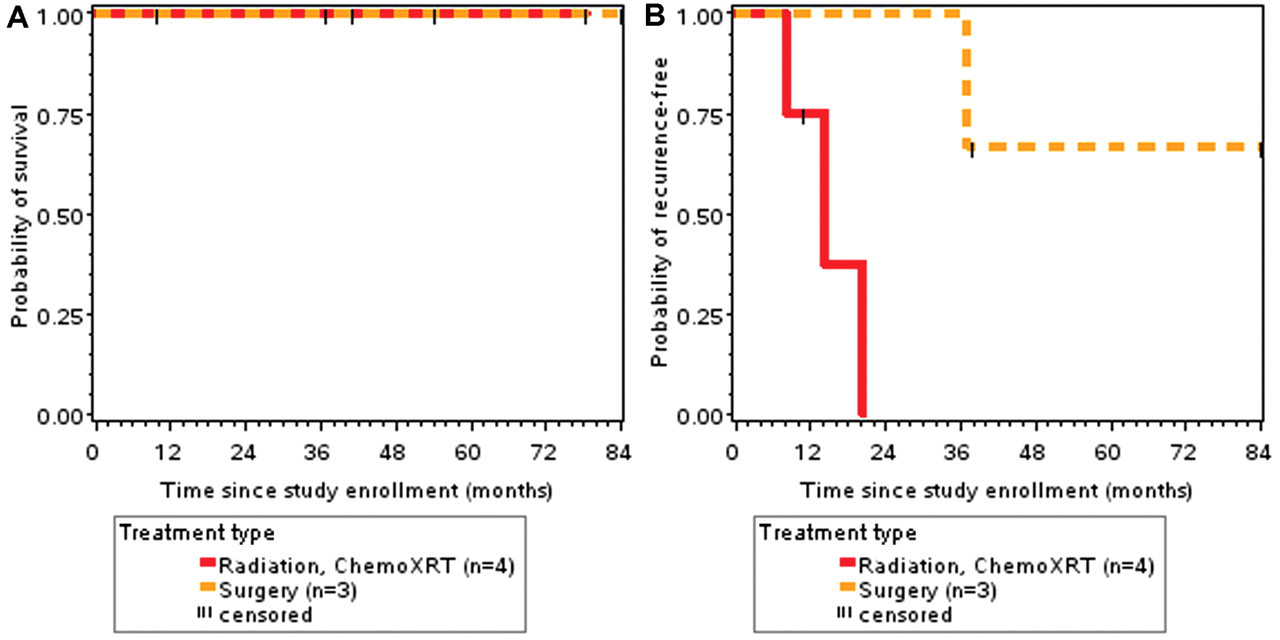
Overall survival (A) and time to recurrence (B) Kaplan-Meier survival plots stratified by treatment type (surgery vs radiation or chemotherapy [chemoXRT]) within the oropharynx.
There were 15 patients with laryngeal tumors; 10 patients were treated with radiation with or without chemotherapy and 5 patients were treated with surgery. There were no differences in survival between patients treated with chemoradiation or surgery with a laryngeal tumor ( Figure 4A ). There was a significant difference in recurrence rate between patients first treated with radiation with or without chemotherapy (6/10) compared with primary surgical treatment (1/5) ( Figure 4B ). Interestingly, 3 of the 6 treatment failures were salvaged with surgery.
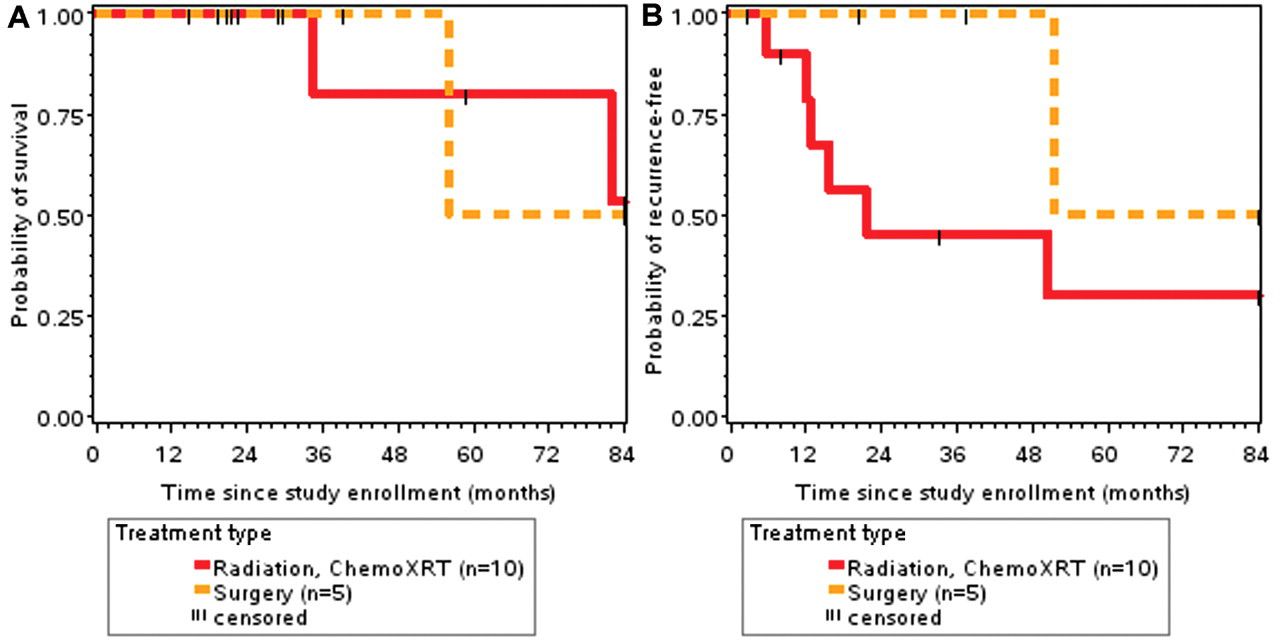
Overall survival (A) and time to recurrence (B) Kaplan-Meier survival plots stratified by treatment type (surgery vs radiation or chemotherapy [chemoXRT]) within the larynx.
Discussion
This study shows that the clinical and pathologic variables examined were not able to predict prognosis in SpSCC. To our knowledge, this study represents the second largest case series in the literature and has the longest follow-up time available for patients with SpSCC. SpSCC is relatively uncommon, and there are few case series in the literature describing clinicopathologic characteristics and outcomes. 1-4
The nomenclature of SpSCC in the head and neck has been divisive: these tumors have been called carcinosarcoma, pseudosarcoma, and sarcomatoid squamous cell carcinoma. 1 We have elected to use the term spindle cell variant because this is an epithelial cell tumor with morphologic differentiation toward spindle or sarcomatoid cells. This was validated by Choi et al, 5 who looked at loss of heterozygosity in chromosomes known to be associated with SpSCC. Those investigators found an 80% concordance rate when comparing mutations within these 2 cell types, leading them to conclude that these tumors originate from 1 cell but are at different evolutionary stages at both a molecular genetic and a morphologic level. Gleason et al 6 also established that p63, a transcription factor found in epidermal stem cells, is active in proliferating cells from patients diagnosed with SpSCC. Similarly, Ansari et al 7 found identical patterns of p53 protein expression in 95% of tumors when comparing the spindle and epithelial components within a tumor. Further evidence demonstrates that these tumors metastasize in the way of an epithelial carcinoma.
This study also shows that SpSCC has a high propensity to recur locally although overall survival is similar to conventional SCC. Subsites of this disease include the larynx, pharynx, and oral and nasal cavities 1 (in descending order), and case reports of tumors in the maxillary sinus and trachea have been reported. 8,9 More than half of our patients developed a recurrence, with 88% of these reoccurring locally. Local or regional recurrence is consistent with other reports in the literature. Ellis and Corio 3 reported that 69% of their patients recurred during their study period (length of follow-up not reported).
In our series, overall survival was similar to that of patients with conventional SCC, although we did not design a controlled study to test this hypothesis. Our survival rates are somewhat better than those reported in the literature for SpSCC. Su et al 2 identified 18 patients with oral cavity and oropharyngeal SpSCC and found a 3-year overall survival of 27.5%. They observed a local recurrence and distant metastasis rate of 73.3% and 33.3%, respectively. These differences are probably attributable to the variability of stage at presentation, the heterogeneity of our group (the inclusion of laryngeal primary tumors will improve survival), and the evolution of treatment paradigms in head and neck cancer. These patients do not appear to have been treated with adjuvant treatment. Ellis and Corio 3 reported an overall survival for patients with SpSCC of the oral cavity at 31% (14/45). The mean survival for those who died of disease was less than 2 years. Again, oral cavity tumors appear to behave more aggressively than other subsites in these studies.
Previous groups have examined tumor factors such as depth of tumor and invasion into the surrounding tissues to identify risk factors for recurrence and survival. Leventon and Evans 1 found that more invasive tumors have worse overall survival after examining 20 patients with pathologically confirmed SpSCC. Invasive tumors were defined as invading “muscle, minor salivary or accessory respiratory glands, or bone.” We did not stratify by this variable, but these patients appeared to have mostly T4 tumors by description. Our study found no significant recurrence or survival difference based on T stage. Most of our invasive tumors were in the oral cavity, and in our cohort, this was a trend toward a worse prognosis without reaching significance.
The presence of an exophytic tumor has been historically described as a favorable prognostic factor in some series. 1 There is no definition of an exophytic tumor in the literature, and this can be both a clinical and a pathologic diagnosis. Iguchi et al 10 divided these further, associating endophytic tumors with a higher rate of nodal metastasis and worse survival. 10 We found no difference in survival based on the presence of an exophytic tumor in this study (data not shown). This may be due to the variability of the definition of an exophytic tumor or limited sample size.
Within the group of 15 patients with a laryngeal primary tumor, 10 patients were treated with primary radiation with or without chemotherapy and 5 patients with surgery. There were 6 treatment failures in the radiation group vs 1 in the surgery group. In addition, 4 of the 6 patients who received radiation as primary treatment had T1 glottic tumors. It is well established in the literature that cure rates of T1 and T2 glottic tumors treated with radiation are greater than 80%. 11 Although our numbers were small, a reasonable inference is that these tumors are not as radiosensitive to normal radiation regimens and that surgery may be a better option. Indeed, of the 6 patients who developed a recurrence in the radiation group, 3 were salvaged with surgery. This is similar to the experience of Lewis et al 4 at the Mayo clinic. They found an 18% recurrence rate and a 50% overall survival rate with a median follow-up of 6.4 years in patients treated with surgery for laryngeal SpSCC. All these patients were treated with surgery as their primary modality.
In the oropharyngeal group, 4 patients were treated with chemoradiation and 3 patients were treated with surgery. Three of the 4 patients treated with chemoradiation developed a recurrence, and all were salvaged with surgery. There were, however, no differences in overall survival between the 2 groups. Our first observation is that the number of patients with oropharyngeal SpSCC is relatively small. At our institution, primary treatment of these tumors is with chemoradiation, and the diagnosis of SpSCC is thus made on a small biopsy of the tumor without the entire specimen, allowing for a sampling error. Multiple studies stress serial examination of tissue specimens because this lesion can be mistaken for other malignancies or miss the spindle cell component completely. 1,10
Our second observation is the high failure rate of oropharyngeal tumors treated with chemoradiation. Although the sample size is again small, a 75% recurrence rate is high and all of these patients could be salvaged with surgery, which was unexpected. Further understanding of the tumor biology of SpSCC would yield more information about appropriate treatment for these patients.
Limitations of this study include lack of a control group to make comparisons with conventional SCC, although this was not a primary objective. There may also have been selection bias as we are a tertiary care referral center, and many patients may have failed other treatments before coming to our center.
Conclusion
Patients with SpSCC are at high risk of developing locoregional recurrence compared with conventional SCC, but no measured clinical or pathologic parameter was predictive of survival. Although overall survival is similar to conventional SCC, closer follow-up should be considered in these patients to allow for earlier detection and treatment of these locally aggressive tumors. Our data indicate that laryngeal and oropharyngeal SpSCC may respond better to primary surgical therapy rather than chemoradiation.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.