
Abstract
Objectives. Tympanostomy tube (TT) biofilm formation may lead to refractory otorrhea and occlusion. Biofilms are commonly composed of multiple microbial species. One species may promote or inhibit biofilm formation by other species. The aim of this study was to determine if Haemophilus influenzae (HI) promotes the development of Pseudomonas aeruginosa (PA) biofilm on TTs.
Study Design. Controlled, in vitro.
Setting. Academic research laboratory.
Subjects and Methods. Fluoroplastic TTs (20 per group) were exposed to plasma, allowed to dry, and cultured with HI for 7 days. TTs were either gas sterilized or treated for 24 hours with 10 or 3000 µg/mL ciprofloxacin. Half of the TTs from each treatment group underwent bacterial counts or scanning electron microscopy. The remainder, as well as TTs not exposed to HI, were cultured with PA for 4 days and treated with gentamicin to kill planktonic PA. Biofilm formation was quantified with bacterial counts.
Results. TTs treated with ciprofloxacin 3000 µg/mL had lower HI counts than TTs treated with 10 µg/mL (P = .0001), but viable HI persisted. PA biofilm formation on TTs with prior HI biofilm and treated with ciprofloxacin 10 µg/mL or gas sterilization was not different than TTs without HI. Less PA biofilm formed on TTs with HI treated with 3 mg/mL ciprofloxacin (P = .002).
Conclusions. HI biofilm does not promote PA biofilm formation on TTs. Use of high-dose ototopical therapy to clear HI may reduce subsequent PA biofilm formation.
Keywords
Posttympanostomy tube (TT) otorrhea is common and occasionally persistent, requiring potentially extensive treatment and expense. 1 Refractory otorrhea may be due to biofilm formation on the TT.2,3 Pathogens isolated from such refractory cases are commonly chronic middle ear pathogens, such as Pseudomonas aeruginosa (PA) and anaerobes,3,4 whereas acute post-TT otorrhea commonly involves acute airway pathogens. 5 Chronic middle ear pathogens, such as PA, can be particularly difficult to eradicate, in part because of their inherent antimicrobial resistance and their propensity to form biofilms, which provides added resistance to antimicrobial therapy and host defenses. 6
It is unclear what leads to the emergence of chronic middle ear pathogens in post-TT otorrhea. It is well known that microbes may promote 7 and inhibit 8 other microbial growth. Haemophilus influenzae (HI) is one of the most common pathogens in acute post-TT otorrhea 5 and a capable biofilm former on both mucosal and plastic surfaces, 9 in contrast to Streptococcus pneumoniae (C. Ojano-Dirain, unpublished observations). 10 Thus, we sought to determine if HI promotes the growth and development of PA biofilm on TTs in an in vitro model.
Materials and Methods
Study Design
Fluoroplastic TTs were exposed to plasma, because blood has been shown to promote biofilm formation on TTs, 11 and allowed to dry overnight. TTs were cultured with HI in microtiter plates for 7 days and then exposed to ethylene oxide gas sterilization (yielding complete eradication of viable HI without loss of residual cellular debris), ciprofloxacin (10 or 3000 µg/mL, yielding killing of HI and removal of cellular debris akin to in vivo exposure with systemic and topical administration, respectively) for 24 hours or no treatment (control). TTs from each treatment group underwent analysis (ie, bacterial counts or scanning electron microscopy), without exposure to PA. The remainder of HI-exposed TTs, as well as additional, fresh TTs not exposed to HI, were cultured with PA for 4 days. TTs were treated with 200 µg/mL gentamicin to kill planktonic organisms. A group of TTs cultured with PA was not exposed to gentamicin, to represent total (planktonic and biofilm) bacterial load. Bacterial growth was quantified by bacterial counts (18 samples per group) and scanning electron microscopy (2 samples per group). Because of the large numbers of samples involved, the study was run in 2 batches, with equal distribution of samples. As this study involved neither human nor animal subjects, it was exempt from institutional review.
TTs and Preparation
Armstrong beveled grommet fluoroplastic TTs (Medtronic ENT, Jacksonville, Florida) were used. All TTs were immersed in human plasma that was donated by a local blood bank. After 24 hours, TTs were removed from the plasma and allowed to dry overnight. A total of 162 TTs were used and divided accordingly among the treatments ( Table 1 ).
Experimental Groups, with Number of Tympanostomy Tubes Analyzed for Quantitative Bacterial Counts, Scanning Electron Microscopy (SEM), and Excluded Because of Values More Than 2 Standard Deviations from the Group Mean
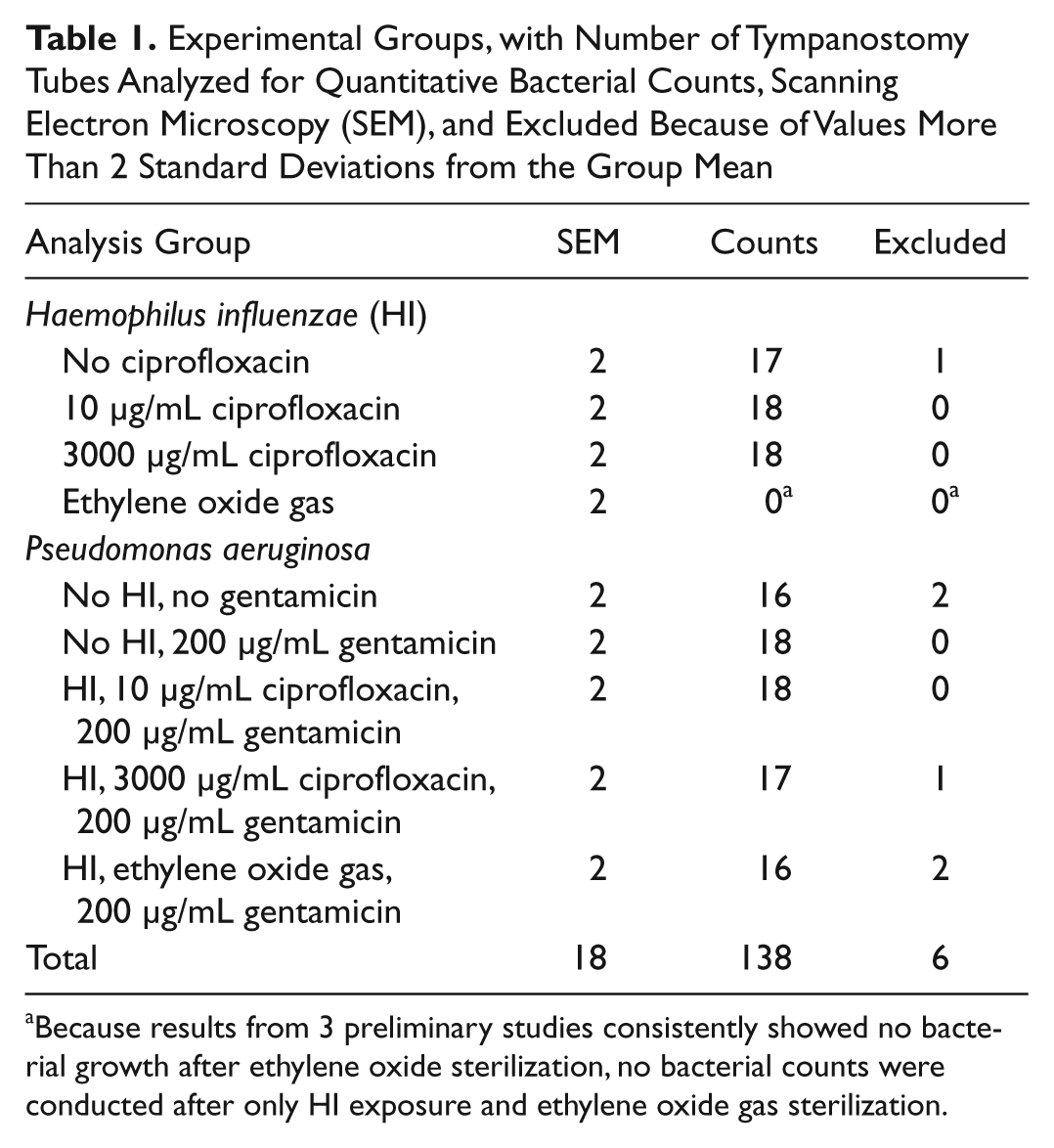
Because results from 3 preliminary studies consistently showed no bacterial growth after ethylene oxide sterilization, no bacterial counts were conducted after only HI exposure and ethylene oxide gas sterilization.
Bacterial Strains and Preparation
HI 62094 (kindly donated by Dr Peter Stroman, Fort Worth, TX) and PA (strain PAO1) were used. Culture media for HI were brain heart infusion (Becton Dickinson, Sparks, Maryland) supplemented with 2 µg/mL nicotinamide adenine dinucleotide (Sigma, St Louis, Missouri) and 10 µg/mL hemin (Remel, Lenexa, Kansas). Specimens were cultured in 96-well microtiter plates at 37°C for 7 days, as pilot studies revealed mature HI biofilms after 4 days. Nutrient broth was replaced daily. After 7 days, TTs were treated with either ethylene oxide gas sterilization, ciprofloxacin (10 or 3000 µg/mL), or no antimicrobial agent (control). Results from 3 preliminary studies consistently showed no bacterial growth after ethylene oxide sterilization, so no bacterial counts were conducted on 7-day HI after gas sterilization.
TTs to be exposed to PA were placed in 96-well microtiter plates containing PA in tryptic soy broth (MP Biomedicals, Solon, Ohio) and maintained at 37°C for 4 days since previous studies revealed mature biofilms with PA after 2 days. Nutrient broth was replaced daily. After 4 days, gentamicin (200 µg/mL; Sigma) was added to the broth to eradicate planktonic organisms.
Bacterial Counts
TTs were washed 4 times for 5 minutes by adding 200 µL 1 molar phosphate-buffered saline (PBS) to each well. PBS washes were aspirated using a sterile glass Pasteur pipette (Fisher Scientific, Fair Lawn, New Jersey). TTs were then transferred to 15-mL flip-top conical tubes (Thermo Fisher Scientific, Rochester, NY) containing 2 mL of PBS with 5 parts per million Tween-80 (Fisher Chemical, Fair Lawn, New Jersey). The conical tubes were placed into a water bath and sonicated (Branson 2510; Branson Ultrasonics, Danbury, Connecticut) for a total of 7.5 minutes, with serial 1.5-minute sonication exposures separated by a 1-minute rest. After sonication, tubes were vortexed at the highest setting (setting 8) for 15 seconds, serially diluted, and spread plated in triplicate on chocolate or tryptic soy agar plates for HI and PA, respectively. Specimens with prior HI and PA exposure were plated on both chocolate and tryptic soy agar to check for the presence of HI after subsequent PA culture. Plates were incubated for 18 to 24 hours at 37°C, and colonies were counted manually.
Scanning Electron Microscopy
Representative TT samples not processed for bacterial counts were fixed in 1-mL Trumps fixative (1% glutaraldehyde, 4% formaldehyde in PBS) and stored at 4°C until processed. Specimens were washed 3 times with PBS for 10 minutes and then fixed for 1 hour in 1% osmium tetroxide in PBS (Electron Microscopy Sciences, Hatfield, Pennsylvania). Specimens were washed once with PBS and 3 times with deionized water for 10 minutes each. Specimens were dehydrated in ethanol series for 10 minutes each (25%, 50%, 75%, 95%, 100%) and then hexamethyldisilazane (Electron Microscopy Sciences) for 5 minutes. Specimens were allowed to air dry overnight. Specimens were sputter coated with gold/palladium with argon gas (Desk II sputter coater; Denton Vacuum USA, Moorestown, New Jersey) for 45 seconds and stored under vacuum until imaged (Phenom scanning electron microscope; FEI Company, Hillsboro, Oregon).
Statistical Analysis
Data were analyzed using a 2-tailed t test (comparison of 2 treatment groups) and 1-way analysis of variance (comparison of 3 or more groups) followed by a Student t test for comparisons of means. A P value less than .05 was considered significant. All statistical analyses were carried out using JMP 7.0 software (SAS Institute Inc, Cary, North Carolina).
Results
Bacterial counts from both batches were similar, so data from both batches were collapsed for the analysis. Bacterial counts were uniform in each test condition, with only 6 being considered outliers (ie, values more than 2 standard deviations from the group mean). These outliers were excluded from analysis ( Table 1 ).
High levels of HI were adherent to the TTs after 7 days. Ciprofloxacin treatment dramatically reduced but did not eradicate all viable HI (P < .0001; Figure 1 ), consistent with functional criteria for biofilm formation. As noted above, counts were not done after ethylene oxide sterilization, as preliminary experiments demonstrated that this treatment uniformly eradicated all HI.

Haemophilus influenzae colony counts on fluoroplastic tympanostomy tubes with and without exposure to ciprofloxacin. Means are statistically significant between treatments (P = .0001). Error bars represent standard deviation.
High levels of PA were found on TTs after all prior exposures and treatments ( Figure 2 ). Treatment with gentamicin dramatically reduced PA counts, consistent with elimination of planktonic organisms. PA biofilm formation, as measured by viable PA colony-forming units after gentamicin exposure, was similar in TTs with prior HI exposure and gas sterilization or low-concentration ciprofloxacin exposure, suggesting that HI does not promote PA biofilm formation. High-concentration ciprofloxacin treatment after HI exposure resulted in lower PA counts (P = .002). HI was not isolated after exposure to either a low or high dose of ciprofloxacin, PA, and gentamicin.
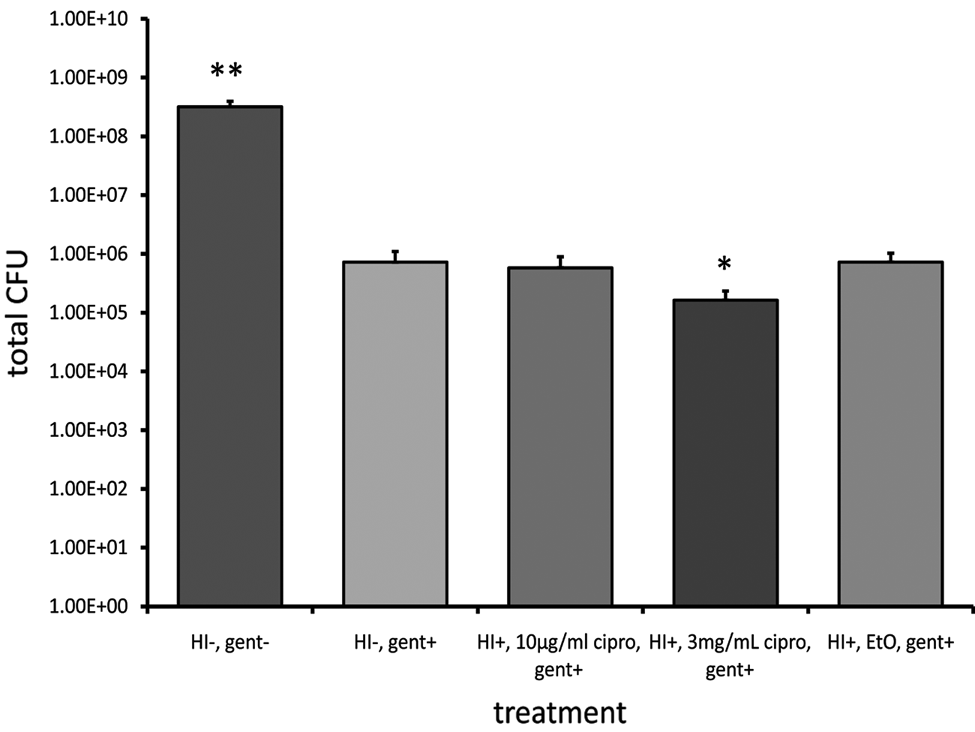
Pseudomonas aeruginosa (PA) colony counts on fluoroplastic tympanostomy tubes (TTs) with and without prior Haemophilus influenzae (HI) infection. PA counts were significantly** higher without gentamicin (gent) compared with all the other treatments (P = .0001). *Less PA biofilm formed on TTs with HI treated with 3 mg/mL ciprofloxacin (cipro; P = .002), whereas PA biofilm formation on TTs with prior HI biofilm and treated with 10 µg/mL ciprofloxacin or ethylene oxide (EtO) sterilization was not different than TTs without HI (P > .05). Error bars represent standard deviation.
Electron microscopy revealed bacteria in an extracellular matrix, typical of biofilms. The number of microbes seen after HI culture was, qualitatively, inversely dependent on the ciprofloxacin concentration ( Figure 3 ). Abundant cellular and extracellular material was seen after ethylene oxide sterilization ( Figure 3C ). TTs not treated with HI and gentamicin ( Figure 4A ) demonstrated the most robust PA biofilm. There were no qualitative differences in PA biofilm between the other treatment groups ( Figure 4B - D ). Abundant cellular and extracellular material was observed on TTs with HI treated with ethylene oxide gas and 200 µg/mL gentamicin ( Figure 4D ). Only PA and no HI was apparent on TTs after PA culture.
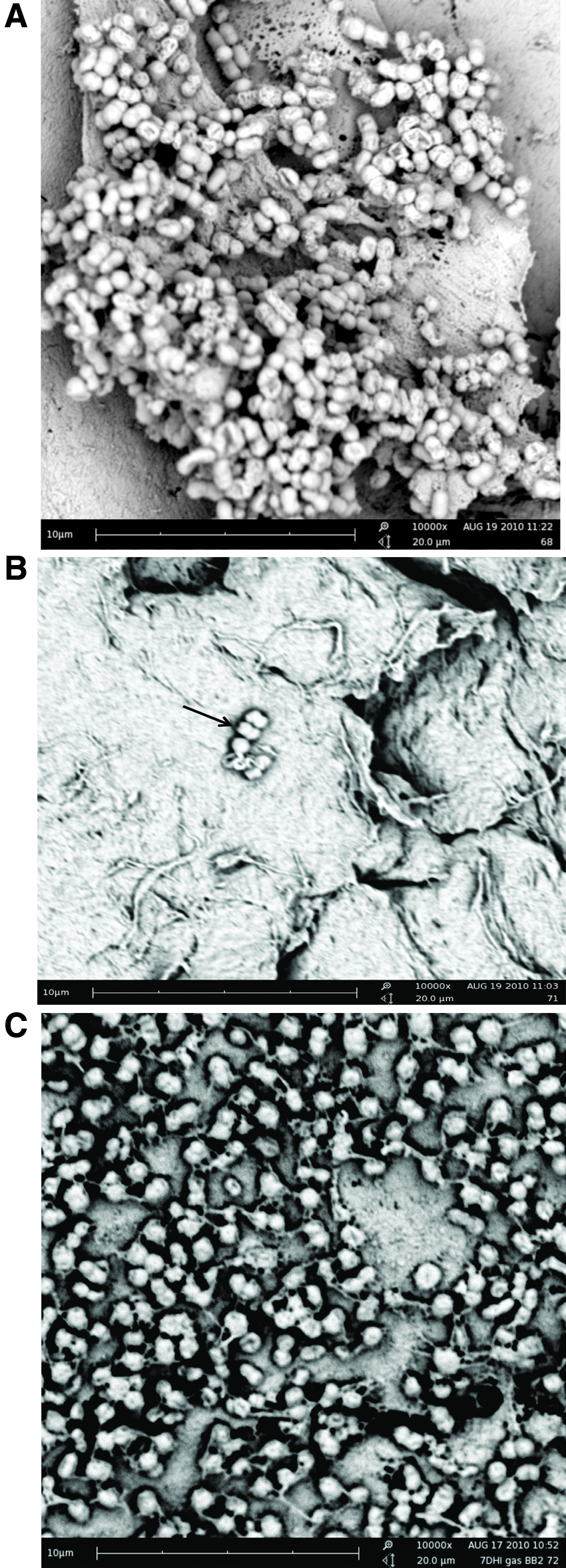
Scanning electron micrographs of tympanostomy tubes (TTs) after culture with Haemophilus influenzae (HI) and exposure to (A) no sterilization or antibiotic, (B) 3000 µg/mL ciprofloxacin, or (C) ethylene oxide sterilization. A thick mat of HI was observed in TTs not treated with ciprofloxacin (A), and very few HI were observed in TTs treated with 3000 µg/mL ciprofloxacin (B, arrows). Abundant cellular and extracellular material was seen after ethylene oxide sterilization (C).
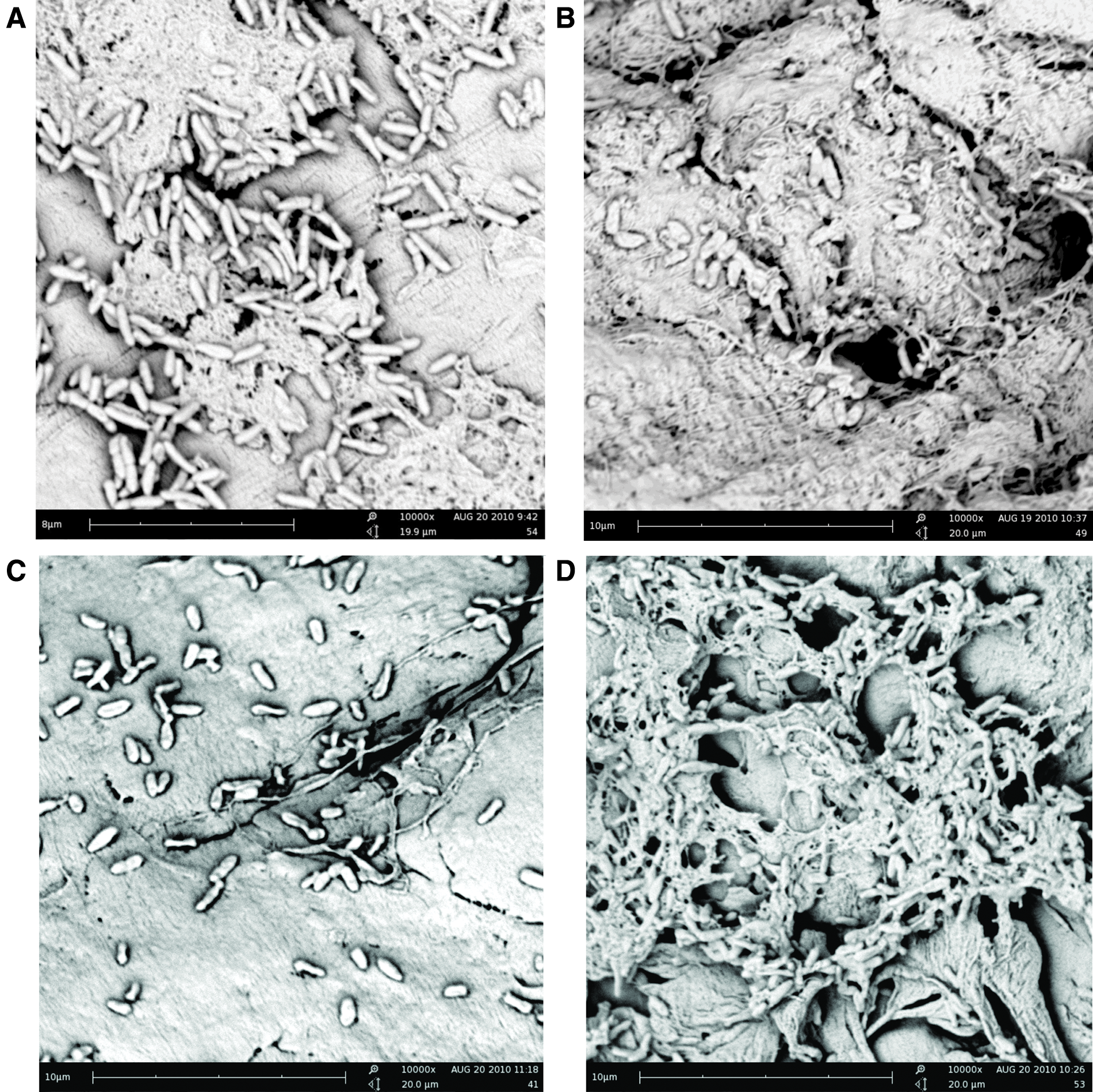
Scanning electron micrographs of tympanostomy tubes (TTs) after Pseudomonas aeruginosa (PA) culture and (A) no Haemophilus influenzae (HI; HI–), no gentamicin (gent; gent–); (B) no HI, 200 µg/mL gent; (C) HI treated with 3000 µg/mL, 200 µg/mL gent; and (D) HI treated with ethylene oxide gas (EtO), 200 µg/mL gent. TTs not treated with HI and gentamicin (A) showed the most robust PA biofilm. There were no qualitative differences in PA biofilm between the other treatment groups (B-D). Abundant cellular and extracellular material was observed on TTs with HI treated with ethylene oxide gas and 200 µg/mL gentamicin (D).
Discussion
Advancing age and prior antimicrobial treatment of post-TT otorrhea are associated with a transition from acute to chronic middle ear pathogens.4,12,13 Emergence of chronic middle ear pathogens is of concern because they are often associated with refractory disease, which may require parenteral antibiotic therapy or surgery.1,3,4
Biofilm formation is promoted by adherence of surface proteins, such as fibronectin from blood, 11 and surface irregularities. 14 HI biofilms may provide myriad additional binding sites to TT surfaces. 15 This was confirmed by our observations of significant debris remaining on TTs cultured with HI for 7 days and treated with ciprofloxacin or ethylene oxide gas sterilization. We hypothesized that debris from HI biofilm might promote biofilm formation by chronic middle ear pathogens, such as PA. In contrast, our observations suggest that this is not the case, at least in an in vitro system.
Numerous limitations of our model may, however, fail to reveal what is developing in children with recurrent otitis media. We studied a single strain of HI, only HI (ie, not Streptococcus pneumoniae), a single acute pathogen exposure, a single strain of PA, and did not expose TTs to the complex milieu (eg, neutrophils and other host responses) found in vivo. In a previous TT biofilm study, 16 we observed S pneumoniae and PA on TT surfaces by electron microscopy after exposure to both pathogens. In contrast, we observed no viable HI by bacterial counts or visually apparent HI by electron microscopy. The reason for this observation is unclear. PA growth may have dominated that of HI, preventing detection by standard culture and microscopy, as has previously been reported. 17 More sensitive techniques, such as polymerase chain reaction, may have demonstrated HI. 18 Our observations using polymerase chain reaction probes suggest that HI and PA commonly coexist on explanted TTs and ossicular prostheses (C. Ojano-Dirain, unpublished observations).
We expected to encounter more PA biofilm on TTs that had HI eradicated with ethylene oxide gas sterilization. This treatment did nothing to remove the HI from the TT surface. Interestingly, only highly concentrated ciprofloxacin treatment, akin to ototopical therapy, significantly reduced biofilm formation. Since PA formation on control TTs without HI exposure was not less than ethylene oxide or low-concentration ciprofloxacin–treated TTs, it is unlikely that this effect was mediated by biofilm. It is more likely that ciprofloxacin adhered to TTs and that the antimicrobial effect was carried forward to subsequent PA culture. This effect may be clinically meaningful. Intraoperative (TT placement) administration of a single dose of ototopical antibiotics has been shown to be effective in preventing post-TT otorrhea. 19 We have recently reported that a single dose of ototopical antibiotics can reduce bacterial growth on and around TTs in an in vitro model. 20 To our knowledge, such an effect (ie, avoidance of subsequent post-TT otorrhea) has not been reported with ototopical treatment of acute post-TT otorrhea.
Conclusions
HI biofilm does not promote PA biofilm formation on TTs. Use of high-dose ototopical therapy to clear HI infection may reduce subsequent PA biofilm formation. The clinical significance of this finding warrants examination.
Author Contributions
Disclosures
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Presented at the American Academy of Otolaryngology—Head and Neck Surgery Foundation Annual Meeting; September 26–29, 2010; Boston, Massachusetts.