
Abstract
Objective. To find the survival rate of patients ≥80 years old who undergo salvage surgery for squamous cell carcinoma of the larynx.
Study Design. National data registry analysis.
Setting. Seventeen population-based registries comprising the National Cancer Institute’s Surveillance, Epidemiology, and End Results database.
Subjects and Methods. Overall, cancer-specific, and relative survival rates were calculated from 1418 patients, stratified into 3 age cohorts, who underwent surgery following radiation therapy for treatment of laryngeal cancer.
Results. The 1-year overall survival of patients ≥80 years old (n = 57) was 76.1%. The cancer-specific survival at 1 year was 86.4%. These survival rates were significantly less than those of patients <65 years old (n = 869), who had a 1-year overall survival of 88.1% (P = .006) and cancer-specific survival of 90.5% (P = .029). Patients aged between 65 and 79 years old (n = 492) displayed 1-year overall survival of 80.7% (P = .426) and cancer-specific survival of 85.1% (P = .711), which were not significantly different from the ≥80 year cohort. When comparing relative survival at 5 years, the ≥80-year-old cohort’s survival trended the highest (≥80 years, 62.8%; 65-79 years, 51.3%; 20-64 years, 56.2%).
Conclusion. While patients ≥80 years old have a less favorable prognosis than patients <65 years old, the survival rates of patients ≥80 years old are not significantly different from the 65- to 79-year-old cohort. After controlling for non-cancer-related death, patients ≥80 years old appear to have similar 5-year survival outcomes compared with other patients.
Nonsurgical therapy with curative intent is currently used in more than 50% of cases of primary laryngeal cancer. 1 Conservative initial treatment has several advantages, including decreased rehabilitation time, improved voice function, and improved quality of life.2,3 By reserving surgery for residual or recurrent cancer, similar survival rates can be achieved both for patients who initially undergo surgery and for those who initially undergo radiotherapy.2,4 This approach is also gaining acceptance for use in advanced-stage laryngeal cancer as combined modality treatments use radiation and chemotherapy.
As the role of operative management in laryngeal cancer has shifted from primary treatment to salvage therapy, some studies have begun to examine what preoperative risk factors may affect outcomes in this specific previously treated patient population.4-7 Few studies have stratified survival rates within the elderly patient subset. While elderly patients undergoing head and neck surgeries have been shown to do well compared with elderly patients undergoing other surgical procedures, the typical complications prevalent in laryngectomy patients having previously received radiation may have a greater impact on the elderly population.8-10 Whether these radiotherapy-related factors affect the survival of elderly salvage surgery patients is an important question as the shifting demographics of the United States will result in an increase of the total elderly patient population and a significantly larger proportion of patients >70 and >80 years old. 11 A single-institution retrospective review would likely not be able to answer this question, as recurrences of laryngeal cancer are relatively rare, with early-stage tumors recurring in 5% to 40% of patients.2,7,12-14 The number of potential cases is likely further reduced by the decision of patients, family members, and physicians to opt for palliative care as an alternative to surgery.
Access to the Surveillance, Epidemiology, and End Results Program (SEER) enabled us to obtain a large number of elderly patients to achieve increased power for this study. The SEER program is a federally sponsored national registry that links epidemiologic cancer data with population demographics, initial therapies, and patient survival. This database is updated annually and allowed review of records from various regions within the United States from 1973 to 2007. 15
The objective of this study was to review available data on the short-term survival of elderly patients who undergo salvage surgery for recurrent laryngeal cancer, particularly at the 1- and 5-year interval. Although patient history was limited, demographic information, cancer stage, cancer subsite, and other available data were analyzed for comparison between elderly salvage surgery patients and salvage surgery patients of all ages.
Methods
The authors consulted the Biomedical Institutional Review Board (IRB) at Saint Louis University and confirmed that this study would not meet the definition of human subjects research and therefore would not require IRB oversight. Salvage surgery cases for laryngeal cancer recurrences from 1973 to 2007 were extracted from the SEER database (November 2009). These cases were defined by the International Classification of Disease for Oncology, Third Edition (ICD-O 3), site codes glottis (C32.0), supraglottis (C32.1), subglottis (C32.2), laryngeal cartilage (C32.3), overlapping lesion of larynx (C32.8), larynx not other specified (NOS) (C32.9), anterior surface of epiglottis (C10.1), and by therapy sequence “radiation prior to surgery.” This distinction was felt to be specific for salvage surgery cases since initial treatment with combined modality approaches has not included the use of radiation as induction or neoadjuvant therapy prior to surgery. Three patient cohorts based on age at diagnosis (<65, 65-79, and ≥80 years old) were created and used for comparison.
Stage, year of cancer diagnosis, and tumor subsite were extracted for comparison between the 3 groups. The SEER database uses both the American Joint Committee on Cancer staging system and its own summary staging system to classify extent of disease. Patient cases are classified to both recent and historic staging systems in SEER to facilitate comparison of cases across time. For laryngeal cancer, however, no single staging system was used for every case, so the staging systems covering the longest period of time were used, those being the summary staging systems labeled “SEER historic stage A (1973-1997)” and “Summary Stage 2000 (1998-2007).” Each case was labeled as local, regional, or distant according to the laryngeal site definition, which varied slightly between the 2 classification systems. To simplify comparison with respect to year of diagnosis, each case was assigned to a corresponding time period (1973-1985, 1986-1996, 1997-2007). For tumor subsite comparisons, anterior epiglottis was combined with supraglottis, and the tumor sites labeled laryngeal cartilage, overlapping lesion, and larynx NOS were combined into the category labeled other. Other data extracted include patient age, sex, race, type of laryngectomy (partial vs total), last recorded vital status, months of survival, cause of death, and extent of primary disease. Demographic data as well as both pre-1998 and post-1997 stage, time period of diagnosis, and tumor site were compared by age of diagnosis.
For each age cohort, overall and cancer-specific survival (CSS) were calculated at 1-year intervals, and values were tabulated up to 5 years. A Kaplan-Meier survival analysis was performed with respect to age using SAS version 9.2 (SAS Institute, Cary, North Carolina). One-year, 5-year, and total survivals were compared between each cohort using log-rank tests with a significance level of .05. Using the SEERstat program survival session, relative survival was also calculated for each cohort at 1-year intervals up to 5 years. SEERstat estimated relative survival by calculating the ratio of overall survival to “effective survival” based on expected life tables for the general population, matched to the age, gender, and racial breakdown of our selected cohort. Last, Cox proportional hazards models were created to look for predictors of overall survival and CSS. To evaluate the effect of staging accurately, the sample was split up between cases diagnosed prior to 1998 and after 1997 so that the corresponding staging system, “SEER historic stage A (1973-1997)” or “Summary Stage 2000 (1998-2007),” could be incorporated into each model. Results for each run were analyzed, and predictive value was determined with significance set at P < .05.
A comprehensive review of the literature was conducted of the PubMed database for published papers, using the search terms laryngeal neoplasm AND salvage therapy. The returned articles were studied for survival rates following salvage surgery for laryngeal cancer recurrences. The bibliographies of these articles were then examined for similar studies. If other cancers or other therapies were grouped with the laryngeal salvage surgery cases, then these articles were excluded. Articles were also excluded if patients’ ages were not given or if patients received endoscopic laryngeal laser surgery for salvage. Type of salvage procedure performed, cancer site, stage breakdown, survival (particularly overall and cancer specific), and ages for patients were recorded (see online
Results
A total of 1418 patients met the inclusion criteria, composed of 57 patients 80 years or older, 492 patients between 65 and 79 years old, and 869 patients 64 years of age or younger. There were 276 (19.5%) female patients and 1142 (80.5%) male patients. The median age for each of the 3 age groups was 56 years for the <65 cohort, 70 years for the 65-79 cohort, and 82 years for the ≥80 cohort.
Table 1 shows the comparison between the 3 age cohorts in terms of stage, site, and time period in which the patients were diagnosed. The ≥80 cohort differed significantly from the <65 and 65-79 cohort, considerably regarding stage and tumor subsite. Patients 80 years and older tended to have less advanced staged cancer, and the laryngeal subsite was more likely to be glottic compared with patients <65 and 65 to 79 years. The time period during which the cancers were diagnosed varied significantly as well.
Comparison of Patient and Tumor Characteristics by Age (N = 1418) a
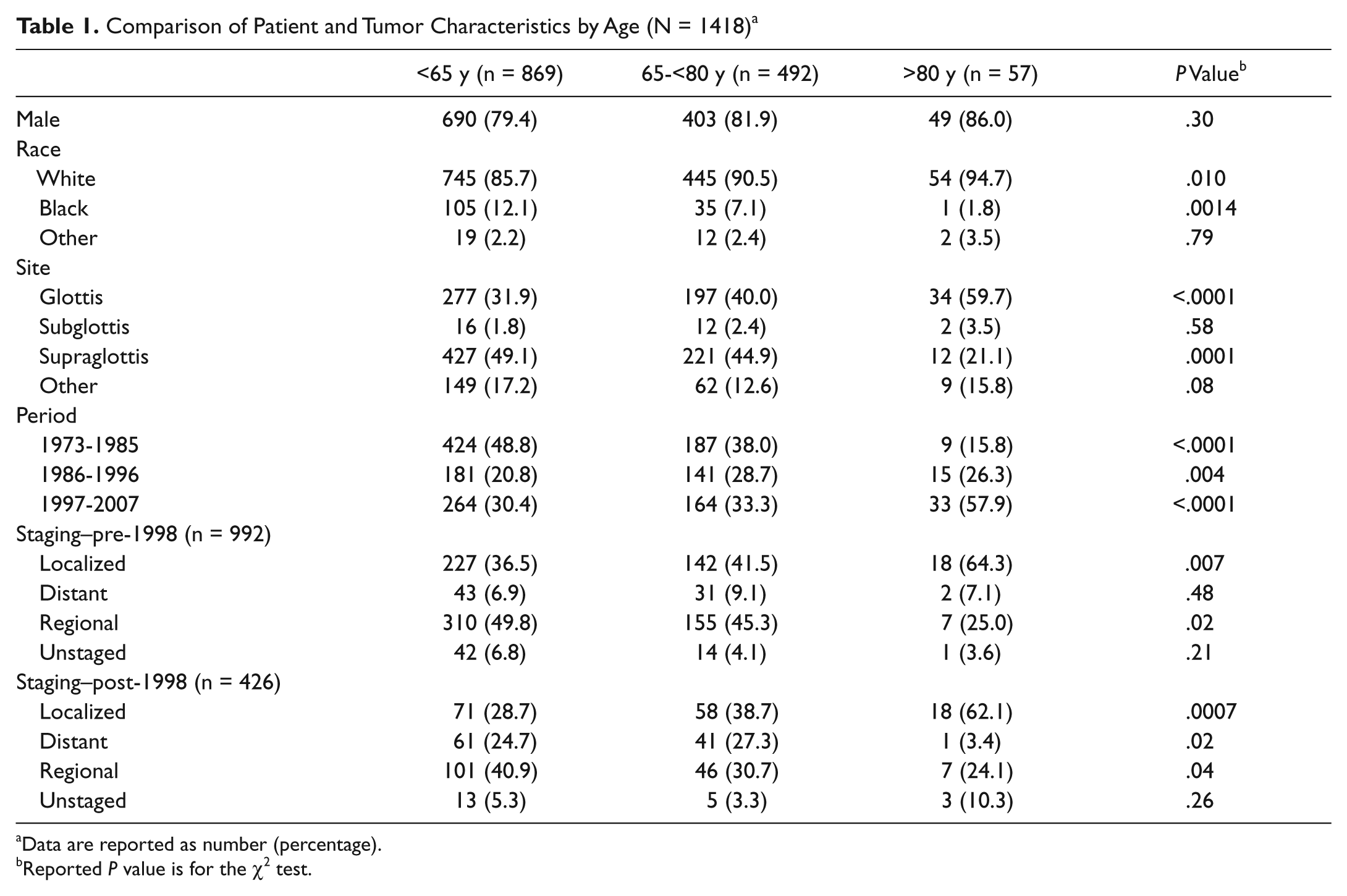
Data are reported as number (percentage).
Reported P value is for the χ2 test.
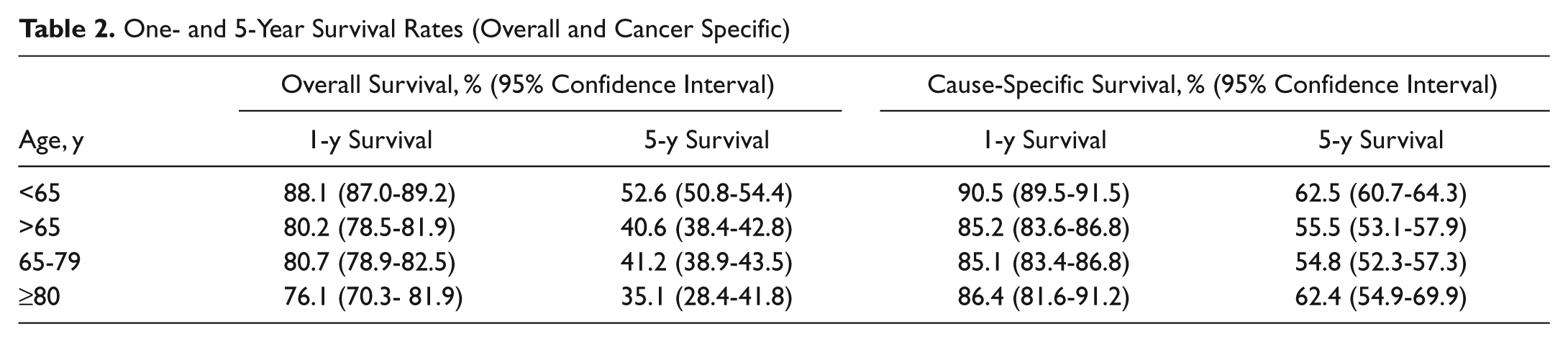
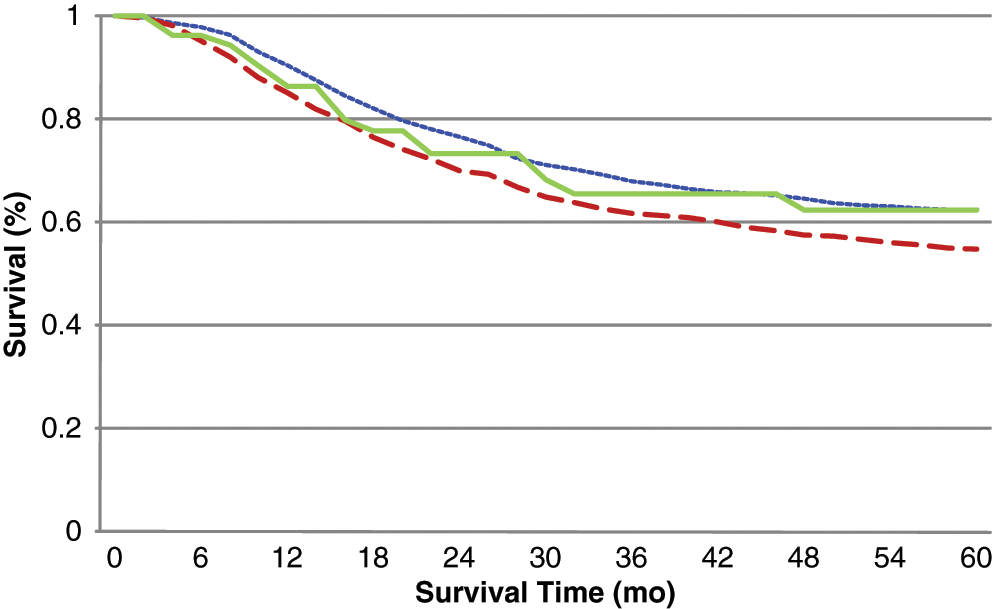
The overall 1-year survival of patients ≥80 years was 76.1%. The 1-year CSS and relative survival rates were 86.4% and 86.5%, respectively. One-year overall and CSS rates were less than those from patients in the youngest age group (<65 years), which had a 1-year overall survival of 88.1% (P = .006) and CSS of 90.5% (P = .029). As shown in Table 2 , the 5-year survival rates were similarly lower. For patients from the ages of 65 to 79 years, the 1- and 5-year survival rates trended higher in terms of overall survival compared with patients ≥80 years, at 80.7% (P = .426) and 41.2% (P = .399), respectively, although they were not significantly different. The 1- and 5-year CSS for the ≥80 cohort were also not significantly different from the 65-79 cohort (P = .711 and P = .88, respectively) and did not show any trends toward higher survival ( Tables 2 and 3 ). Figures 1 and 2 show these data in a Kaplan-Meier graph comparing all 3 age groups’ survival over 5 years.
One- and 5-Year Survival Rates (Overall and Cancer Specific)
P Values for Overall and Cancer-Specific Survival Comparisons between Age Groups a
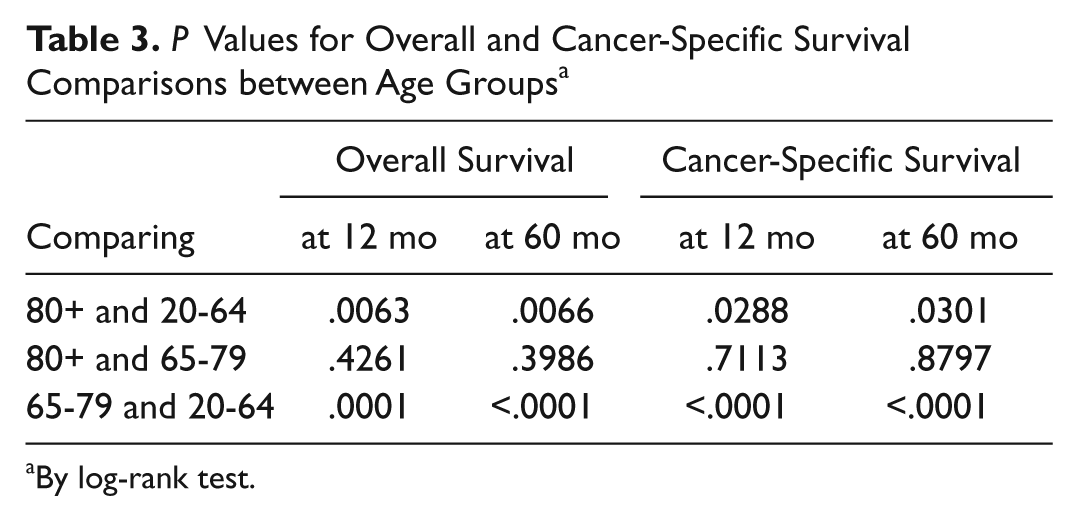
By log-rank test.
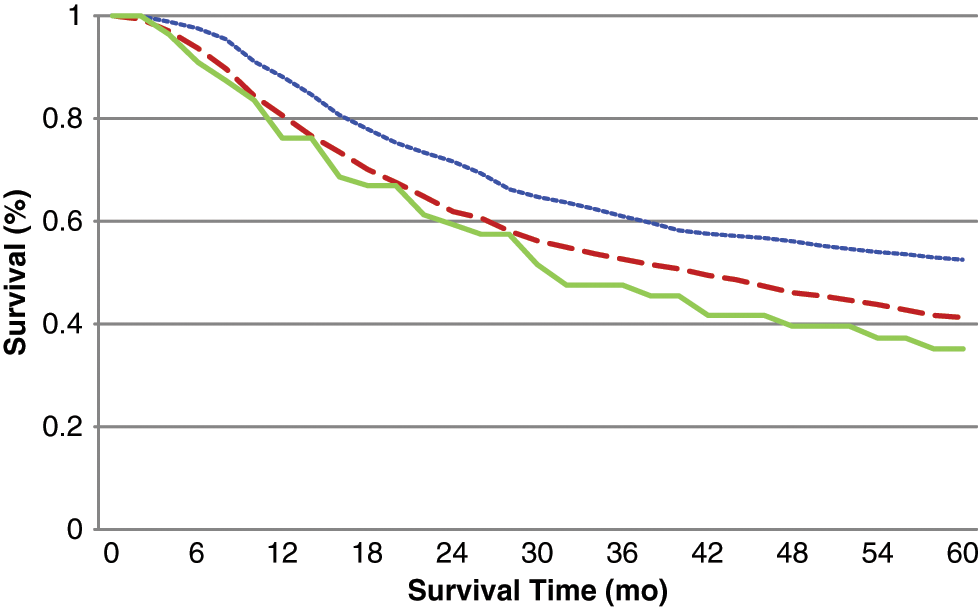
Kaplan-Meier graph of overall survival stratified into 3 age groups. Overall P values, calculated by log-rank test, were (a) <65 versus 65-79 (P < .0001), (b) <65 versus ≥80 (P = .0003), and (c) 65-79 versus ≥80 (P = .2203). Short dashed line indicates age <65 years; long dashed line indicates age 65 to 79 years; solid line indicates age ≥80 years.
Kaplan-Meier graph of cancer-specific survival stratified into 3 age groups. Overall P values, calculated by log-rank test, were (a) <65 versus 65-79 (P < .0001), (b) <65 versus ≥80 (P = .15), and (c) 65-79 versus ≥80 (P = .73). Short dashed line indicates age <65 years; long dashed line indicates age 65 to 79 years; solid line indicates age ≥80 years.
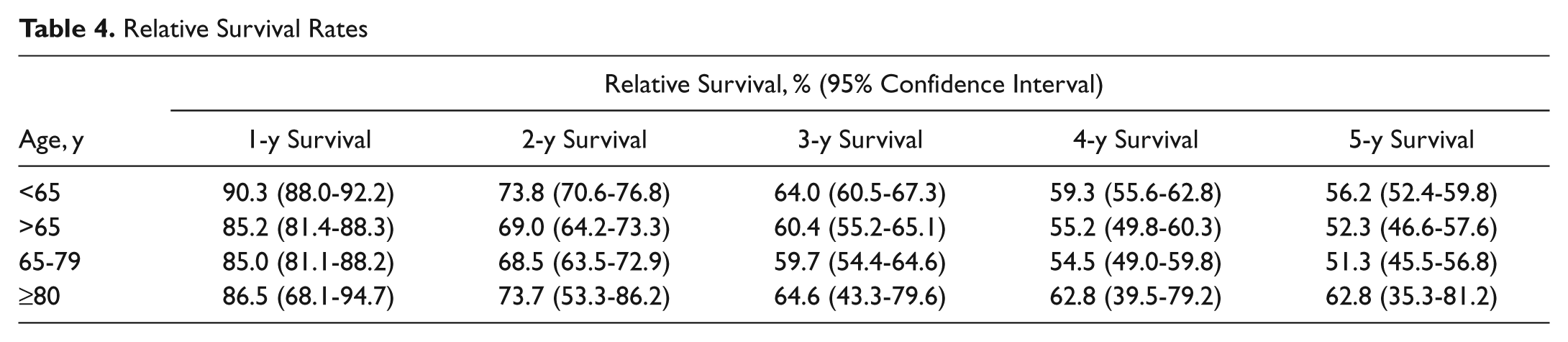
When comparing relative survival, the ≥80 cohort demonstrated nearly identical 1-year survival to the 65-79 cohort. When comparing relative survival at 5 years, the ≥80 cohort demonstrated a trend toward the highest survival rate compared with the younger cohorts (62.8% for the ≥80 cohort vs 51.3% for the 65-79 cohort vs 56.2% for the 20-64 cohort). Statistical significance could not be calculated for relative survival as raw survival data from the demographically matched life expectancy tables were not available ( Table 4 ).
Relative Survival Rates
Figures 3 and 4 show a Kaplan-Meier graph comparing the <65-year-old cohort and the 2 older cohorts combined (≥65 years) for overall and CSS.
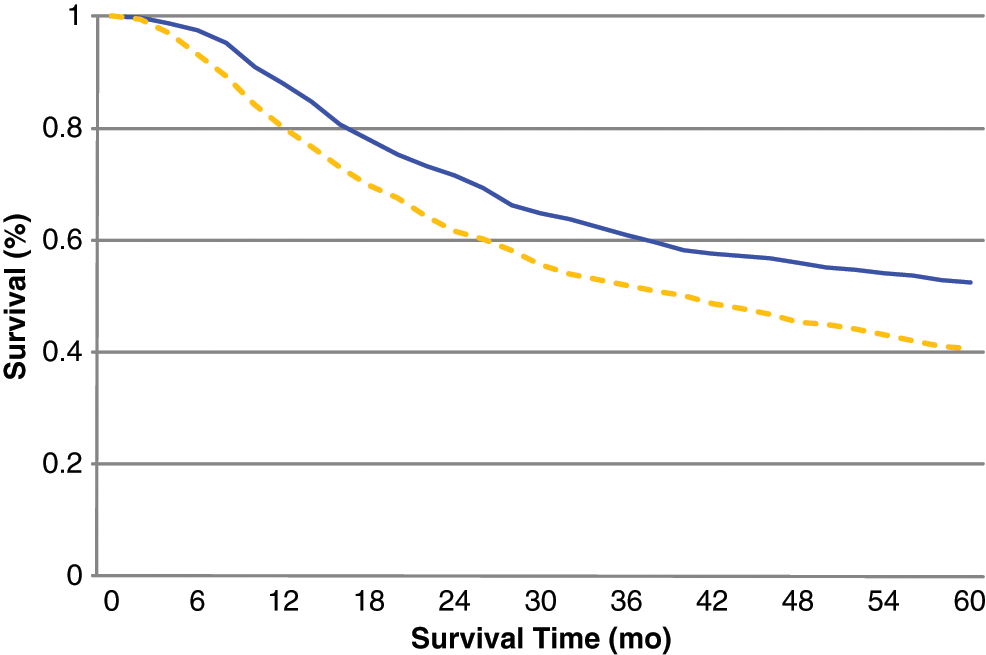
Kaplan-Meier graph of overall survival stratified into 2 age groups. Overall P value was <.0001, calculated by log-rank test. Solid line indicates age <65 years; dashed line indicates age ≥65 years.
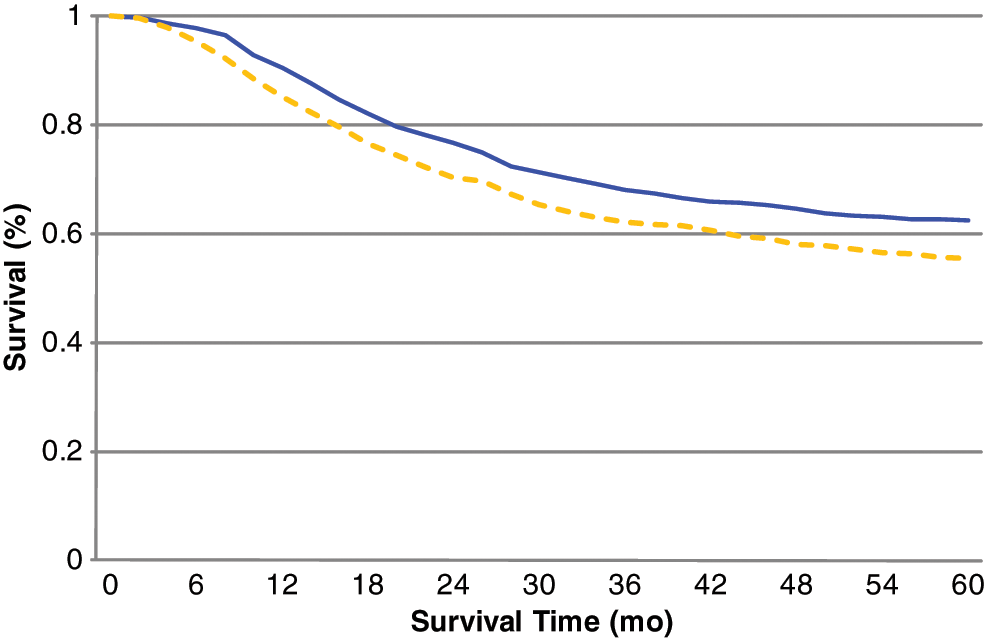
Kaplan-Meier graph of cancer-specific survival stratified into 2 age groups. Overall P value was <.0001, calculated by log-rank test. Solid line indicates age <65 years; dashed line indictes age ≥65 years.
When looking at CSS across the entire sample (controlling for all variables except stage), age between 65 and 79 years and site other than glottic cancer predicted worse survival. These variables continued to predict worse survival when controlled for stage in the pre-1998 group. However, neither age nor site predicted worse survival in the post-1997 age group. Advanced stage predicted worse survival in all age groups. The results of the Cox proportional hazards model, comparing the predictive value of variables for overall and CSS, can be seen in Tables 5 and 6 .
Hazard Ratios for Cancer-Specific Death and for All-Cause Death, 1973-2007 (N = 1418)
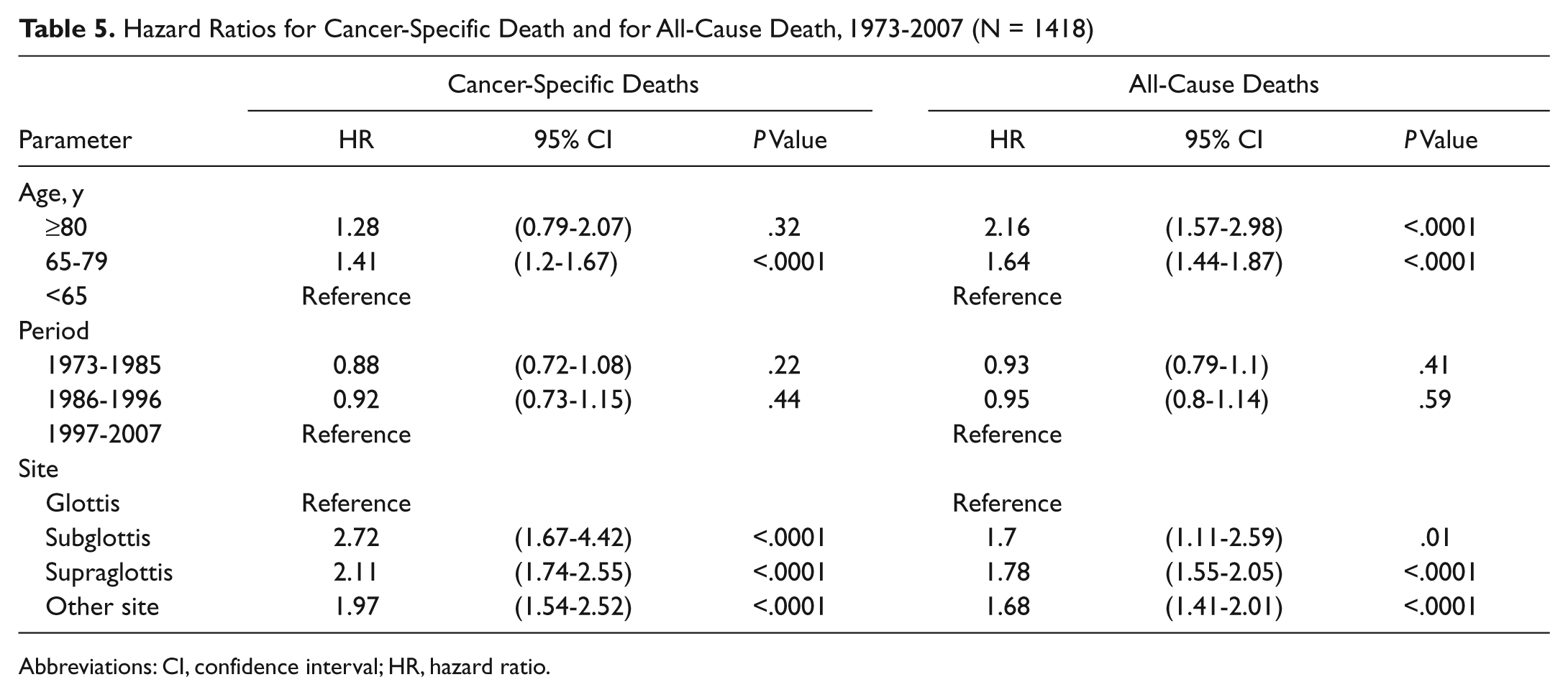
Abbreviations: CI, confidence interval; HR, hazard ratio.
Hazard Ratios for Cancer-Specific Death and for All-Cause Death (Including Hazard Ratio for Stage) a
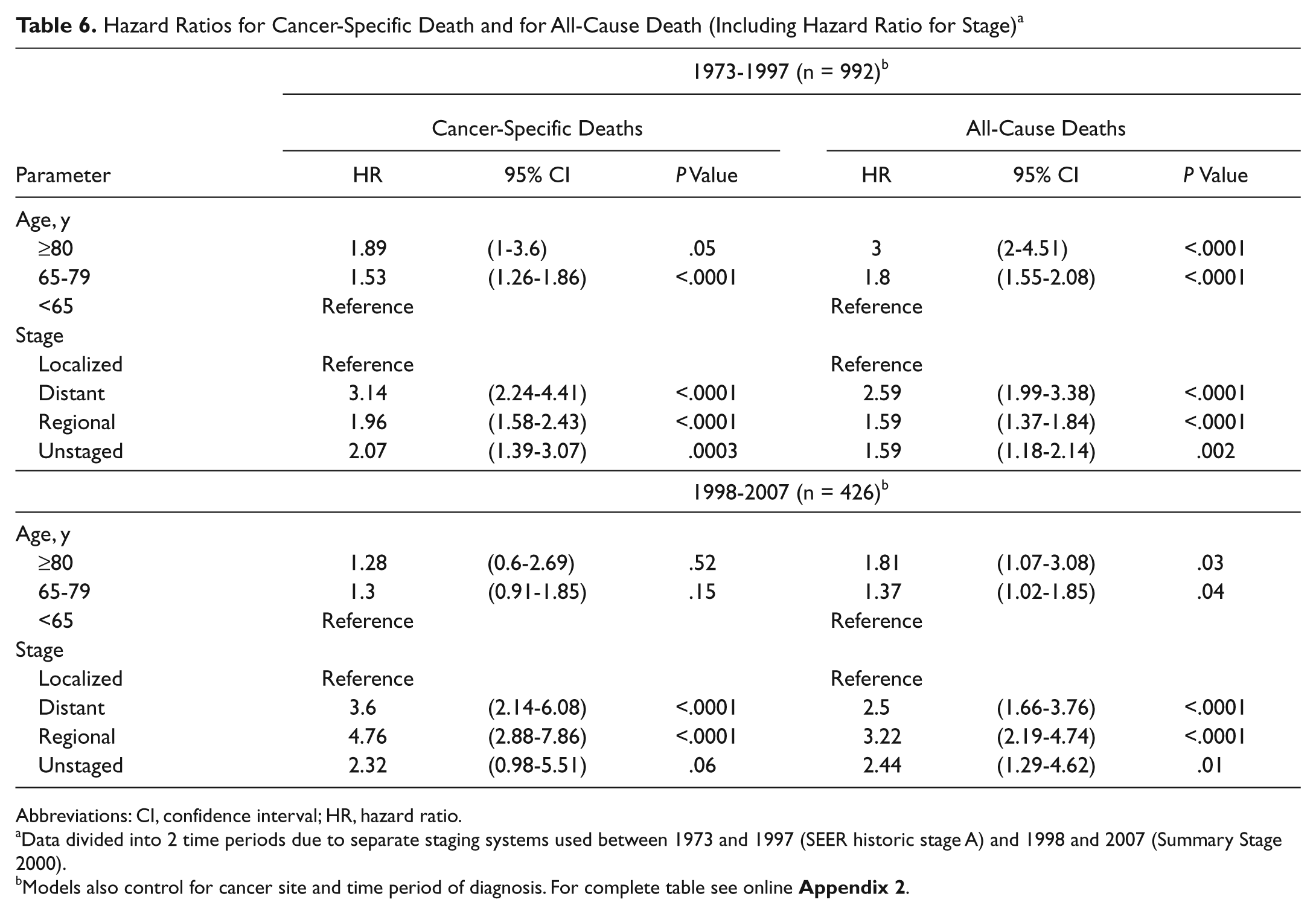
Abbreviations: CI, confidence interval; HR, hazard ratio.
Data divided into 2 time periods due to separate staging systems used between 1973 and 1997 (SEER historic stage A) and 1998 and 2007 (Summary Stage 2000).
Models also control for cancer site and time period of diagnosis. For complete table see online
A post hoc power analysis was performed for all-cause mortality and cancer-specific mortality with age as the primary regressor. Given the sample size we obtained through SEER, which included all possible patients who met our inclusion and exclusion criteria, we obtained 100% and 94% power, respectively.
Discussion
Laryngeal cancer is the most common cancer of the head and neck, representing approximately 20 000 cases per year in the United States. 16 Laryngeal anatomy can often facilitate resection with complete margins, and complex reconstruction is not often required, especially compared with tumor resections from other areas of the head and neck. However, the significant rehabilitation necessary for recovery from laryngeal surgery and the perceived and actual deficits in voice quality and deglutition do make a nonsurgical treatment option more favorable to patients. 17 This trend may be even more pronounced in the elderly patient populations as seen from aggregate data reported by cancer centers represented in the National Cancer Database (NCDB) database. Radiation therapy alone is used in a greater proportion of patients for initial treatment of laryngeal cancer as age increases, from 26% of patients aged 50 to 59 years to 38% of patients aged 80 to 89 years. 1
As a consequence of this trend in initial therapy and the shifting population demographic, it is likely salvage laryngectomy will be increasingly considered for treatment of radiation failure in elderly patients, particularly in those older than 70 and 80 years. While some studies have shown that age does predict worse survival for this treatment group, 4 other studies have not shown this relationship.5,7 Our study, using the patients from the SEER research database, does indicate that salvage surgery patients ≥65 years have significantly worse survival, both in terms of overall survival and CSS. This likely occurs for a combination of reasons but may be due especially to the comorbidities frequently associated with these patients. Similar to patients with other aerodigestive tumors, laryngeal cancer patients have an extremely high incidence of respiratory and cardiovascular disease secondary to the mutual risk factors of smoking and alcohol abuse.8,18,19 Not only is the damage on the respiratory and cardiovascular system cumulative with time, the burden of diseases such as chronic obstructive pulmonary disease and congestive heart failure is often greater in elderly patients, who have decreased physiologic reserve by which to compensate. 20
However, this worse survival does not preclude these patients from consideration for surgery without appropriate preoperative evaluation. Despite commonly poor patient health profiles, overall, head and neck surgery patients have the same mortality as moderate-risk general surgery patients. 19 Also, the surgical complications that typically have a strong association with mortality in elderly patients, such as sepsis and acute renal failure, are not typically experienced by patients who undergo laryngectomy.8,20
One of the main points of our study was to examine the elderly population subset, comparing the survival of the very elderly to the “younger” elderly population to see if the correlation between increased age and worse prognosis was maintained. This relationship appeared to occur for the overall survival curves, with 1- and 5-year survival appearing to be increasingly worse for the older age group (although no significant difference was found between the 65-79 cohort and the ≥80 cohort.) This relationship was not apparent for CSS and relative survival, where the 1-year survival rates were almost identical and the 5-year survival appeared better for the ≥80 age group compared with the 65-79 cohort (although again not significantly different). Interestingly, when comparing the relative survival at 5 years, the ≥80 cohort had the best survival of all age cohorts, including against the 20- to 64-year-old group.
One of the initial explanations for the favorable survival of patients ≥80 years old is that the patients selected for surgery likely have cancers that are of less advanced stage and are generally less invasive. This explanation was found to be accurate in that patients in this very elderly age group did have a larger proportion of early-stage cancers as well as a higher proportion of cancer staged from the glottis subsite, typically portending toward a better prognosis. 21 However, when staging and site were controlled, age ≥80 years did not have a negative impact on CSS. Another factor may likely be the motivation and overall health of this particular group of patients 80 years and older. Of note, Arriaga et al 8 mentions that some elderly patients actually improve their overall health following a total laryngectomy as a result of the eliminated risk of aspiration and associated complications such as pneumonia and hypoxia-induced arrhythmias.
The time period of diagnosis was also considered to be a potential confounding factor as the various treatment modalities have evolved greatly over the past 30 years. A much larger proportion of the ≥80 cohort underwent treatment in the most recent time period (1997-2007) compared with the other aged cohorts. One would suspect that new technologies such as intensity-modulated radiotherapy and advanced surgical reconstructive techniques may have positively influenced this group’s survival. Recent observational studies, however, show this assumption to be inaccurate as survival for laryngeal cancer at various stages has either decreased or remained stable over the past 30 years, even when stratifying among treatment modalities.18,22 While these treatment advances have reduced morbidity from radiation side effects and postoperative fistulas, they appear unlikely to influence short-term survival.
It is hoped that this study will better inform and guide the counsel of patients and family when deciding whether or not to pursue salvage surgery. This is the first study to look at outcomes specifically for patients older than 80 years who undergo salvage surgery. We hope this study will warrant further research directed toward what factors can help better predict which elderly patients would benefit from surgery following failed radiation treatment. Factors specific to salvage surgery that have been suggested to predict worse outcomes other than age include clinical T stage of recurrent tumor, positive surgical margins at the site of recurrence, pathologic node status, and whether there is regional or local recurrence.4-6
One initial concern in conducting this study was achieving a large enough sample size to accurately assess the survival of the ≥80 age group. As with any study limited by sample size, the lack of statistical significance may be more easily attributed to insufficient power and may not necessarily indicate that the survival outcomes of 2 populations are similar. However, by using the SEER database, this sample of salvage surgery patients is the largest studied to date. The Commission on Cancer’s NCDB offers a much larger group of patients to be studied, but this database was not amenable for use in this study as it does not record data on any secondary therapy following primary treatment.
Another potential limitation was that the definition used to extract salvage surgery cases may have also included patients who received surgery without the purpose of salvage or who received salvage surgery for only regional or distant metastases. Surgery-specific codes, indicating laryngectomy versus neck dissection versus local excision, were extracted from SEER when available; however, a substantial number of cases did not include this information. Prior to 1988, no site-specific codes existed for laryngeal cancer, and the coding definitions continued to evolve up until 2003. While the potential for error should be acknowledged, the likelihood of a recurrent laryngeal cancer requiring a neck dissection for regional recurrence without surgery at the primary site for local recurrence would be small. In one recent study by Johansen et al, 23 regional recurrence alone occurred in <8% of 274 cases of recurrent glottic carcinoma following radiation therapy.
As the use of national data registries has become more common, including several longitudinal studies regarding survival outcomes in laryngeal cancer,18,22,24 evaluation of the reliability and consistency of data from these databases continues to be critical. Patient cases recorded in SEER and the NCDB are collected from multiple registries across the United States and span decades. SEER uses a number of quality control tools including reliability studies, requiring each hospital registry to code de-identified control cases, which are then reconciled to identify discrepancies in coding. The use of these studies to revise coding manuals and improve training for registrars should continue to improve the uniformity of data from various regional registries. Unfortunately, similar control mechanisms do not currently exist for comparing or combining case data across time. For this reason, we chose to control for time period of diagnosis (as well as stage and site) when determining odds ratios for each age cohort.
Conclusion
Elderly patients do have worse survival than younger patients do, both for overall survival and CSS. However, very elderly patients, those 80 years and older, who have favorable tumor-related prognostic indicators do well compared with other age groups. Future studies should look at the role in which specific patient characteristics influence this age group’s survival.
Author Contributions
Disclosures
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
This article was presented at the American Head and Neck Society 2010 Research Workshop on Biology, Prevention, & Treatment of Head and Neck Cancer; October 29, 2010; Arlington, Virginia.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.