
Abstract
In the past several years, food allergies have taken center stage in the media and have become a topic of great concern for our patients and their families. Whether or not this is due to a rise in the prevalence of food allergies or just a heightened awareness, it is our responsibility as clinicians and scientists to critically analyze the current evidence available concerning the epidemiology, manifestations, diagnosis, and management of this disease. In 2010, the National Institute of Allergy and Infectious Diseases (NIAID) published guidelines concerning the diagnosis and management of food allergies. Since 2009, the Allergy, Asthma and Immunology Committee of the American Academy of Otolaryngology—Head and Neck Surgery has sponsored a miniseminar titled, “Food Allergy: State of the Science.” This commentary focuses on the highlights from the 2010 meeting and provides some thoughts on what this latest publication means to otolaryngologists.
Epidemiology of Food Allergies
During the course of development, it is necessary for humans to achieve immunologic tolerance to the foods they are consuming. In certain predisposed individuals, this process breaks down, and this leads to sensitization to a food protein. Sensitization begins early in life, and the risk of developing food allergies is higher in children with a history of asthma, eczema, or allergic rhinitis. 1 The Centers for Disease Control and Prevention estimates the prevalence of food allergy in children younger than 18 years in the United States to be 3.9%, which represents an 18% increase from 1997 to 2007. 2 The majority of children will outgrow their food allergies to cow’s milk, corn, wheat, and soybean, but sensitivities to fish, shellfish, tree nuts, and peanuts are more likely to persist into adulthood ( Table 1 ). 3
Natural History of Food Allergy and Cross-Reactivity between Common Food Allergies 3
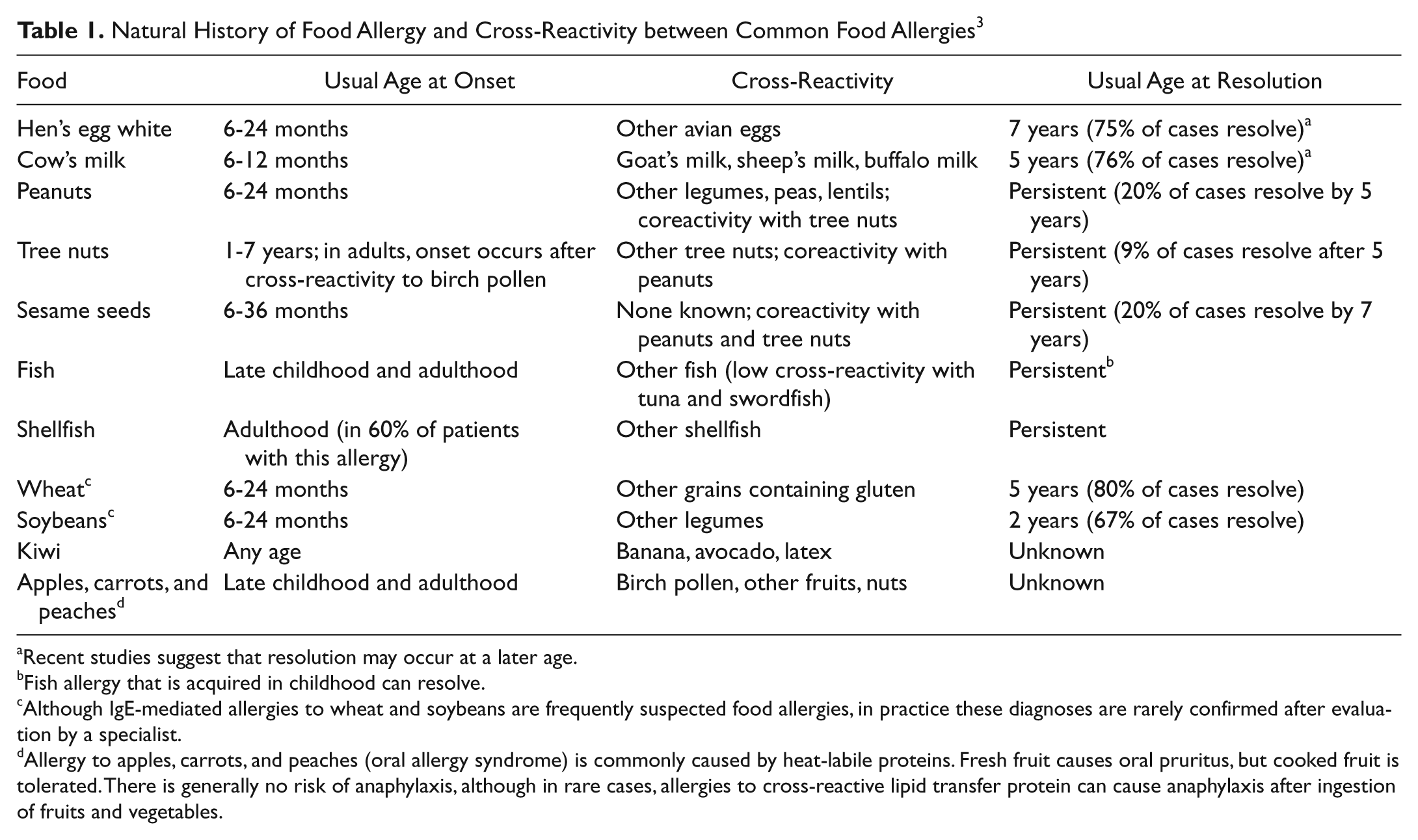
Recent studies suggest that resolution may occur at a later age.
Fish allergy that is acquired in childhood can resolve.
Although IgE-mediated allergies to wheat and soybeans are frequently suspected food allergies, in practice these diagnoses are rarely confirmed after evaluation by a specialist.
Allergy to apples, carrots, and peaches (oral allergy syndrome) is commonly caused by heat-labile proteins. Fresh fruit causes oral pruritus, but cooked fruit is tolerated. There is generally no risk of anaphylaxis, although in rare cases, allergies to cross-reactive lipid transfer protein can cause anaphylaxis after ingestion of fruits and vegetables.
Ear, Nose, and Throat Manifestations of Food Allergies
Type I, IgE-mediated, hypersensitivity reactions tend to be rapid in onset and severe in nature. When exposed to an antigen, IgE bound to mast cells becomes cross-linked, leading to cell degranulation with the release of histamine and other preformed mediators. The early physiologic response includes increased vascular permeability, vasodilation, smooth muscle contraction, and stimulation of the mucous glands. The late-phase response includes tissue edema and the attraction of an inflammatory cell infiltrate. Examples of IgE-mediated reactions include food-induced anaphylaxis, acute urticaria from food that is contacted or ingested, and oral allergy syndrome (OAS), which is a localized IgE-mediated allergy causing itching, tingling, or burning of the oral cavity when raw fruits and vegetables cross-react with the shared epitopes of airborne allergens.
Non-IgE-mediated reactions are also known to occur in response to foods, but the percentage is unknown. Food protein–induced enterocolitis syndrome (FPIES) is a severe, systemic response to a food protein, mediated by a cytotoxic, Gell and Coombs type II reaction, which may cause failure to thrive in infants. Food protein–induced allergic proctocolitis is a transient disease, usually caused by cow’s milk, human breast milk, or soy, which resolves within the first 1 to 2 years of life. Heiner syndrome, or food-induced pulmonary hemosiderosis, is a rare disease affecting infants and young children that is typically associated with hypersensitivity to cow’s milk proteins. Clarifying the natural history of non-IgE-mediated reactions was identified by the National Institute of Allergy and Infectious Diseases (NIAID) as a gap in knowledge. 4
Mixed IgE and non-IgE-mediated reactions may also result from the ingestion of foods. Eosinophilic esophagitis is a chronic inflammatory condition that is most common in infants, children, and adolescents, producing feeding disorders, abdominal pain, failure to thrive, irritability, vomiting, and food refusal. In adults and adolescents, clinical symptoms include esophageal food impactions, abdominal pain, and dysphagia. Atopic dermatitis is the first manifestation in the allergic march with a peak onset normally before 3 months of life. Eighty-five percent of patients with atopic dermatitis are sensitized to food and inhalant allergens, and up to 37% of children younger than age 5 years with moderate to severe atopic dermatitis will have IgE-mediated food allergy. 5
Another important gap in knowledge concerns the manifestations of food allergies in the airway, particularly the upper airway. Up to half of asthmatics have IgE-mediated food allergies. The coexistence of food allergies in patients with asthma may be a risk factor for severe exacerbations of asthma. Asthmatic patients with food allergies are more likely than asthmatic patients without food allergies to require emergency room visits and hospitalizations for asthma. 6 However, a Th2 cytokine pattern has also been found in both middle ear effusions and nasopharynx tissue in atopic patients, and a strong association has been found between food allergies and Ménière disease.7,8
Diagnosis of Food Allergies
Skin prick testing (SPT) is a rapid and safe means to determine sensitization to an antigen, whereby allergenic extract or raw fruits and vegetables are introduced into the epidermis of the patient. A negative SPT response is usually interpreted as confirming the absence of IgE-mediated sensitivity (negative predictive value of >90%). However, it must be kept in mind that only about 50% of patients with a positive SPT have a clinically relevant sensitivity to the food identified. The optimal skin test for detecting non-IgE-mediated reactions remains unclear.
In vitro testing may be of particular benefit for those patients who have a history of a life-threatening reaction to the suspected food or for those patients who cannot be skin tested. But like SPT, a positive in vitro test only indicates sensitization to a particular food and may not correlate with clinical disease. Studies suggest that the absolute levels of antigen-specific IgE antibodies (sIgE) may directly correlate with the likelihood of clinical reactivity when compared with oral food challenge results, but it must be kept in mind that undetectable sIgE levels occasionally occur in patients with IgE-mediated food allergy.
Microarray, or component-resolved testing, focuses on the levels of certain proteins or segments of proteins (epitopes) in foods to which IgE binding correlates with a high risk for clinical reactions. For nonsevere reactions, heat-labile proteins may easily be denatured prior to the consumption of the food. The goal is to develop a diagnostic test with an accuracy that approaches that of the double-blind, placebo-controlled food challenge test. Component-resolved testing may also be useful in the diagnosis of oral allergy syndrome and in helping determine which antigens should be included in the immunotherapy treatment vial.
Office-supervised food challenges may be performed when the diagnosis of food allergies remains uncertain even after careful evaluation, using the clinical history and available testing. There is currently no standardized protocol for performing or interpreting oral food challenges, but it involves completely removing the suspected foods from the diet for a prescribed period of time, and then, under medical supervision, the food or a placebo in a neutral form (no texture, smell, or taste clues) is reintroduced in gradually increasing amounts while the patient is monitored for signs of an allergic reaction. Trial elimination diets are also useful, having the advantage of being simultaneously diagnostic as well as therapeutic, but the risk of placebo effect is high.
The NIAID guidelines discourage the use of the basophil histamine release/activation, lymphocyte stimulation, endoscopic allergen provocation, provocation/neutralization, cytotoxic assays, and allergen-specific IgG and IgG4 testing. At this time, these tests lack standardization and have low quality of evidence. Intradermal skin testing for the diagnosis of food allergy is also not recommended because insufficient evidence exists to support its use and because the test carries a higher risk of adverse reactions than SPT.
Management of Food Allergies
Overall, there has been no strong evidence to support the practice of maternal avoidance of foods during pregnancy and lactation to prevent food allergies in their child. Likewise, the effects of breastfeeding are controversial, but the current guidelines recommend exclusive breastfeeding for the first 4 to 6 months, if possible. Hydrolyzed formulas may be of some benefit if exclusive breastfeeding is not possible, but the evidence is weak in this area. Similarly, there is no good evidence to support the use of probiotics, prebiotics, symbiotics, antioxidants, vitamin D, or folate, and in 2008, the American Academy of Pediatrics modified its position, stating that there was no reason to withhold any foods beyond 6 months of age. 9
Avoidance remains the primary management strategy for food allergies. However, strict elimination can lead to nutritional deficiencies, so patients and parents are encouraged to consult with nutrition specialists to assist in diet planning. The Food Allergy Labeling and Consumer Protection Act of 2006 has made it easier to identify the types of food antigens present in a given product, but there is still no regulation concerning advisory labels with a “may contain” warning. The NIAID guidelines did not address the care of the food allergy patient outside of the office, and further studies are necessary to understand the impact food allergies have on the quality of life of a child, as well as the psychological ramifications of avoidance strategies implemented at parties and in school.
Currently, no medications are recommended for food allergies in a prophylactic capacity, but recent studies have provided promising results for the use of traditional Chinese medicine (TCM) herbal products and monoclonal antibodies. Oral antihistamines may be used for nonsevere reactions, and swallowed corticosteroids are being used in the management of eosinophilic esophagitis. It is extremely important for the clinician to train patients and their families to recognize the signs and symptoms of anaphylaxis, as well as how to use self-injectable epinephrine. Nevertheless, the largest obstacle to overcome is convincing the patient to keep this device available at all times.
Desensitization to peanuts has been attempted using the subcutaneous route but, despite its success in desensitization and induction of oral tolerance, produced an unacceptable amount of local and systemic reactions for it to be put into clinical use. Other routes, such as sublingual and oral immunotherapy, have gained much attention in the recent years, but it is still unclear whether the risks of this therapy outweigh its clinical benefit. Current research is also focusing on methods to improve the safety and efficacy of this therapy, such as the use of genetically modified antigens, overlapping peptide vaccines, plasmid DNA-encoded vaccines, and allergen-conjugated CpG immunostimulatory sequences.
Future Directions
Future efforts must focus on improving the specificity of skin and in vitro testing for IgE-mediated food allergies. We must also identify useful diagnostic testing strategies for non-IgE-mediated food allergies and continue to investigate the manifestations of these reactions. The inflammation produced by food allergies is a systemic problem, and we must look beyond the skin, lower airway, and gastrointestinal tract and examine the impact of food allergies on the upper airway, including the middle, inner, and external ear. Sublingual immunotherapy and oral immunotherapy will both require continued investigation to determine whether they are safe enough and effective enough to recommend to our patients. New technology, such as genetically modified antigens and immunostimulatory sequences, may lead to novel treatment strategies and perhaps even safer forms of subcutaneous immunotherapy for food allergies. In the upcoming years, we must also learn more about the psychosocial impact of food allergies and avoidance measures on parents and children who suffer from this disease.
Conclusions
Food allergies result from the contact or ingestion of a food to which the body is sensitized, producing a heterogeneous, systemic inflammatory reaction that may affect any part of the body, including the head and neck. It is important for otolaryngologists to participate in national and international panels designed to create policies and guidelines on food allergies. We must continue to work closely with our allergy colleagues in other specialties to identify gaps in knowledge and advance the science of food allergies for the benefit of our patients and their families.
Author Contributions
Disclosures
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
This commentary was discussed during a miniseminar at the 2010 AAO-HNSF Annual Meeting & OTO EXPO; September 27, 2010; Boston, Massachusetts.