
Abstract
Objective. Examine the usefulness of large-scale community-based head and neck cancer screening for reducing tobacco use in an at-risk population. Questions answered: (1) Is participating in a community-based head and neck cancer screening related to a reduction in tobacco usage? (2) Do differing factors between participants predict behavior change?
Study Design. Survey based with a longitudinal follow-up component.
Setting. Atlanta Motor Speedway during a National Association of Stock Car Auto Racing (NASCAR) race event.
Subjects and Methods. Recruited NASCAR fans (n = 620). Initial screening and 11-question survey for 6-month telephone follow-up.
Results. One hundred fifty-six participants (25%) required medical follow-up. Chi-square analysis indicated a significantly higher proportion of smokers (13%) evidenced positive findings compared to nonsmokers (8%) or past smokers (6%). Kruskal-Wallis analysis followed by Dunn’s multiple comparison post hoc test indicated smokers were from a significantly lower socioeconomic status background compared to nonsmokers. Analysis of variance indicated contacted participants reported smoking significantly fewer cigarettes per day 6 months postscreening compared to the number of cigarettes smoked at the baseline. Forty-four (59%) participants reported reducing the number of cigarettes smoked per day, and 11 participants reported quitting smoking.
Conclusion. The authors have demonstrated that large-scale community-based head and neck cancer screenings can be effectively implemented in nonmedical venues. This study demonstrated that targeting education for reduction of risk factors in the NASCAR population positively affected tobacco cessation.
Tobacco consumption has been listed as the number one preventable cause of lifestyle-based chronic diseases in the United States. 1 Prevention of lifestyle-based chronic diseases has become a national government initiative and is the focus of the National Prevention, Health Promotion and Public Health Council, a mandate of the Patient Protection and Affordable Care Act (PL 111-148) and signed into law June 30, 2010. The goal of the council is to develop “an integrative health-care strategy that incorporates the most effective and achievable means of improving the health status of Americans and reducing the incidence of preventable illness and disability in the United States.” 2
Attempts to reduce tobacco consumption by the US federal government are not new. Government-funded programs such as Healthy People (1979), Promoting Health/Preventing Disease: Objectives for the Nation (1980), Healthy People 2000 (1990), and Healthy People 2010 (2000) were created to improve the health of people in the United States. These programs sought to establish national health objectives and serve as the basis for the development of state and community initiatives to take an active role in health promotion. 3 Healthy People 2010 was tasked with reducing the overall prevalence of cigarette smoking among US adults to ≤12% by 2010. This objective has not been met, with the incidence of tobacco use in the United States remaining stagnant since 2005 at 46 million people or 21% of all adults continuing to smoke cigarettes or use tobacco products. 4 Those at higher risk for tobacco use include people living below the poverty line, living in the southeastern United States, with less education, or with lower socioeconomic status. 5
Seventy-five percent of all head and neck cancers are related to tobacco use. 6 The International Agency for Research on Cancer, an agency of the World Health Organization, estimates that 60% to 80% of head and neck cancers could be reduced by changing at-risk behaviors, including tobacco use. 7 However, national tobacco cessation campaigns to date have had little impact on reducing mortality from head and neck cancer. 8
The Centers for Disease Control and Prevention (CDC) supports implementing community-based programs that pair tobacco control interventions with programs that reduce smoking-related illness as a method of prevention and education. 9 Community-based screenings provide the opportunity for access to health care and health care education outside the hospital system and differ greatly from office-based screenings. 10 Community-based screenings reach populations who may not receive routine health care or health care education because of limited financial or economic resources and lack of health insurance and/or health care benefits. In head and neck cancer specifically, office-based screenings for head and neck cancer have failed to demonstrate their effectiveness in targeting those most at risk for the development of the disease.11,12 Conversely, the authors have demonstrated that a large-scale community-based head and neck cancer screening of National Association of Stock Car Auto Racing (NASCAR) fans in the southeastern United States was effective in identifying those at greater risk for head and neck cancer. The study found that those screened had a lifetime incidence of smoking at 54%, current smokers at 28%, daily alcohol use at 41%, and smokeless tobacco use 4 times the national average at 14%. Most concerning was a high incidence of signs and/or symptoms of head and neck cancer that required further medical follow-up in 43% of the participants. 13
The aim of this study was to examine the usefulness of a large-scale community-based head and neck cancer screening for reducing tobacco use in a population identified as at risk for head and neck cancer. Specific questions answered were the following: (1) Is participating in a community-based head and neck cancer screening related to a reduction in tobacco usage? (2) Are there demographic differences between those receiving a positive finding on the screening and those with normal results?
Methods
Emory University Institutional Review Board approval was obtained. This study was survey based with a longitudinal follow-up component. Convenience sampling was used to recruit the study sample from a community identified as at risk of developing head and neck cancers. The independent variable was the screening intervention, and the dependent variable was tobacco quit rate.
Participants
Participants were recruited for the study from NASCAR fans touring the midway before entry into the race venue at Atlanta Motor Speedway (AMS) in Hampton, Georgia, over 2 race weekend events in 2008 and 2009.
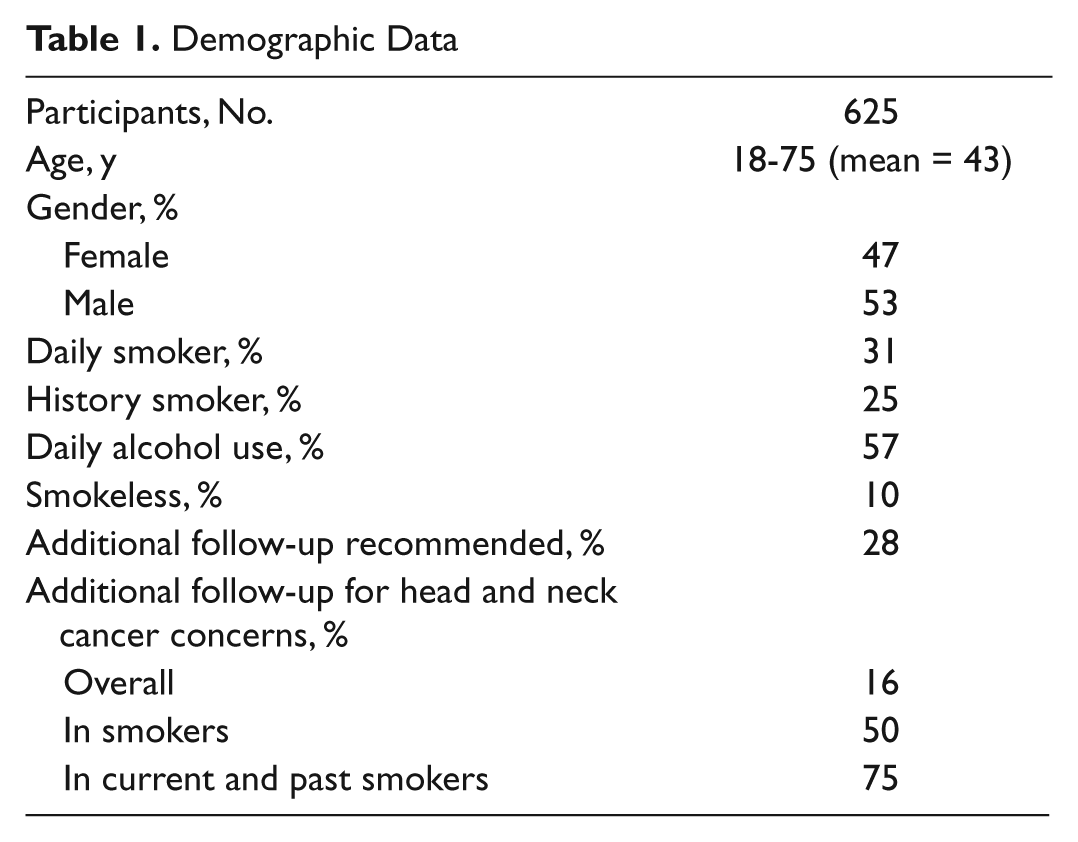
Six hundred twenty male and female participants were consented to be in the study and underwent a head and neck cancer screening and completed an initial survey ( Table 1 ). The survey collected demographic information, relevant medical history about the participant and his or her family history, and information about risk factors for head and neck cancers, for example, current and past tobacco use and alcohol consumption (Appendix A, available at otojournal.org). Participants ranged in age from 18 to 73 years with a mean age of 44 years. The gender distribution matched that of NASCAR race fans with 41% female participants and 59% male participants. 14
Demographic Data
Materials and Procedures
After consenting and completing the initial survey, participants were directed to a private screening room to undergo a head and neck screening by otolaryngologists and/or oral and maxillofacial surgeons that required approximately 15 minutes to complete. The screening was composed of an examination of the oral cavity, including the buccal mucosa, gums, tongue, hard and soft palate, nasal cavity, and pharyngeal and laryngeal cavities, using indirect laryngoscopy with a laryngeal mirror. The survey was adapted from a survey used by the Head and Neck Cancer Alliance for its international Oral Head and Neck Cancer Awareness Week screenings and was used successfully in this population in a previously published study by the authors. 15
Those signs and symptoms considered concerning for cancer or precancerous conditions were documented. Signs and symptoms identified included any of the following: a lump or sore in the mouth; head or neck area that has not healed; a sore throat or cough that does not go away; dysphagia; dysphonia; odynophagia; white or red patches in the mouth, on the gums, or on the lining of the buccal cavity; bleeding in the mouth or nose; swelling in the area of the jaw or neck; swelling under the chin or neck; and intermittent ear pain with no explainable etiology. Results of the examination and any findings were discussed with the participants. During the screening, physicians talked with participants regarding signs and symptoms of head and neck cancer and the risks associated with tobacco use. Physician screeners were told to discuss tobacco cessation during the screening for all tobacco users but were not trained in any specific tobacco cessation methodology. Furthermore, they distributed the Georgia Tobacco Quit Line brochure and several additional smoking cessation brochures from the American Cancer Society to participants. 16
Participants who were current smokers at the time of the screening and a random sampling of past smokers and nonsmokers generated to equal the number of current smokers were contacted by phone 6 months after the initial screening and administered a brief telephone survey about their current smoking behavior (Appendix B, available at otojournal.org). During the telephone follow-up, participants were not informed of their responses regarding tobacco consumption from the original surveys. This information was withheld in an attempt to reduce any bias in tobacco consumption reporting at follow-up.
Results
At the baseline time point, χ2, analysis of variance (ANOVA), and Kruskal-Wallis analyses were conducted to determine if there were demographic differences among smokers, nonsmokers, and past smokers. Chi-square analyses were used to examine frequency data. ANOVA analyses were used to examine for group differences for data that were at the interval or ratio scale level. For data at the ordinal level, Kruskal-Wallis analyses were conducted to detect group differences. To determine whether cigarette smoking behavior changed over time in those participants who evidenced positive findings of head and neck cancer or a concerning finding of precancerous lesions compared to those participants who received a negative screening result, a repeated-measures ANOVA was conducted.
Of the 620 participants who were screened, 156 (25%) evidenced some sign or symptom that required further medical follow-up. Four hundred twenty-two (68%) did not evidence any concerning findings, and data from 42 (7%) participants were missing or their status could not be determined from their screening form. Five hundred seventy-eight participants had a complete screening result. Of those 578, 179 (31%) were smokers, 251 (43%) were nonsmokers, and 148 (26%) were past smokers. Chi-square analysis indicated that a significantly higher proportion of smokers (13%) evidenced positive findings compared to nonsmokers (8%) and past smokers (6%), χ2 (n = 578) = 28.25, P < .001. A significantly higher proportion of men (16%) evidenced positive findings compared to women (10%), χ2 (n = 578) = 4.81, P < .05. ANOVA analysis indicated a significant main effect of age across smoker classification groups, F(2, 575) = 10.92, P < .001, η2 = .04. Tukey post hoc analysis (P < .05) indicated that past smokers were significantly older (mean = 46.99) than smokers (mean = 40.40) and nonsmokers (mean = 42.89). With respect to socioeconomic status (SES), Kruskal-Wallis analysis indicated a significant difference across smoker classification groups, χ2 (n = 578) = 18.13, P < .001. Follow-up Dunn’s multiple-comparison post hoc test (P < .05) indicated that smokers were from a significantly lower SES background compared to nonsmokers.
Seventy-five participants (47%) who self-identified as smokers at the time of the screening were able to be contacted by phone at 6 months after the initial screening ( Figure 1 ). A 2 (screening findings) × 2 (time point) repeated-measures ANOVA indicated that overall, participants reported smoking significantly fewer cigarettes per day (mean = 13.78) at the 6-month follow-up compared to the number of cigarettes (mean = 19.43) smoked at the baseline time point, F(1, 72) = 31.86, P < .001, η2 = .31. Importantly, there was no difference in the rate of smoking reduction between those participants who had a positive screening and those who did not. Forty-four (59%) participants reported reducing the number of cigarettes they smoked per day, and 11 participants reported quitting smoking (14.6%).
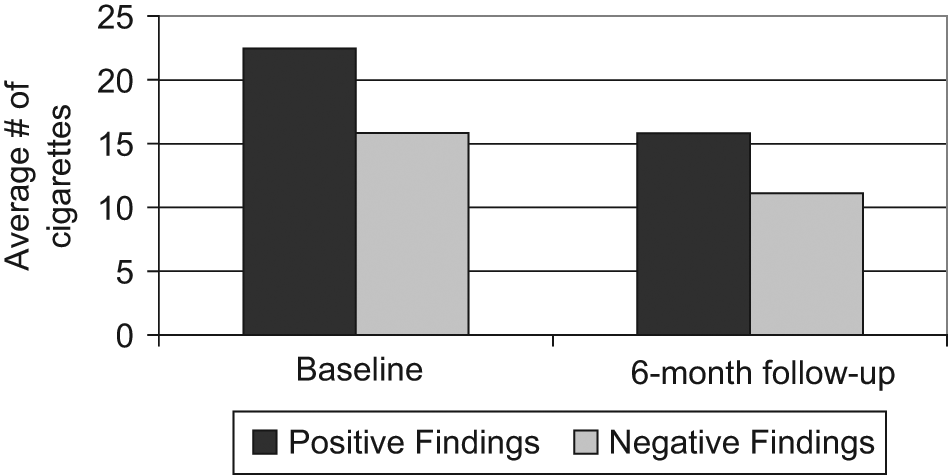
Tobacco usage at initial and 6-month follow-up time points.
Discussion
The results of this study suggest that the screening may have affected tobacco cessation. However, this study did not use a comparison group, and other factors may have contributed to the reduced rate of tobacco use. Participants self-selected to be screened for head and neck cancer, and this may have influenced the quit rate as it is well established in the literature that people quit smoking for a variety of reasons, often outside organized smoking cessation programs.
The findings from this study parallel previously published research indicating that men are 4 times more likely to have cancers of the head and neck because of greater use of cigarette smoking. Those participants who were male, were older, were from a lower SES household, and reported higher cigarette consumption demonstrated a higher incidence of concerning signs and symptoms of head and neck cancer. The incidence of smoking found in this study (31%) was slightly higher than that found in previously published NASCAR literature at 28%; however, both are 1.5 times the incidence of tobacco use reported in the US general population. Although not specifically addressed in this study, previous literature reports a high rate of daily alcohol consumption in NASCAR fans. This high rate of smoking and the increased incidence of head and neck cancer with the synergistic use of tobacco and alcohol supports that this population is at increased risk for head and neck cancer.
The American Cancer Society estimated that in 2010, there would be more than 171,000 deaths related to the use of tobacco products in the United States. These figures support the notion that national tobacco cessation campaigns over the past 30 years have had little impact on reducing mortality from head and neck cancer. Mechanisms to reduce or eliminate at-risk behaviors such as smoking and the use of smokeless tobacco face ever-decreasing availability of funds to support programs. Nationally supported organizations such as The Tobacco Quit Line have been shown to reduce tobacco consumption rates by up to 56%, but these programs continue to lose funding.
In Georgia, the location of data collection and a site of previous research by the authors, the CDC has reported that 59% of adult smokers have made at least 1 quit attempt in the past year. 17 Information regarding the Georgia Tobacco Quit Line was given to participants at the time of the initial data collection but not queried to its use during the follow-up telephone calls. Research into the success of quit lines indicates that they have a low rate of follow-up. 18
The current study found that there was a 15% quit rate among smokers who received a head and neck cancer screening and found no difference in quit rates between smokers who demonstrated a concerning finding during the screening requiring medical follow-up and those who had no concerning findings. The study suggests that smokers did not reduce tobacco consumption when faced with the possibility that they had presented signs or symptoms concerning for head and neck cancer. The literature has demonstrated that smokers tend to underestimate their risk for other cancers, specifically lung cancer, when compared to nonsmokers.19,20 Perhaps this study is consistent with previous research that smokers have reduced risk perception for head and neck cancer and that perceived risk drives behavior change, specifically smoking cessation. 21
The Institute of Medicine’s recommendation for support of community mobilization for tobacco control is consistent with recommendations made by the CDC for comprehensive community tobacco prevention programs. Perhaps, as suggested in other screening initiatives such as for diabetes, community-based screenings may provide the mechanism to bring health education to the general public, increasing awareness and reducing at-risk behaviors:
If we think of a continuum of cancer screening interventions stretching from physician-based chart reminders to the ideal community-based intervention, it is clear that much progress has been made. The field, as a whole, is shifting towards interventions that employ outreach to community members.
22
One limitation of this study is that a large number of smokers could not be reached by telephone for a follow-up interview. Although previous studies have successfully used a telephone follow-up format to assess adherence to smoking cessation treatments, this format may not be the most appropriate to be used with this population. Only half of the current smoking group at the 6-month time point was able to be contacted for follow-up. Many of the participants in this study came from low SES households, and anecdotally, there were many disconnected phone numbers. Furthermore, many smokers did not return calls to the surveyors despite multiple messages requesting a return call, and these individuals may be fundamentally different in their smoking behavior from those who were reached. Future studies focused on this population should document multiple pieces of contact information (eg, e-mail, home address) to ensure a higher rate of collection of follow-up data.
A second limitation was that the study was based on self-report of smoking status and not biochemical assessments of blood/urine. The participants were blind to the amount of cigarettes they reported smoking at baseline; however, a consistent reporting of a reduction of smoking across participants suggests that the self-reported decline in cigarette use was real and not a result of social desirability. Furthermore, previous research has found that self-reported data on current smoking have high assessment validity. 23
Conclusions
Although cause and effect of the screenings for tobacco cessation cannot be established in this study, the goal of the study—to determine the usefulness of this community-based screening initiative to provide yet another opportunity to educate an at-risk population regarding tobacco cessation—was demonstrated. Little is known about the impact of large-scale head and neck cancer screenings in changing at-risk behaviors. More must be done at national, state, and community levels to support tobacco cessation in venues outside those funded government programs that historically have had little impact on tobacco use and head and neck cancer mortality. Physicians and health care workers must take the lead in developing creative avenues to teach their patients about tobacco cessation and its link to cancer and other diseases. Future research will address the impact of this type of large-scale community-based head and neck cancer screening to improve earlier access to health care, earlier detection of head and neck cancer, the impact of this early detection on reducing mortality from these cancers, and improvement of tobacco cessation education.
Author Contributions
Disclosures
Footnotes
Acknowledgements
We acknowledge the Oral Head and Neck Cancer Advocacy Foundation, Madeleine Haugh, and Elizabeth Heller for their cooperation and assistance in completing this research.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
This article was presented at the 2010 AAO-HNSF Annual Meeting & OTO EXPO; September 26-29, 2010; Boston, Massachusetts.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.