
Abstract
Objective. Although approved by the US Food and Drug Administration for clinical use, the utility of handheld tissue reflectance and autofluorescence devices for screening head and neck cancer patients is poorly defined. There is limited published evidence regarding the efficacy of these devices. The authors investigated the sensitivity and specificity of these modalities compared with standard examination.
Study Design. Prospective, cross-sectional analysis.
Setting. Tertiary care medical center.
Subjects and Methods. Patients who were treated previously for head and neck cancer (n = 88) between 2009 and 2010 were included. Patients were screened using white light visualization (standard of care) and compared with tissue reflectance and autofluorescence visualization. Screening results were compared with biopsy or long-term follow-up.
Results. Autofluorescence visualization had a specificity of 81% and a sensitivity of 50% for detecting oral cavity cancer, whereas white light visualization had a specificity of 98% and a sensitivity of 50%. Tissue reflectance visualization had low sensitivity (0%) and good specificity (86%). The power of this study was insufficient to compare the positive and negative predictive values of standard white light examination (50% and 98%, respectively) to tissue autofluorescence (11% and 97%) or reflectance (0% and 95%). In addition, stratification by previous radiation therapy found no statistically significant difference in screening results.
Conclusion. Standard clinical lighting has a higher specificity than tissue reflectance and autofluorescence visualization for detection of disease in patients with a history of head and neck cancer. This study does not support the added costs associated with these devices.
Keywords
Oral cavity cancer accounts for almost 130,000 deaths annually worldwide and is the sixth most common cancer worldwide.1,2 In the United States, the overall 5-year survival for all stages is 59% and decreases to 52% for those with regional disease. 3 Screening strategies to detect cancers at an early stage or in the premalignant phase may improve statistics. Furthermore, approximately 5% of those patients who do survive their initial disease are at risk of developing a second primary cancer, and approximately 19% are at risk of developing a local recurrence. 4 Therefore, a routine follow-up schedule is recommended to promote early detection of new lesions. However, oral cavity examination in previously treated patients is often complicated by diffuse mucosal changes from field cancerization, prior surgery, and radiation therapy. An optimization of detection rates by noninvasive screening techniques balanced with cost-effectiveness is needed for detection of both primary and secondary oral cavity cancer.
Currently, the standard of care for the oral cavity cancer screening is visual inspection under white light (traditional examination light) and palpation by a physician or dentist. The sensitivity of this technique is highly dependent on the experience of the examiner, and therefore more objective methods were developed. In recent years, it was discovered that oral cavity tissues contain fluorophores, such as nicotinamide adenine dinucleotide dehydrogenase and the cross-links between collagen and elastin. These fluorophores absorb UV photons and emit lower energy, longer wavelength photons. These longer wavelength photons can be visualized as fluorescence.5,6 Neoplastic lesions have a decreased number of collagen and elastin cross-links, and therefore fewer of the longer wavelength photons are emitted, leading to a decrease in the amount of fluorescence visualized.6-8 In addition, it was found that the 540- to 575-nm wavelengths are able to detect changes in vasculature by enhancing the reflective properties of the mucosa. As a result, tissue reflectance appears darker in areas of increased vasculature. Handheld devices have been designed that include filters that allow clinicians to visualize tissue fluorescence and reflectance in the clinic. In recent years, these handheld tissue autofluorescence9,10 and reflectance 10 screening devices have been marketed to primary care and dental offices. These devices have been approved by US Food and Drug Administration for oral cavity screening. Although these instruments have the potential to improve detection of mucosal dysplasia and cancer in situ, their efficacy as screening tools remains unproven.
As these devices become more common in the clinic, their reliability to differentiate a benign oral cavity lesion from a premalignant or malignant lesion must be assessed. In addition, the added cost of these screening modalities must be evaluated relative to their potential benefit. To this end, we evaluated patients undergoing routine head and neck cancer surveillance using the Identafi 3000 device manufactured by Trimira (Houston, Texas). This device combines the technologies of tissue autofluorescence and reflectance, making it unique from other handheld oral cavity screening devices.
Materials and Methods
Patient Selection
Following institutional review board approval, a prospective study was performed at the University of Alabama at Birmingham. Consecutive patients who presented to the otolaryngology clinic during defined clinic times between November 2009 and October 2010 for follow-up (n = 88) following management of primary head and neck cancer were included. Data obtained included patient age, gender, race, social history, original cancer stage, other comorbidities, and prior treatments. Tumors were staged according to the American Joint Committee on Cancer (AJCC) 11 guidelines, and histology was confirmed by pathology.
Imaging Procedure
Oral cavity and oropharynx sites were initially screened by a registered nurse and then by a head and neck surgeon using visualization with white light illumination (traditional examination light) followed by visualization of tissue autofluorescence and tissue reflectance. The Trimira Identafi 3000 ultra, multispectral oral cavity screening system was used. Any abnormality was assessed by the head and neck surgeon, and if there were concern for malignancy or recurrence, the abnormal lesion was biopsied. Screening results were compared with histological biopsy results or a 3-month follow-up screening.
Histopathologic Correlation
Any area of abnormality found by visualization with traditional white light illumination and/or by tissue autofluorescence or reflectance was biopsied and evaluated by a pathologist using standard histopathologic analysis. The location of the biopsy was noted in the patient’s chart.
Statistical Analysis
The statistical analysis was done using GraphPad Prism software (GraphPad Software, San Diego, California). Analysis included calculation of sensitivity, specificity, positive predictive value (PPV) and negative predictive values (NPV), and their respective 95% confidence intervals (CIs) for outcomes of the different screening visualization modalities (white light, tissue autofluorescence, and tissue reflectance).
Results
Screening in Previously Treated Patients
We evaluated patients during routine surveillance visits. All patients had undergone a previous treatment for head and neck cancer. The patients were primarily elderly (mean age 64 years; range, 41-85 years), white (61%, n = 54), and male (74%, n = 65). All patients were in the first 5 years of follow-up. The most common location of the primary tumor was the oral cavity (47%, n = 41), followed by the oropharynx (25%, n = 22) and larynx (24%, n = 21). The remaining sites included the maxillary sinus (n = 2), nasopharynx (n = 1), and temple (n = 1). The majority of patients had undergone treatment for stage IV (57%, n = 50) or stage III (19%, n = 17) head and neck cancer. The majority had a history of tobacco use (81%, n = 71) or alcohol consumption (66%, n = 58). The majority of patients had undergone surgical excision of their primary lesion (85%, n = 75), and 73% (n = 64) had undergone previous radiation therapy, whereas only one-third had received chemotherapy (38%, n = 33).
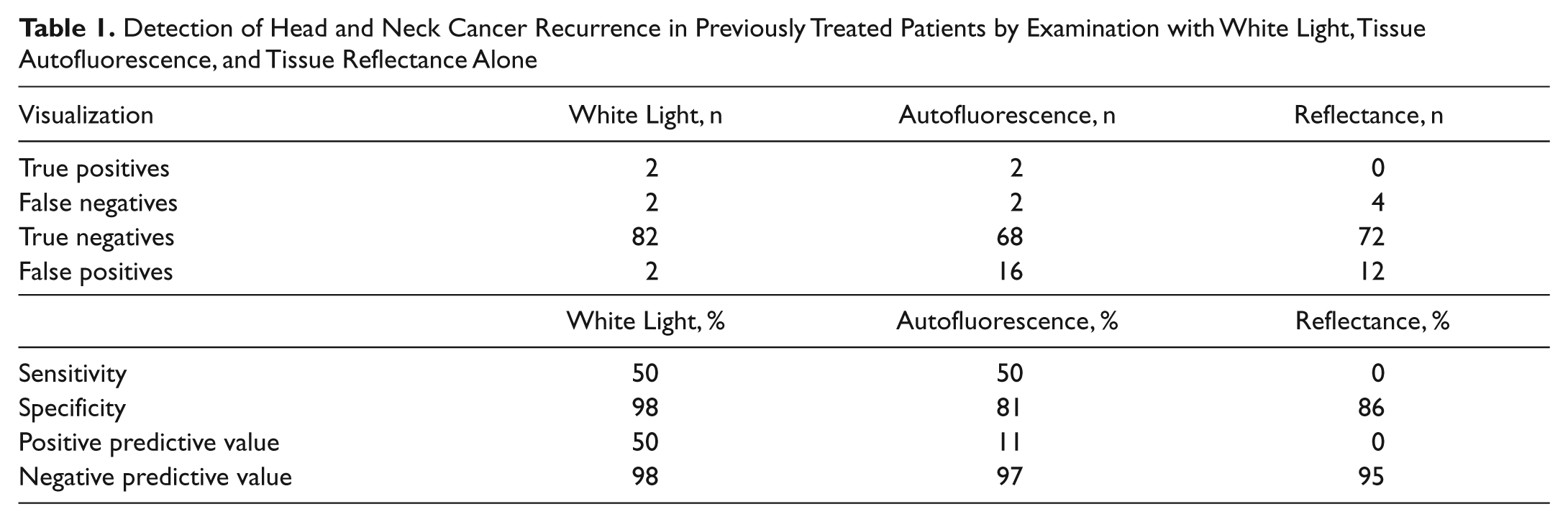
Patients were evaluated by direct visualization of the oral cavity with white light (traditional examination light), tissue autofluorescence, and tissue reflectance. The patients experienced no harmful or adverse side effects from the screening. A total of 4 patients were found to have positive disease by biopsy confirmation or development of a recurrence less than 3 months following screening. There were a total of 17 lesions identified by tissue autofluorescence and/or reflectance, of which 9 underwent biopsy. There were no lesions detected by tissue autofluorescence or reflectance that were not detected by white light. There were 9 lesions identified on autofluorescence that were determined to be benign by the clinician and were followed for 6 months without change. Although the power was insufficient to state definitively, it could be extrapolated that screening with white light illumination has better overall results with a specificity of 98% (95% CI, 92%-100%), a sensitivity of 50% (7%-93%), a PPV of 50% (7%-93%), and an NPV of 98% (92%-100%) ( Table 1 ). Screening with tissue autofluorescence visualization had a specificity of 81% (95% CI, 71%-89%), a sensitivity of 50% (7%-93%), a PPV of 11% (1%-35%), and an NPV of 97% (90%-100%). Screening with tissue reflectance illumination had low sensitivity (0%; 95% CI, 0%-60%) and PPV (0%; 0%-27%) and good specificity (86%; 76%-92%) and NPV (95%; 87%-99%). A summary of screening results is found in Table 1 . In addition, stratification by previous radiation therapy found no statistically significant difference in screening results ( Tables 2 and 3 ).
Detection of Head and Neck Cancer Recurrence in Previously Treated Patients by Examination with White Light, Tissue Autofluorescence, and Tissue Reflectance Alone
Detection of Head and Neck Cancer Recurrence in Previously Irradiated Patients by Examination with White Light, Tissue Autofluorescence, and Tissue Reflectance Alone
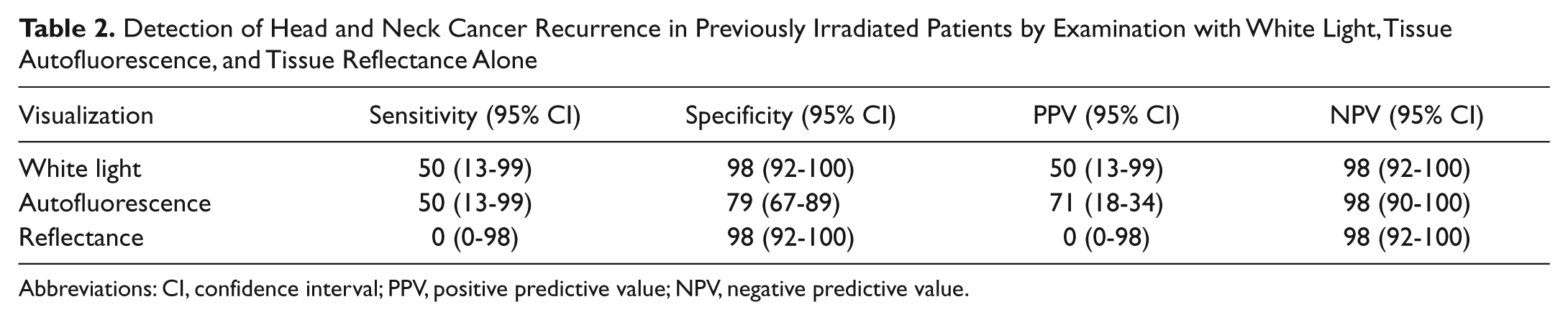
Abbreviations: CI, confidence interval; PPV, positive predictive value; NPV, negative predictive value.
Detection of Head and Neck Cancer Recurrence in Previously Nonirradiated Patients by Examination with White Light, Tissue Autofluorescence, and Tissue Reflectance Alone
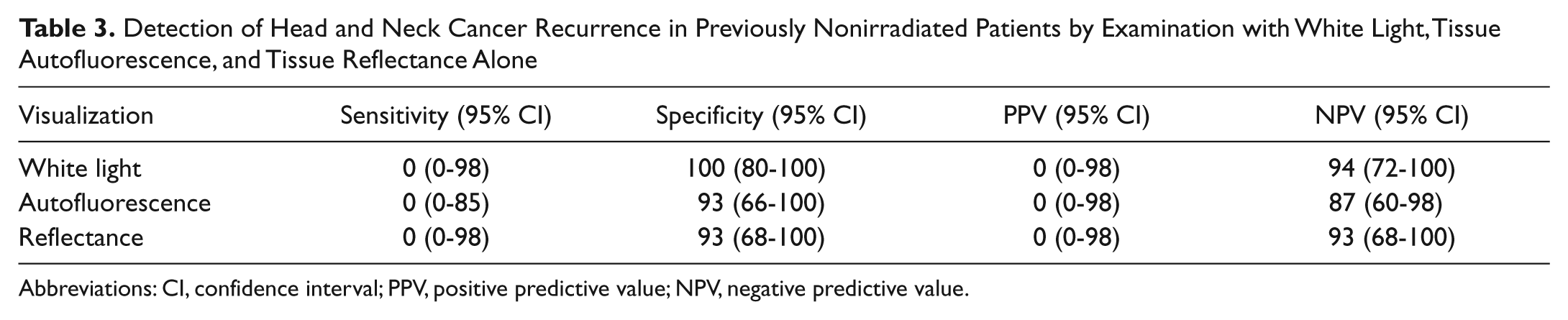
Abbreviations: CI, confidence interval; PPV, positive predictive value; NPV, negative predictive value.
Discussion
Despite the widespread proliferation of approved devices using tissue autofluorescence or reflectance for screening of oral cavity cancer, there is limited data to support their use. We present the first prospective study addressing the application of this technology for oral cavity cancer screening in previously treated patients. Examination with white light and pathological confirmation remain the gold standard for early detection of oral cavity malignancies. However, clinical examination remains subjective. Several noninvasive fluorescence screening modalities have been developed to improve malignancy detection rates. These technologies range from devices requiring direct contact with the tissue, such as fiber-optic spectrometers 12 and depth-sensitive optical spectroscopy, 13 to full-field measurements of autofluorescence using visualization aids such as VELscope and Identafi.14,15 Subtle changes in early cancer cellularity and blood flow are the basis for development of light-based screening strategies to improve the sensitivity and specificity of routine examination. Although previous case reports have identified the utility of this technology in evaluation of known lesions,6,8,16,17 our data suggest that the addition of tissue autofluorescence or reflectance illumination to routine clinical examination of high-risk patients has very limited benefit and does not justify the additional time or expense associated with their use.
Even though screening with white light illumination provides a cost-effective means of screening for oral cancer, this technique remains subjective and has limited sensitivity. In low-risk patient populations, screening for oral cavity cancer with white light visualization was found by systematic review to have a weighted pooled sensitivity of 85% and specificity of 97%, 18 whereas others found a sensitivity of 64% and PPV of 74%. 19 Variables affecting the sensitivity and specificity of traditional white light visual examinations include index of suspicion and experience of the examiner. 6 The difficulty in detecting oral cavity neoplastic lesions is confounded by field cancerization in which up to 58% of biopsies of normal-appearing mucosa are found to have histologic abnormalities (cellular atypia, dysplasia, squamous cell carcinoma).
In an effort to improve detection rates of new primaries and recurrence, several autofluorescence devices have been introduced to aid detection. Some studies have found oral cavity visualization under autofluorescence to be advantageous for assessment of known neoplastic disease16,17,20 when compared to white, incandescent light alone. Marketing materials state that “dentists, oral surgeons, primary care physicians, and otolaryngologists now have the technology to detect oral cancer earlier and save lives” (www.trimira.net). However, there is limited evidence in the peer-reviewed literature that tissue autofluorescence or reflectance can be used to detect cancer during screening visits and no data it saves lives. The lack of consensus on the potential benefit of this technology is related to study design flaws and insufficient data found within the literature.18,19,21,22
One group performed 50 biopsies from areas with changes in tissue autofluorescence and showed a sensitivity of 98% and specificity of 100% for identification of dysplasia, carcinoma in situ, or invasive cancer. 16 However, this broad classification of success does not significantly improve clinical decision making or suggest that it can be used for screening or to make comparisons to white light examination. More objective measures have been developed to assess tissue autofluorescence and have demonstrated sensitivity of 90% and specificity of 87%, but this requires a quantitative computer-based algorithm. 23 Furthermore, this study used clinical consensus rather than pathology or clinical follow-up as the gold standard to determine sensitivity and specificity. Other studies have evaluated autofluorescence visualization as a diagnostic aid for oral cavity lesions not suspicious for neoplasia and requiring only serial follow-up. 15 In this setting, autofluorescence was found to be of no benefit. In addition, no lesions were detected with autofluorescence that were not already apparent on white light examination. Similarly, we found that use of tissue autofluorescence in previously treated head and neck cancer patients was equivalent to standard white light examination. In the current study, we demonstrate a sensitivity of 50% and specificity of 98% for white light visualization compared with tissue autofluorescence, which had inferior specificity (81%) and equivalent sensitivity for screening these high-risk individuals. There were only 2 false-negative screenings by white light examination; 1 lesion was in a location out of the range of visualization by the naked eye (the base of tongue and detected by fiber-optic scope examination), and the second lesion was initially screened at the first postoperative follow-up and was found to be a local recurrence in the surgical site a few weeks later. The low specificity of screening in this patient population may be attributed to postoperative and postradiation changes in the oral mucosa resulting in pigmentation and fibrosis. When examining oral cavity mucosa using white light or tissue autofluorescence or reflectance, dysplastic lesions were difficult to differentiate from benign changes in the mucosa, such as inflammation, ulceration, or radiation changes. Only 4 patients had evidence of recurrence, and therefore the power was limited and is likely the explanation for the low sensitivity of screening in this patient population.
Our study was unique in that it evaluated the patient population most likely to benefit from screening. However, patients previously treated for head and neck cancer, particularly those with a history of radiation, may suffer diffuse changes that make tissue autofluorescence a poor tool for early diagnosis of a new primary or recurrence. Areas of inflammation, ulceration, or radiation damage cause changes to the underlying stroma and basement membrane, which result in loss of tissue autofluorescence, making differentiation between these benign changes and dysplastic changes difficult. Changes in stromal fluorescence observed in dysplastic lesions are similar to loss of stromal fluorescence associated with inflammatory changes. 7 It is possible that postradiation changes or xerostomia are sufficient to cause low-level inflammation, which limits the value of autofluorescence screening. It would appear in this setting autofluorescence does not enhance visualization of neoplastic lesions and would increase the false-positive rate and as a result lead to unnecessary biopsies when compared with white light examination. Ultimately, use of autofluorescence (much like the standard of care) relies on subjective interpretation of visual inspection, and therefore it is qualitative in nature and will vary depending on the examiner and level of experience.
Our study also evaluated tissue reflectance, which has not been previously evaluated for head and neck cancer screening but is also marketed in this capacity. Tissue reflectance in the setting of these multispectral devices is based on the premise of detecting changes in angiogenesis with green-amber light (540- to 575-nm wavelength) illumination. The amber light is thought to enhance the reflective properties of the oral mucosa, allowing a distinction between normal and abnormal tissue vasculature. 10 Surprisingly, there are no published results evaluating this technology. Our study found its ability to detect recurrence or a second primary to be poor with a sensitivity of 0%, specificity of 86%, PPV of 0%, and NPV of 95%. We therefore found tissue reflectance visualization to be inferior to traditional white light examinations. The suggested retail price of these devices ranges between $2000 and $3500; the cost of the device used in the current study is $3390.00, and replacement covers cost $2.50 per patient. Although most insurance companies do not cover the cost of mucosal screening (CDT code D0431), the reimbursement for this office examination has been cited within the range of $25 to $70 per patient, although some dental offices will perform the screening at no cost to the patient.
This study focused on previously treated head and neck cancer patients undergoing evaluation by physicians with experience examining the oral cavity for malignancies. As a result, the utility of these devices for patient screening in the primary care setting remains unclear. Although all lesions found by tissue autofluorescence and/or reflectance were not biopsied, they were evaluated for at least 6 months and were still considered to demonstrate no evidence of disease by current standards of care. Therefore, we believe the added discomfort and cost to the patient were not justified. White light examination was performed first as the standard of care followed by the Identafi 3000 examination, which may have biased the results of the study. However, visualization using autofluorescence or reflectance is relatively straightforward because the dark areas (areas of decreased fluorescence or reflectance) are clearly delineated from tissues with fluorescence or reflectance properties. Furthermore, for the white light examination, there is a clear advantage in favor of the examinees in the environment evaluated in this study. Specialty trained head and neck surgeons have extensive experience, allowing them to more easily differentiate malignancy or dysplasia from mucosal abnormalities caused by irradiation changes or inflammation. Because these devices are also marketed to dentists and otolaryngologists possessing significant oral examination experience, to a small degree, the findings of this study can be generalized to these providers.
Conclusion
Although this was a pilot study, it suggests that tissue autofluorescence and reflectance are equivocal to white light examination, highlighting the need for further investigations validating the efficacy of these screening devices and justifying the additional cost. In the setting of trained physicians and health care staff, our data suggest that the addition of tissue autofluorescence or reflectance illumination to a routine clinical examination of high-risk patients has limited benefit in detecting lesions. The added cost associated with the tissue reflectance and autofluorescence screening devices does not appear to be justified in this patient population.
Author Contributions
Disclosures
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.