
Abstract
Objective. No specific epidemiology data are available for carcinoma of the uvula. This study aims to analyze the epidemiological characteristics and treatment outcomes of carcinoma of the uvula at the authors’ institution.
Study Design. Case series with chart review.
Setting. Service of ENT–Head and Neck Surgery, University Hospital Complex of Santiago de Compostela (CHUS), Spain.
Subjects and Methods. Retrospective epidemiological study of 21 male patients, mean age 57.52 years, diagnosed with squamous cell carcinoma of the uvula in the CHUS between January 1990 and June 2009.
Results. Most patients presented with odynophagia and exophytic lesions microscopically consistent with moderately differentiated squamous cell carcinoma. Despite the size of the lesions (T1 and T2), more than half of the patients had lymph node metastases at diagnosis. More than 90.0% of patients with lesions larger than 1 cm presented with lymph node metastases. Although more than 70.0% of patients underwent a neck dissection in the first year after diagnosis, only 25.0% were free of metastatic disease. Recurrences occurred at a mean of 14 months from baseline in more than 50.0% of cases. Of the patients, 52.4% died, with a median survival of 38.15 months after diagnosis. The overall 5-year survival was 39.0%. According to tumor size, 5-year survival was 53.0% for T1 and 27.0% for T2.
Conclusion. According to the data, clinical features of carcinoma of the uvula correspond with aggressive tumors, with rapid onset and a major negative impact regardless of tumor size at diagnosis. Early stage patients benefit significantly from surgical treatments with neck dissections.
Incidence of cancer in the oral cavity and oropharynx in Europe and India is high, reaching 20 of 100,000 habitants per year. 1 It is more frequent in the sixth decade of life 2 and is strongly associated with tobacco and alcohol abuse. 3 The role of human papillomavirus (HPV) is not clear.4,5
The available data for cancer of the oropharynx are grouped, showing results that prevent them from being analyzed individually in each zone. 6 In part, this is because of the limits of the anatomical region. According to the American Joint Committee on Cancer (AJCC), of the 4 regions of the oropharynx—the base of the tongue, the tonsils, the posterior wall of the oropharynx, and the soft palate—arbitrariness is more evident in the soft palate due to an absence of anatomical boundaries between the uvula and adjacent structures.
Carcinomas of the uvula are rare, but their location makes them easily diagnosed. Prognosis depends on cervical lymph node (CLN) metastasis, which should be related to the size of the primary tumor (T).7,8 They have a higher risk of bilateral CLN metastasis, the same as all primary tumors from the midline. 9
The uvula is a 1.8-cm unpaired structure that constitutes the convergence of the velopalatine muscles. 10 Anatomically, it is in close relation with deep tissue. The lymphatic drainage of the oral cavity and oropharynx is extensive, and there is evidence that it can cross from one side to the other,11,12 which could explain contralateral CLN metastasis. Sentinel node studies have demonstrated an unpredictable drainage from the midline lymphatic vessels. 13
No specific data are available in the literature about T1-T2 carcinoma of the uvula. Diagnostic approaches, prognostic factors, and treatment outcomes of the malignant lesions from the uvula seem to depend on the epidemiological data for oral cavity and oropharyngeal carcinomas.6,14
The superficial spread of the tumor is an important parameter in oropharynx tumor staging. In the uvula, a tumor that does not reach 2 cm in size can only be T1 and T2. Nevertheless, in the tumor classification, the depth is not mentioned, despite the presence of the great lymph vessel network, which increases the risk of metastases. Cohan et al 5 cite the presence of CLN metastases for soft palate carcinomas to be around 20% for T1 and T2 tumors and 60% to 70% for T3 and T4 tumors.
Because of the anatomical site, as well as the rapid extension and easy dissemination to the CLN with unpredictable laterality, we believe that carcinoma of the uvula has a very different evolution compared to other carcinomas of the oral cavity and oropharynx.
The aim of this study is to analyze the characteristics of patients diagnosed and treated for carcinoma of the uvula in the University Hospital Complex of Santiago de Compostela (CHUS) between January 1990 and June 2009.
Materials and Methods
In this retrospective study of 33 patients diagnosed with carcinoma of the uvula (mean age 57.52 years; range, 41-77 years), all had a confirmatory biopsy of epidermoid carcinoma. None had distant metastasis at the time of diagnosis. Twelve patients were excluded because of doubts about the initial location of the tumor, incomplete clinical history, synchronic tumoral lesions of the head and neck, and monitoring for less than 18 months.
The tumors were classified according to the AJCC criteria. Only T1 and T2 lesions were analyzed through standard clinical methods and with the origin in the uvula as defined by one of the authors (CMM).
Among the variables studied, age, date of diagnosis, initial symptoms, and macroscopic and microscopic aspects were taken into account. Moreover, the presence of clinical CLN metastasis confirmed by computed tomography (CT), dates and type of treatment, and appearance of local/regional recurrence were also analyzed.
Anatomical level of CLN metastasis, the need for CLN dissection according to CT results, and histological characteristics of the metastatic CLN were considered.
The presence of HPV was estimated by a standard protocol using the Clart HPV 2 by Genómica (Madrid, Spain) for virus extraction, purification, and amplification.
The statistical analysis was done with SPSS version 15.0 (SPSS Inc, an IBM company, Chicago, Illinois). The Chi-square formula was used to calculate the dependence of random variables. Cox regression models and Kaplan-Meier curves were used for survival analysis.
Results with a confidence interval higher than 95% or P values lower than .05 were considered statistically significant.
For the statistical analysis, final outcome of the disease was patients deceased at the end of the period.
The study was approved by the CHUS medical ethics board.
Results
All patients were men with smoking and alcohol habits; 16 (76.2%) smoked more than 20 cigarettes per day, and 16 (76.2%) consumed more than 20 g/dL of alcohol per day. It was impossible to calculate pack-years exposure because of a lack of information.
Figure 1 shows distribution according to symptom, macroscopic and microscopic type of lesion, and size.
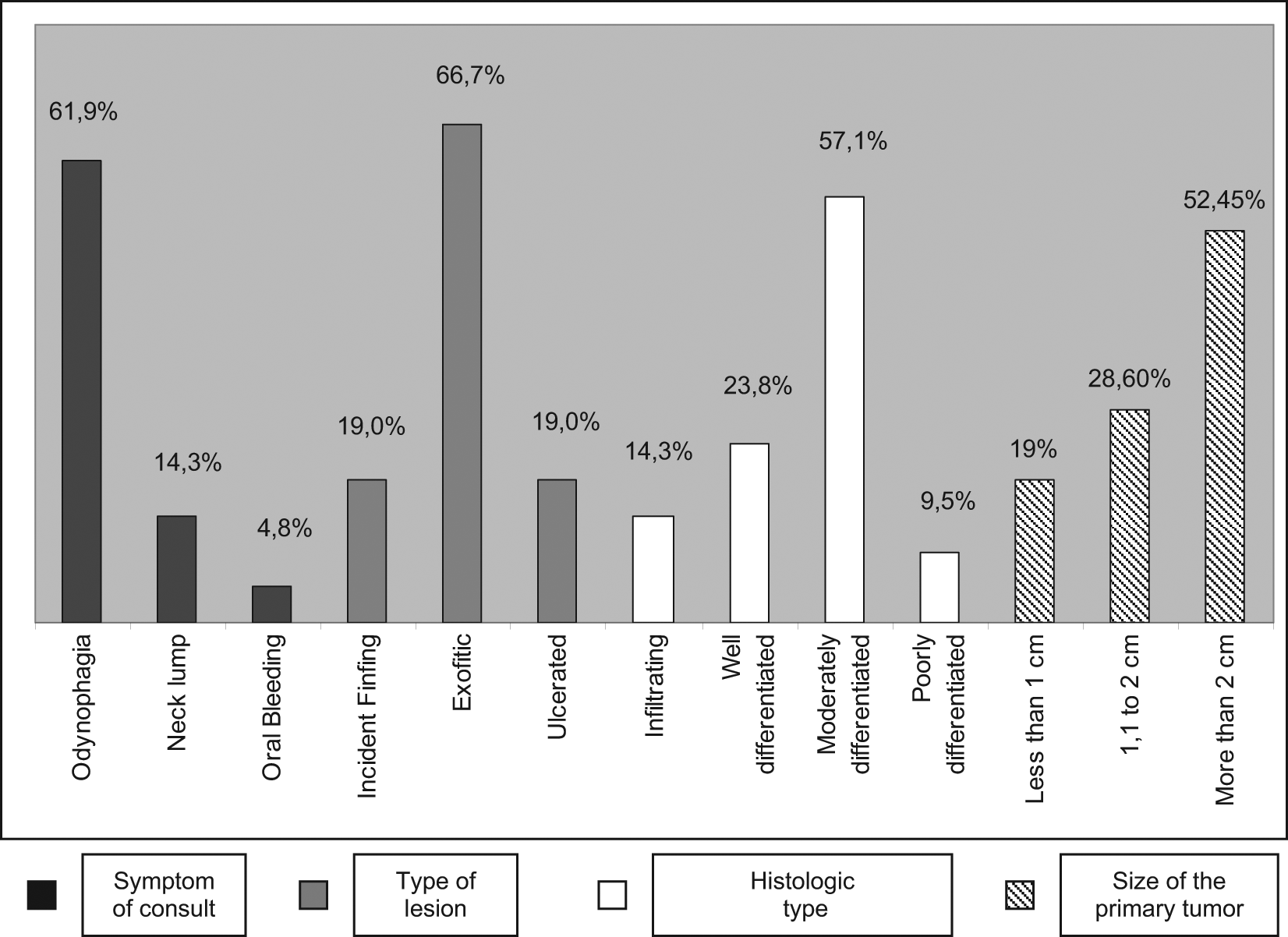
Percentage distribution according to initial symptom, type of lesion, histologic type, and tumor size.
According to the TNM classification, 10 patients (47.6%) were classified as T1 at diagnosis, and 11 (52.5%) were T2. We found statistically significant results when comparing T stage and final outcome (P = .013).
In the first exam, 13 patients (61.9%) had altered CLN (11 [85.7%] unilateral and 2 [13.3%] bilateral), and the remaining 8 (38.1%) had no clinically detectable CLN. All the patients had CLN in neck levels II and III. Of the patients with CLN only, 3 (21.4%) had a favorable evolution to remission of the disease, and the other 10 died with or without evidence of persistence or recurrence. Eleven cases (52.4%) could be attributed to the disease (P = .004).
At diagnosis, 10 patients (47.6%) were classified as T1, and 11 (52.4%) were classified as T2. Eight patients (38.1%) had no CLN enlargement, although after the diagnostic tests (CT and ultrasound), this dropped to 7 (33.3%). Once the initial study of the disease was completed and the case was analyzed by the committee of head and neck tumors, the classifications were as follows: 2 (9.5%) were N1, 9 (42.9%) were N2 (N2a: 2 patients; N2b: 5 patients; N2c: 2 patients), and 3 (14.3%) were N3.
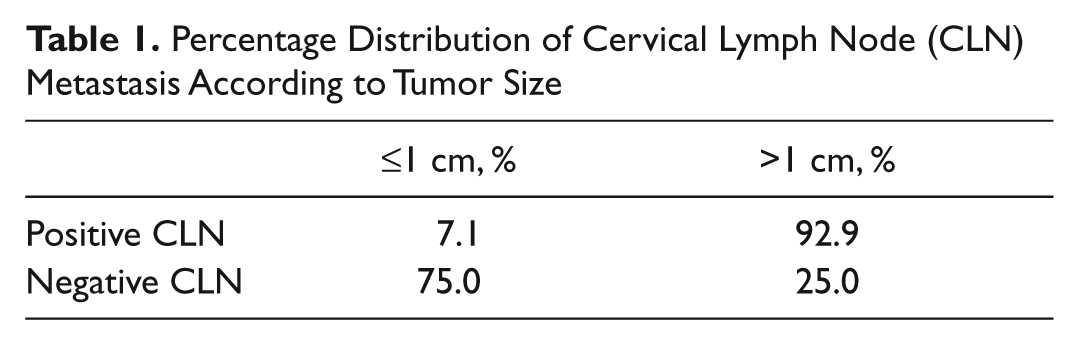
We observed that 6 patients without CLN compromise (75%) had lesions ≤1 cm. By contrast, only 1 patient with CLN metastasis (7.1%) had lesions up to 1 cm in size, and the remaining 12 (92.9%) had lesions greater than 1 cm. We found a statistically significant relationship between tumor size and final outcome (P = .013; Table 1 ).
Percentage Distribution of Cervical Lymph Node (CLN) Metastasis According to Tumor Size
Seven patients (33.3%) had a second primary tumor in the upper aerodigestive area during evolution. We found a direct relation between the presence of a second primary tumor and the final outcome (P = .001).
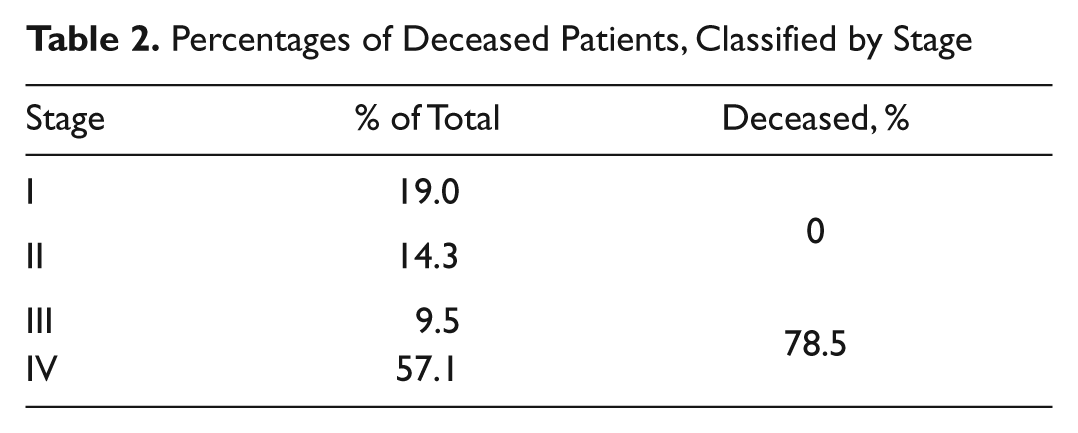
According to the AJCC classification, 4 patients were classified as stage I (19%), 3 were stage II (14.3%), 2 were stage III (9.5%), and the remaining 12 (57.1%) were classified as stage IV. By comparatively analyzing tumor staging and final outcome, we found statistically significant differences (P = .006). Eleven patients (78.5%) in stages III and IV died of the disease, but all patients in stages I and II were free of disease ( Table 2 ).
Percentages of Deceased Patients, Classified by Stage
Patients were divided into 4 treatment groups: 5 patients (23.8%) underwent surgery of the primary tumor; 6 (28.6%) underwent surgery and radiotherapy; 8 (38.1%) received surgery, radiotherapy, and chemotherapy; and 2 (9.5%) received radiation therapy and chemotherapy without surgery (P = .03; Table 3 ). Of the 19 patients who underwent surgery, 17 (90.4%) also received CLN dissection and 15 (80.0%) radiotherapy.
Percentage Distribution of Treatment Groups According to Neck Dissection and Stage
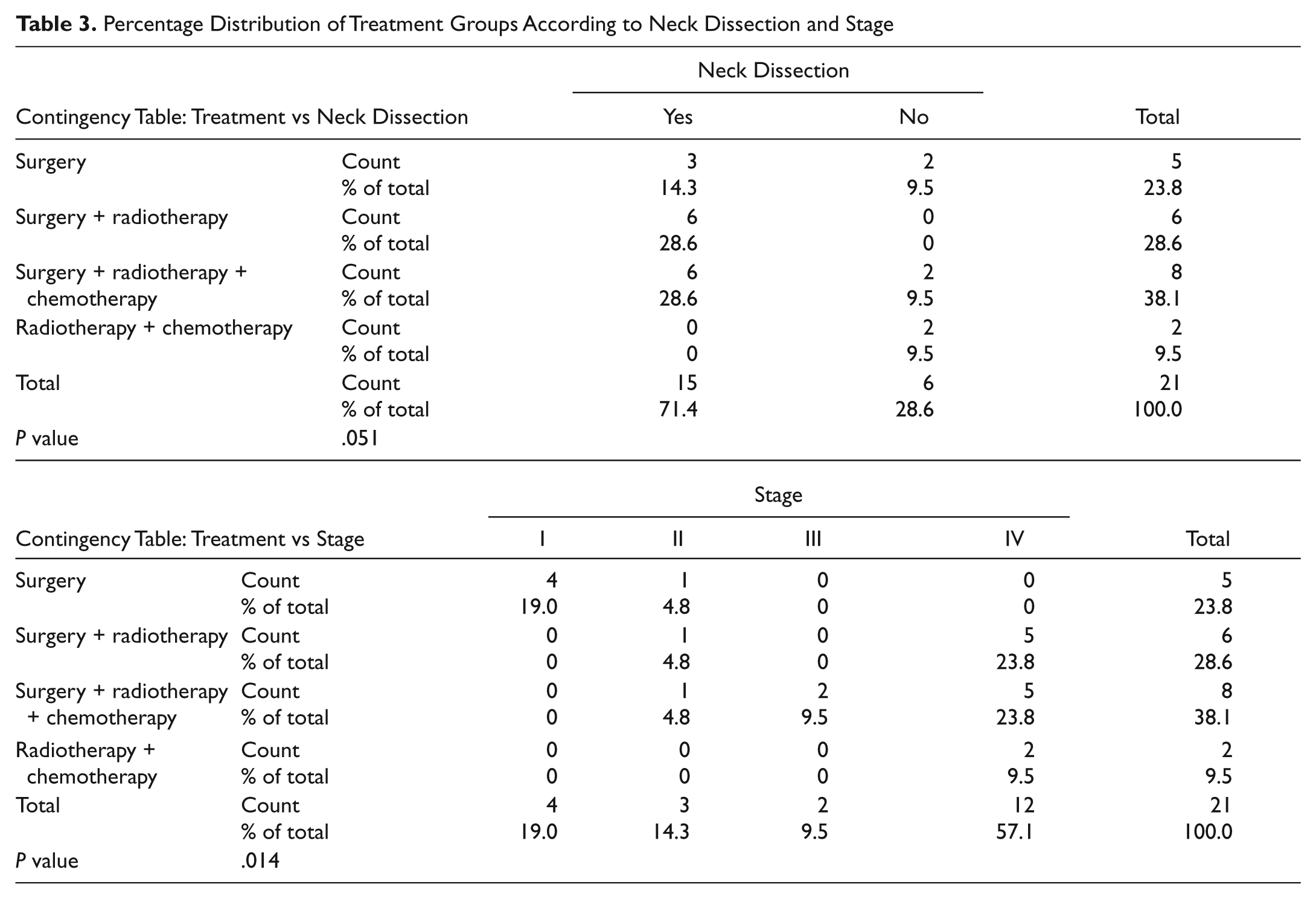
CLN dissection was performed in 15 patients (71.4%), 8 of whom (53.3%) died in the course of the disease. Of the 6 (28.6%) patients who did not undergo dissection, 3 (50%) died.
It is important to note that patients who underwent CLN dissections had remission or death figures that varied greatly depending on the type of treatment offered from their staging. We observed that the 5 patients who underwent surgery only (all in stages I and II) evolved to remission, and 3 underwent prophylactic CLN dissection without pathological evidence of neoplastic infiltration. On the other hand, of the 14 patients requiring additional therapy to surgery (radiotherapy or radiotherapy + chemotherapy), 8 died with confirmed lymph node infiltration.
The distribution between functional (supraomohyoid) and radical neck dissections was 53.4% and 46.6%. The mean number of lymph nodes removed was 20.69 (range, 11-35). The average lymph node infiltration was 2.06 with a range between 1 and 13 nodes. Four patients (25%) who underwent an initial neck dissection showed no infiltrated lymph nodes. Seven patients (46.2%) had capsular rupture, and the average node size was 1.85 cm (range, 1-4 cm). No statistically significant results were found when analyzing capsular spread and final outcome (P = .725).
Five patients (23.8%) required a second contralateral CLN dissection—3 (60%) functional and 2 (40%) radical, with an average of 19.2 lymph nodes removed (range, 6-29) and mean infiltration of 1.6 nodes (range, 1-5). In this group, 3 (60%) had lymph node metastases, and 1 patient had nodes with capsular rupture (average size of lymph nodes was 1.52 cm; range, 1-3 cm).
Seventeen patients (90.48%) who underwent surgical treatment had negative surgical margins, and the remaining 2 (9.5%) had involved margins. Perivascular or perineural invasion was documented in 7 patients.
Depending on the causes of death, 7 patients (64.3%) died as a consequence of the disease. The remaining 4 (35.7%) died of other causes (pneumonia, intestinal perforation, esophageal neoplasm).
Ten patients (47.6%) had recurrence or persistence distributed as follows: persistency, 2; regional recurrence, 3; and locoregional recurrence, 5. The average time of recurrence of any type was 8.25 months (range, 4-22 months). No statistical significance was found when compared with the final outcome (P = .06).
We analyzed the presence of HPV, finding positive results in 5 patients (23.8%). No statistically significant results were found when analyzing the relation between the presence of HPV and the final outcome of the disease (P = .696) or the presence of CLN metastases (P = .920).
According to the clinical course, 11 patients (52.4%) died with a median survival of 38.15 months after diagnosis. The overall 5-year survival was 39.0% ( Figure 2 ). According to tumor size, 5-year survival was 53.0% for T1 and 27.0% for T2 ( Figure 3 ). With regard to nodal involvement, 5-year survival was 100.0% for N0 and 50.0% for N1, decreasing significantly to 14.0% for N2 and 0% for N3 ( Figure 4 ). Five-year survival for was 100.0% for stages I and II, 50.0% for stage III, and 16.0% for stage IV ( Figure 5 ).
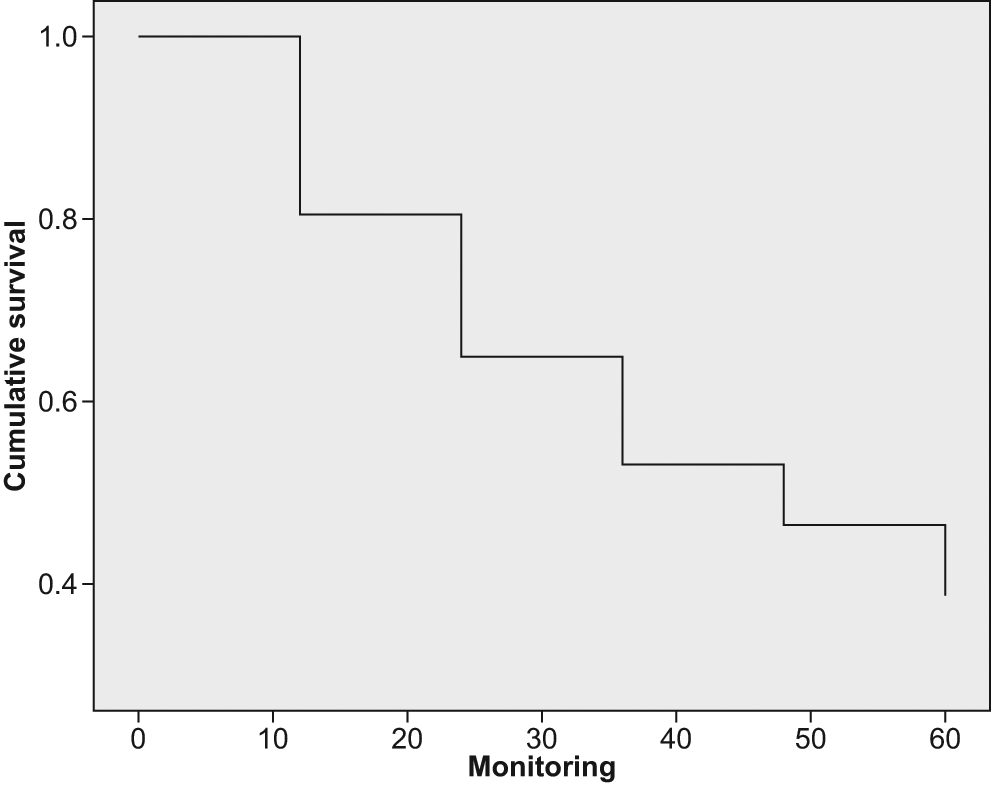
The x-axis corresponds to the time of monitoring in months, and the y-axis corresponds to the percentage of cumulative survival. Approximately 50.0% of the patients were deceased between 30 and 40 months from diagnosis.
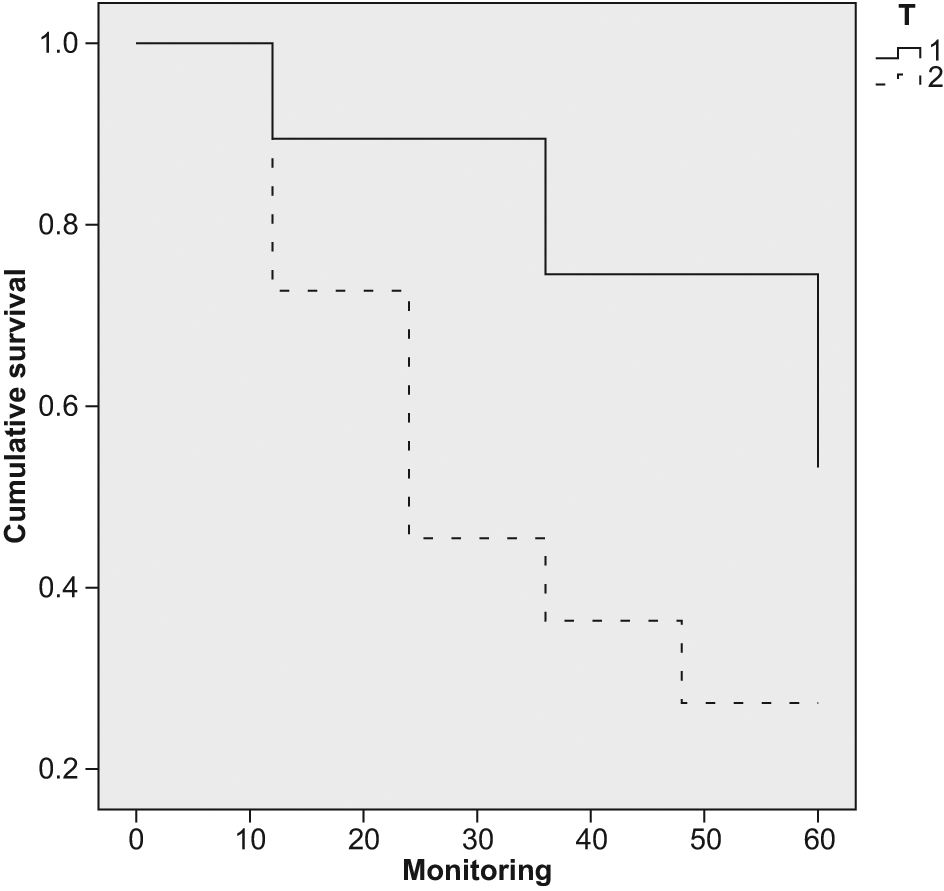
Survival function showing significantly lower survival rates for T2 tumors.
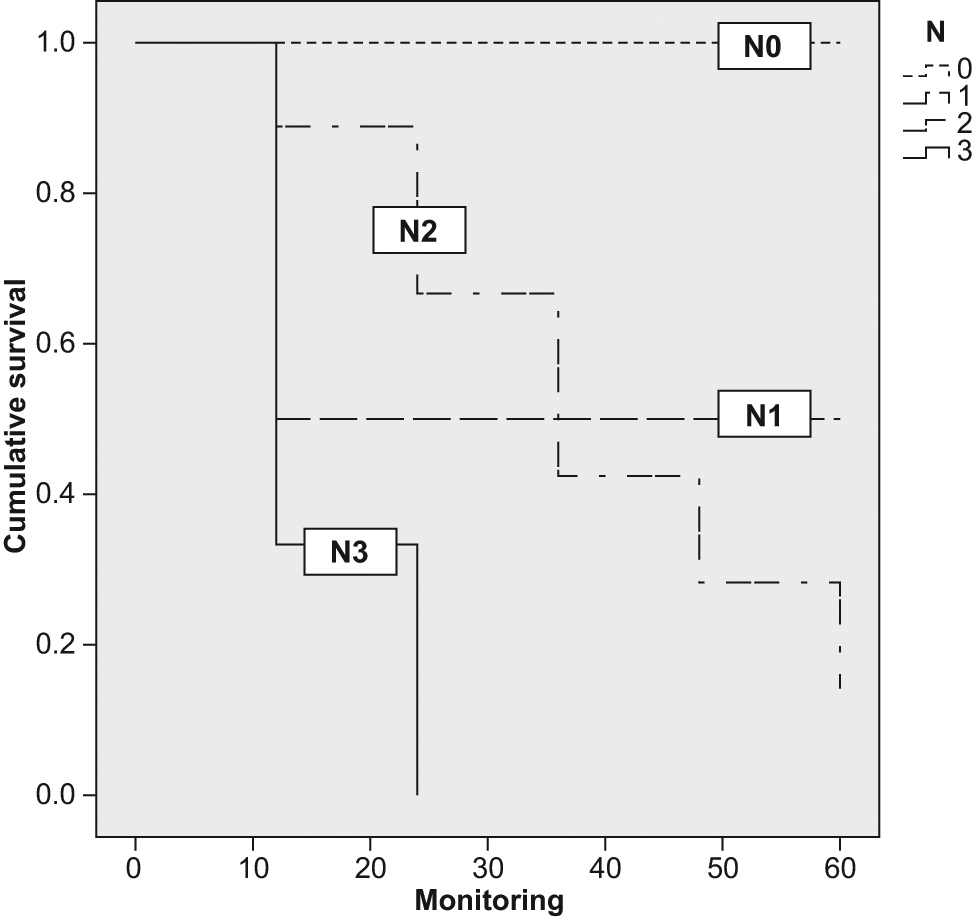
Survival function showing significantly lower survival rates for N2 and N3 disease.
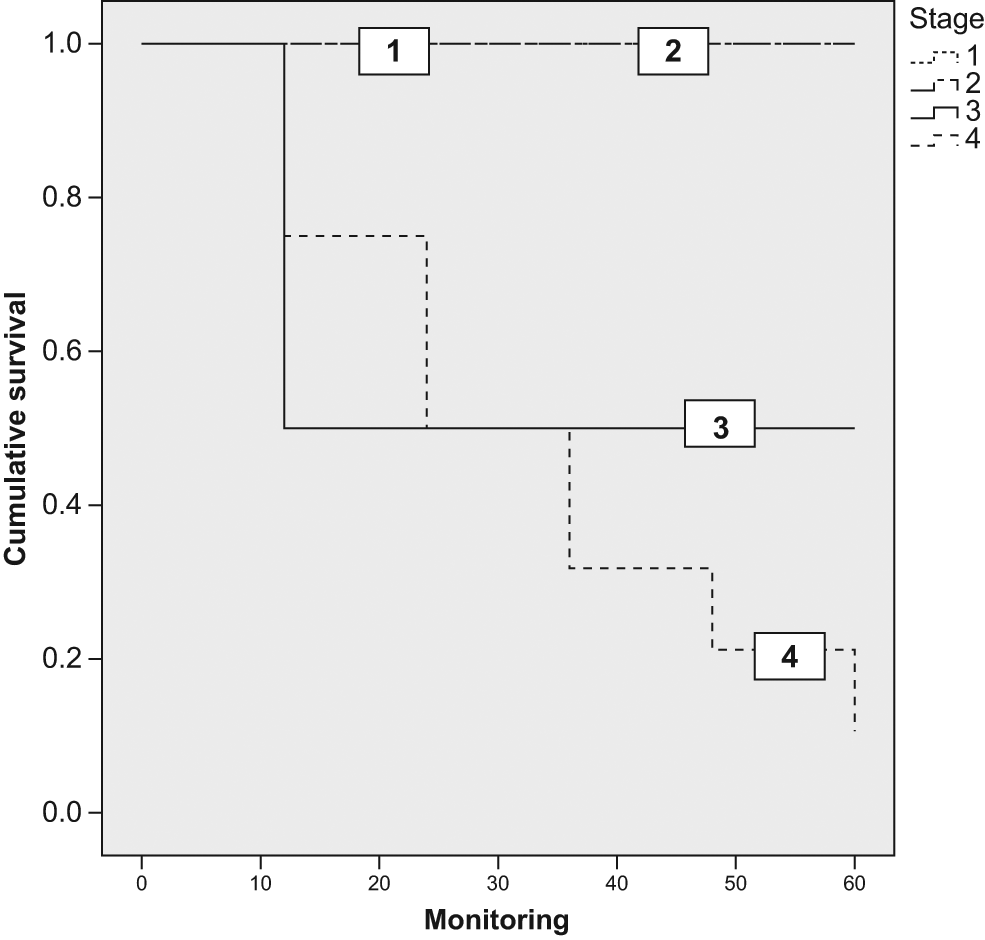
Survival function showing significantly lower survival rates for stage III and IV disease.
Discussion
Our study aims to demonstrate the significance of a small tumor in the oropharynx. Survival in oropharyngeal cancer varies according to tumor size (T1/T2 tumors are considered low risk and T3/T4 high risk), but as in other locations, it will be strongly influenced by TNM stage.15 The neoplasia studied can reach only size T1 or T2 because of its location, but the prognosis is heavily influenced by the stage of the disease. A major limitation to this work is the small sample; nevertheless, bigger samples are very difficult to gather because of the low incidence of the disease.
The difficulty in defining the exact locations of soft palate cancer by the defined limits of this region result in an underestimation of cancer of the uvula, located in a small midline unpaired structure with important prognostic implications.
It is hard to find publications referring only to carcinoma of the uvula. Most studies include them within oral cavity neoplasms. 2 In the seventh edition of the AJCC Cancer Staging Manual, 6 there are no major differences in the TNM classification of tumors of the oral cavity and oropharynx. It appears survival may change depending on the location of the tumor, and tumors that involve the midline have poorer prognosis.9,16 Despite this, most authors do not distinguish between carcinoma of the uvula and the soft palate.2,6,17
Cancer of the uvula can be diagnosed early without special techniques, even though this rapid-spreading carcinoma usually presents in advanced stages. This is why we consider it important to distinguish between cancers of the oropharynx and carcinoma of the uvula.
All patients were men with a mean age of 57.52 years, coinciding with the epidemiology of oropharyngeal cancer. 2 There is a statistically significant association between smoking and alcohol consumption and the development of carcinomas of the oropharynx. 4
Most patients presented with odynophagia and exophytic lesions microscopically consistent with moderately differentiated squamous cell carcinoma. Despite the size of lesions (all T1-T2), more than half of the patients had CLN metastases at diagnosis, of which almost half were already N2. Several publications have shown rates of nodal involvement higher than 30% in lesions of the uvula and soft palate. 9 More than 60% of our patients were stage IV at diagnosis, indicating the aggressive, fast-spreading, and thus poor prognosis of the disease.
Importantly, lesions affecting the uvula quickly reach a flush lymphatic network that spreads the neoplasia to both sides of the neck. 18 More than 80.0% of patients with metastatic CLN had lesions between 1 and 2 cm only. In addition, 13.3% of our patients had bilateral CLN metastasis possibly due to the lymphatic drainage characteristics of the uvula. Only 21.0% of patients with CLN metastasis evolved to remission. Knowing the prognosis implications of metastatic nodes, it is conceivable that carcinoma of the uvula may be an underestimated neoplasia.
Thickness of the lesion will influence the development of nodal metastasis. 19 The diameter or surface of the lesion is the available measurement of the TNM classification, even though it is not appropriate to compare it with the thickness or the depth of the tumor, which is directly related to the prognosis. 7 Statistically significant differences in our series showed that more than 90.0% of patients with lesions larger than 1 cm presented with CLN metastases.
The vast majority of nodal metastases were to level II, and almost 80.0% of patients with CLN metastasis at diagnosis died during follow-up. Of the cases, 13.3% presented with bilateral CLN metastasis at diagnosis. These statistics confirm the poor prognosis associated with the presence of CLN metastasis. With similar findings, other authors suggest the need for neck treatment in tumors of the uvula regardless of tumor size.9,20,21
Nearly 30.0% of our patients had a second primary tumor in the upper aerodigestive area during their evolution, which is almost twice that in another study. 22 Statistically significant differences demonstrate that the presence of a second neoplasm has a negative influence on the final outcome of the disease. The apparent increased susceptibility to upper aero–digestive tract neoplasms of these patients represents a therapeutic challenge. 23
In our study, more than 70.0% of patients underwent a neck dissection in the first year after diagnosis. Only 25.0% were free of metastatic disease, similar to published data on cancers of the oral cavity and oropharynx. 15 In addition, we found that about half of the cases had CLN metastasis and capsular spread, and more than 20.0% required a contralateral neck dissection. Of these, 60.0% were positive with capsular spread in 20.0%, demonstrating the aggressiveness of the disease. Almost 25.0% of all patients required a second CLN dissection within 6 months following the completion of the first surgery; 60.0% of them had tumor infiltration and up to 20.0% had node rupture.
With regard to treatment outcome, as seen with our findings, tumor staging plays a very important role. Early stage patients benefit significantly from surgical treatments with nodal dissections. However, more advanced stages seem to have little additional benefit with any treatment.
Despite a rapid initial treatment between 1 and 2 months after diagnosis, an anatomic location with a relatively easy approach, and the size of the uvula, more than half of the patients in our series showed persistence or recurrence of the disease, consistent with the natural history of other malignancies of the oral cavity and oropharynx considered aggressive. 15 The recurrence of the disease is primarily associated with disease stage.
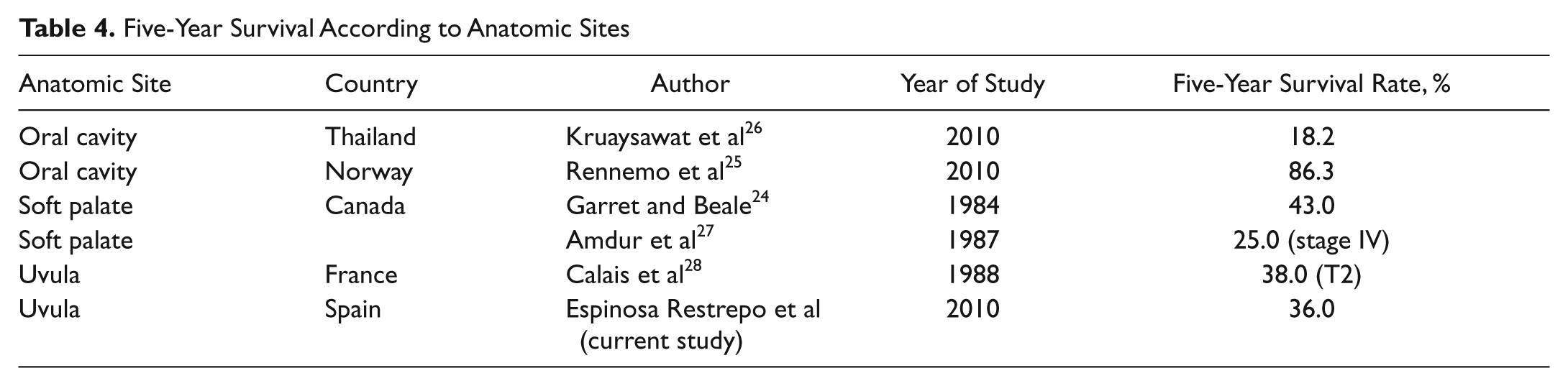
Recurrences occurred at a mean of 14 months from baseline in more than 50.0% of cases. This plays an important role in the final evolution of the disease with statistical significance according to our results. More than 65.0% of patients in our series died of the tumor directly. The average survival rate is 36% for 5 years and 18% for 10 years, with a confidence interval of 95%, similar to that reported by Garret and Beale 24 in 1984. Compared with published studies of other regions of the oral cavity, the percentages for survival can vary widely25,26 ( Table 4 ). However, the advanced stages, even for small tumors, appear to have lower survival rates.27,28
Five-Year Survival According to Anatomic Sites
Conclusion
Despite being an easily diagnosable tumor with over 60% of patients complaining of sore throat and more than 65% with exophytic lesions, squamous cell carcinoma of the uvula has a high rate (greater than 80%) of CLN metastases, although the initial size of the lesion is between 1 and 2 cm. Almost 15% of patients present with bilateral lymph node metastasis, establishing that most patients are N2 (>45%) and stage IV (>60%) at diagnosis.
With statistical evidence, we showed that the vast majority of patients with tumors larger than 1 cm presented with CLN metastases during the course of the disease.
There are insufficient data to make any conclusion about HPV and the relationship to uvula carcinoma in our study.
Early stage patients benefit significantly from treatments with nodal dissections. However, the outcomes in more advanced stages seem to occur equally among deaths and referrals, making an early diagnosis and accurate surgical treatment even more necessary.
We believe uvula carcinoma is an underestimated entity by currently available classifications. Although very small in size, tumors tend to metastasize frequently by the large lymphatic network that runs beneath the mucosa, which contributes to the tumor rarely being diagnosed at an early stage. According to our data, taking into account the prognostic significance of lymph node metastasis, we consider the clinical characteristics and evolution of uvula carcinoma as corresponding to very aggressive tumors with a rapid onset and a major negative impact on the final outcome despite tumor size at diagnosis. Therefore, in the context of head and neck oncology, we think the uvula must be considered a different subsite of the oropharynx and the treatment reevaluated, considering tumor resection and bilateral neck dissection even in early stages.
Author Contributions
Disclosures
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.