
Abstract
Background. Perineural invasion (PNI) in cutaneous squamous cell carcinoma of the head and neck (CSCCHN) is associated with decreased survival. Large-nerve PNI presents with clinical signs and symptoms and/or magnetic resonance imaging evidence of cranial nerve involvement. We sought to determine which variables predict a worse outcome and to analyze patterns of failure.
Study Design. Case series with planned data collection.
Setting. Tertiary care center.
Subjects and Methods. Patients with large-nerve PNI from CSCCHN between 1996 and 2006 were identified from a prospectively collected database. Clinical and demographic variables were recorded. Local control rates and survival analysis were performed using Kaplan-Meier curves.
Results. Thirty-six patients were identified (28 men and 8 women). The mean age was 61 years. Twenty-nine were treated with curative intent, and 7 received palliation. The mean follow-up was 35 months. Involvement of V3, disease zone, and the type of therapy were significantly associated with overall survival (P < .05). The 5-year disease-free survival for patients by therapy was 50% for subcranial surgeries, 53.6% for skull base surgery, and 0% for radiation and palliative therapies (P < .001). None of the patients treated with a skull base resection had a central recurrence, while all patients who received palliation had a central failure.
Conclusions. Disease extent, type of therapy, and involvement of V3 are all significant predictors of survival in PNI from CSCCHN. We confirmed that the natural history of the disease is central progression and that this can be halted, if detected early enough, by a properly planned skull base resection.
Keywords
The presence of perineural invasion (PNI) in cutaneous squamous cell carcinoma of the head and neck (CSCCHN) has been associated with locoregional recurrence and decreased survival in various series.1-5 There is significant confusion in the literature with regard to this entity. Histologic PNI refers to nerve invasion found incidentally following the resection of the tumor. Clinical PNI, on the other hand, refers to patients with cranial nerve deficits and/or radiologic evidence of cranial nerve invasion. The latter carries worse prognosis in CSCCHN.1,2 This distinction is important in the analysis of locoregional control and survival. Unfortunately, in the literature, it is not always clear, and these 2 patient populations are often combined when reporting results.
When the tumor invades the perineural space of a cranial nerve, it can extend proximally and/or distally in the nerve sheath and eventually reach the brainstem. Consequently, PNI may preclude obtaining tumor-free margins and/or cure. Often, patients who present with clinical PNI will have a history of a previous resection of a CSCCHN with “negative margins” and years later present with cranial nerve deficits and imaging demonstrating PNI involvement of cranial nerves and/or central nervous system (CNS) involvement; at the latter stage, it is often too late. Although this is a rare phenomenon occurring in less than 5% of cutaneous malignancies, 6 the consequences of it are devastating.
Given the heterogeneity of patient populations reported in the literature with a lack of distinction between histological and clinical PNI, and also reports combining CSCCHN and basal cell carcinoma of the head and neck (BCCHN),1,2,4,5,7 we have purged our case series to carefully analyze our experience with CSCCHN with clinical PNI diagnosed by the presence of cranial nerve deficits and radiologic evidence of cranial nerve invasion. Anecdotally, untreated patients with clinical PNI succumb to disease spread into the brainstem (ie, central failure). Our objective was to determine which variables, if any, predict a worse outcome, and to analyze the patterns of failure as they relate to the therapy received by the patient in an attempt to validate our clinical observations.
Materials and Methods
Subjects
Patients with large-nerve PNI from CSCCHN that have been assessed via the Princess Alexandra Hospital Head and Neck Tumor Board between January 1996 and 2006 were identified from a prospectively collected database. After obtaining approval from the ethics committee at our institution (research protocol 2003/197), we performed a retrospective chart review and documented the patients’ age, sex, involvement of trigeminal nerve (V1, V2, V3) and facial nerve, involvement of other cranial nerves, disease extent, histology, margins, and previous therapies.
Staging
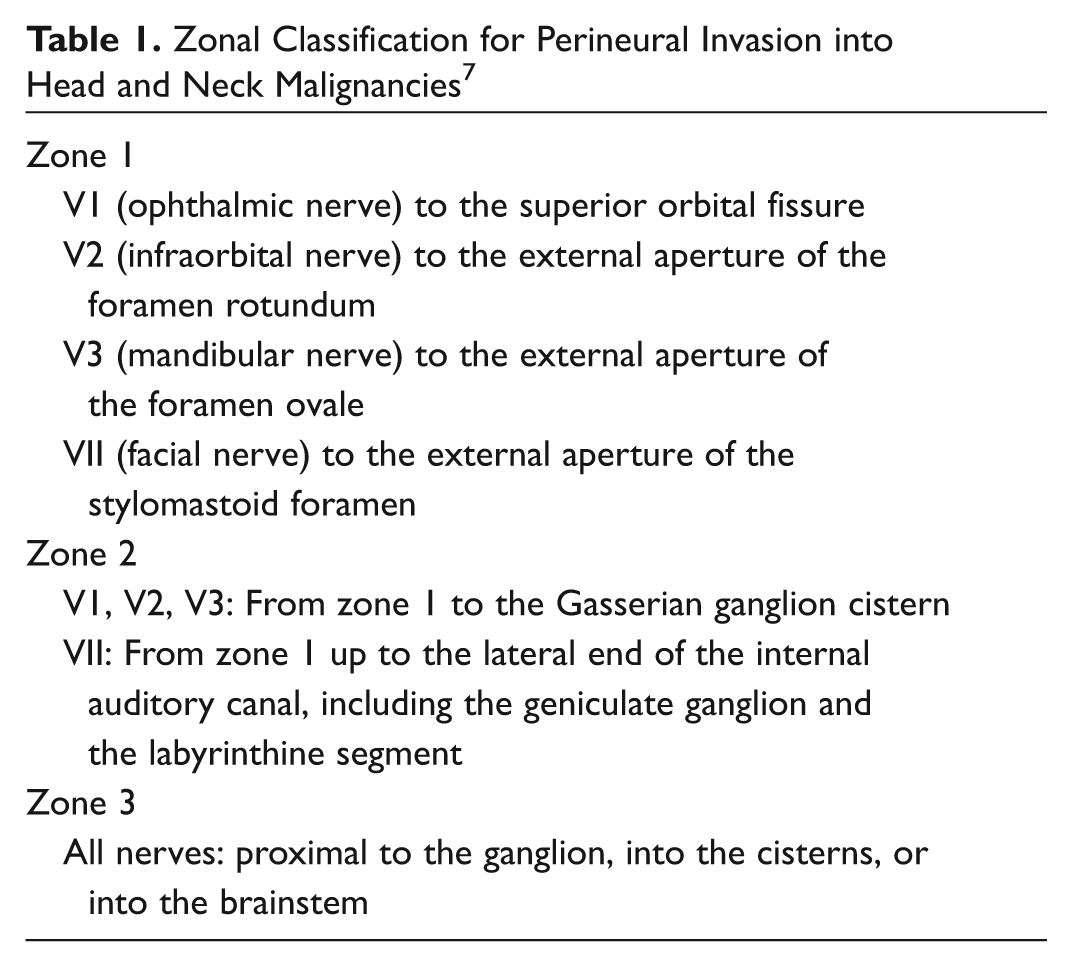
The anatomic extent of disease was defined according to a zonal classification originally described by Williams et al. 7 This classification is summarized in Table 1 . Patients were retrospectively classified blindly based on their preoperative imaging by a neuroradiologist. A higher zone indicates increased central disease progression. Surgical planning was directly related to the disease extent.
Zonal Classification for Perineural Invasion into Head and Neck Malignancies 7
Statistics
The primary outcome variable was overall survival (time to death). A set of univariate χ2 tests of association were conducted to establish the presence of any significant associations between survival, recurrence, pattern of failure, and therapy to the explanatory variables in the data set (ie, age, sex, involvement of trigeminal nerve [V1, V2, V3] and facial nerve, involvement of other cranial nerves, disease stage, histology, margins, and previous therapies). Kaplan- Meier survival analyses and plots were carried out to test for an association between survival or recurrence and the demographic and clinical variables. The log-rank test was used to test for statistical significance. The statistical analysis was performed with SAS version 11.1 software.
Results
Thirty-six patients with large-nerve PNI from CSCCHN were identified from the database. The mean age was 61 years (range, 38-86 years). There were 28 men and 8 women. Seventy-two percent of patients presented with cranial nerve deficits and a previous history of a small (ie, T1) CSCCHN; the remainder presented with large-nerve PNI and a soft-tissue mass (ie, T4). Of these, 29 were treated with curative intent: 5 patients received radiotherapy alone with curative intent with doses ranging from 64 Gy to 70 Gy in 32 to 35 fractions, 5 patients were treated with subcranial resection, 3 of which were not treated by the senior author (BP) and not designed to fully encompass the radiological extent of the disease, and 19 patients had skull base resections. Of the surgical patients, 4 patients could not receive additional radiation therapy, and the remainder were treated with postoperative radiotherapy with doses ranging from 56 Gy to 63 Gy in 28 to 30 fractions. The remaining 7 patients received palliative therapies. The median follow-up was 19 months, and the mean follow-up was 35 months. Overall, there were 17 deaths, with 15 of these being disease specific. There were 22 recurrences among 20 patients, with 12 being central, 3 regional, and 7 local. In total, 21 patients had a recurrence or death. There were no cases of distant metastasis.
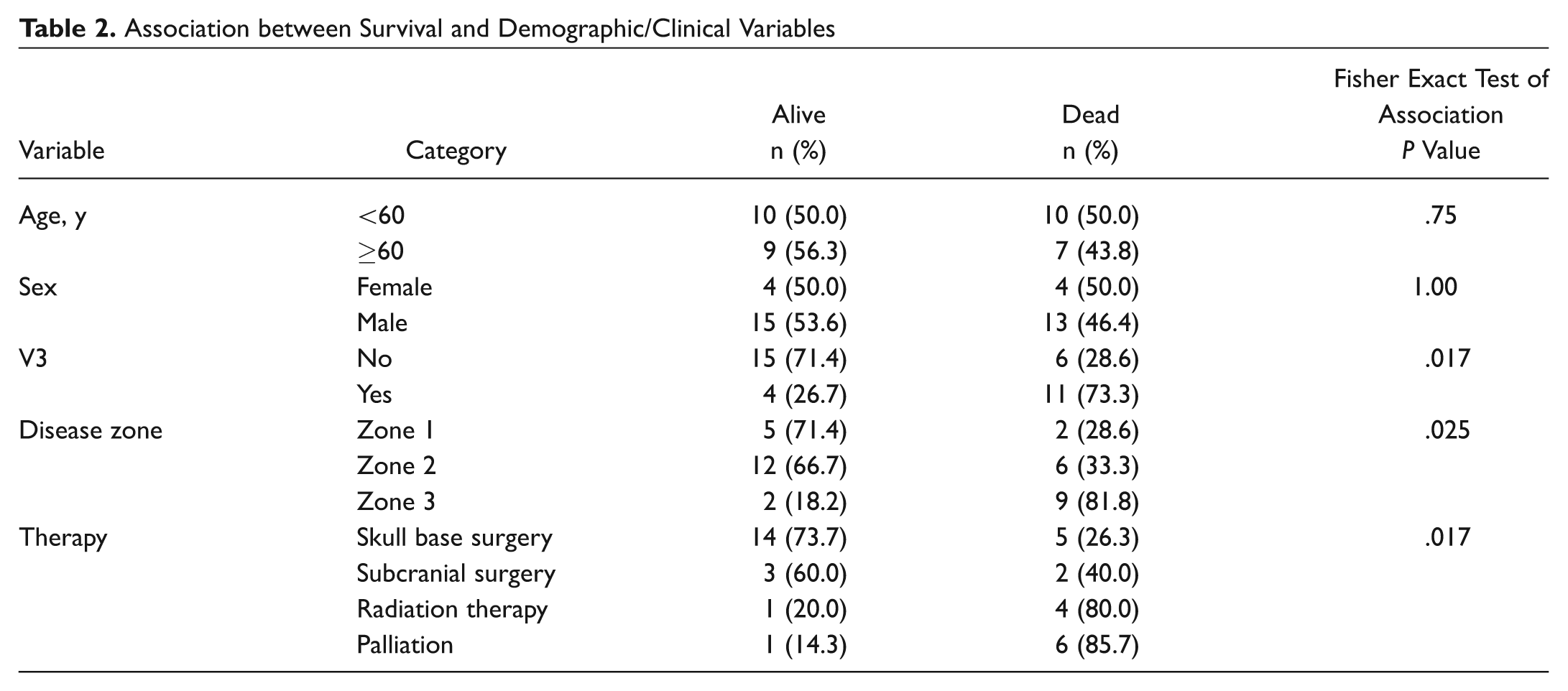
Involvement of V3, disease zone, and the type of therapy given to the patient were all statistically significantly associated with overall survival and rate of recurrence (P < .05). Those that were diagnosed as having involvement of V3 had a lower survival status (−26.7%) compared with 71.4% without involvement ( Table 2 ). As a result, those patients had a much lower survival curve and lower median survival (15 months) compared with those who did not have V3 involved in their disease (median, 90 months; P < .001). The 5-year survival rates for patients with and without V3 involvement were 80.4% and 16.3%, respectively ( Figure 1 ).
Association between Survival and Demographic/Clinical Variables
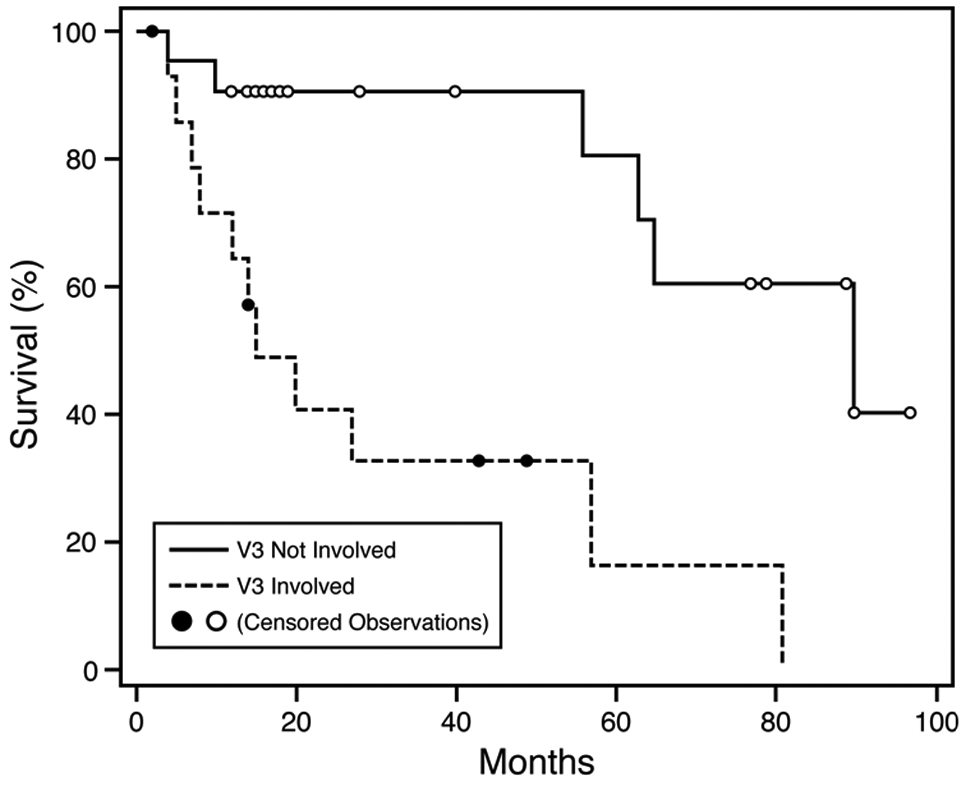
Kaplan-Meier survival curves classified by V3 involvement (P < .001).
Patients with zone 3 disease were less likely to survive (18.2%), whereas those with less advanced stages were more likely to survive (71.4% and 66.7%) for zone 1 and 2 disease, respectively ( Table 2 ). The median survival time among patients with zone 3 disease was 11 months, while patients with zone 1 and 2 disease survived a median of 81 and 90 months, respectively. The 5-year survival rates were 85.7%, 64.4%, and 20% for zones 1, 2, and 3, respectively ( Figure 2 ).
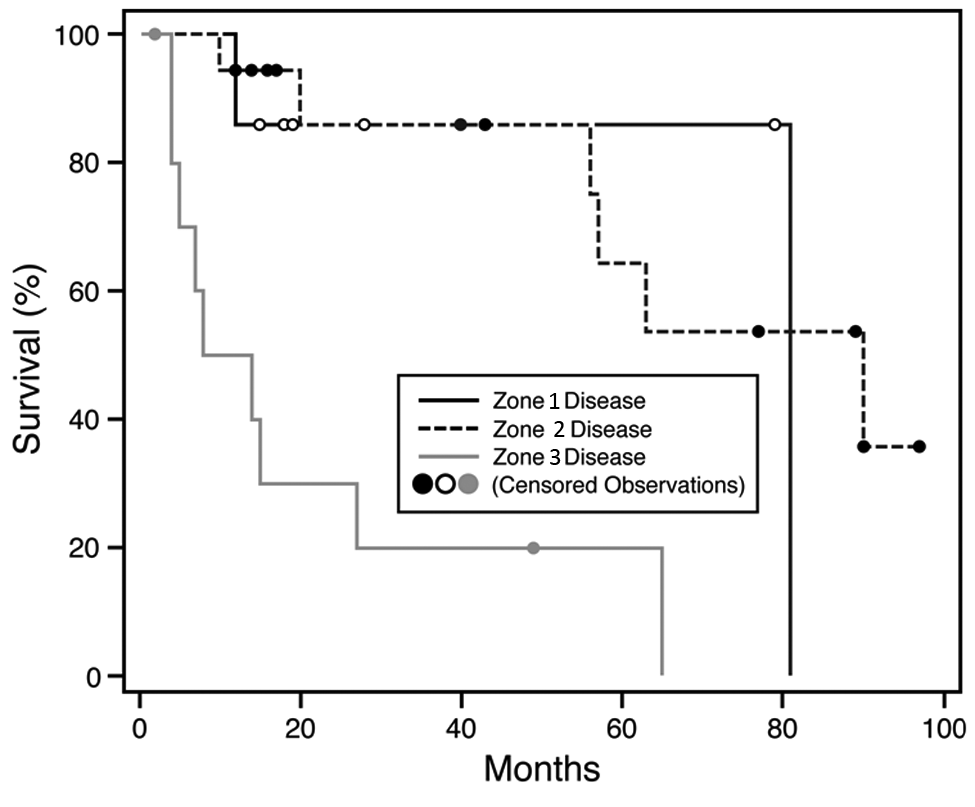
Kaplan-Meier survival curves classified by disease zones (P < .001).
The 5-year disease-free survival for patients according to different therapies was 50% for subcranial surgeries, 53.6% for skull base surgery, and 0% for radiation and palliative therapies (P < .001; Figure 3 ). Few patients who underwent radiotherapy alone with curative intent (20%) and patients characterized as being palliative (14.3%) survived, while those who underwent some form of surgery were more likely to survive (73.7% for skull base surgery and 60% for subcranial surgeries; P = .017; Table 2 ). Removal of the palliative group deemed the association between survival and therapy as nonsignificant. After excluding patients treated with palliative intent, V3 involvement remained significantly associated with survival, with a 56.4% versus 0% 5-year survival. There were no significant associations between survival and the remaining demographic and clinical variables (P = .19-1.0).
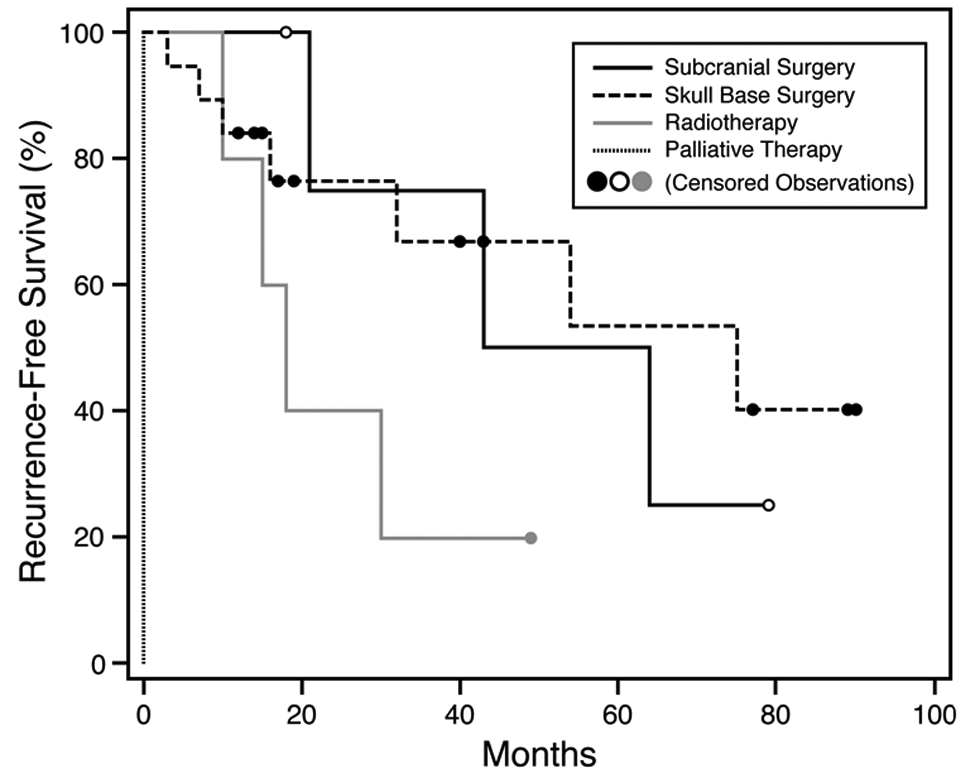
Kaplan-Meier recurrence-free survival curves classified by type of therapy (P < .001).
V3 involvement and disease status were significantly associated with the type of therapy rendered to the patient (P = .004 and <.001; Table 3 ). Most patients defined as palliative (6/7) had V3 involvement. Far fewer patients with known V3 involvement had surgery (26.7% had a skull base resection and 6.7% had subcranial surgery) compared with those without involvement (71.4% had a skull base resection and 19.0% had subcranial surgery). Eighty percent (4/5) of patients undergoing radiotherapy had V3 nerve involvement. There was no significant association between therapy and the other demographic and clinical variables (P = .12-1.0).
Association between Therapy and Demographic/Clinical Variables
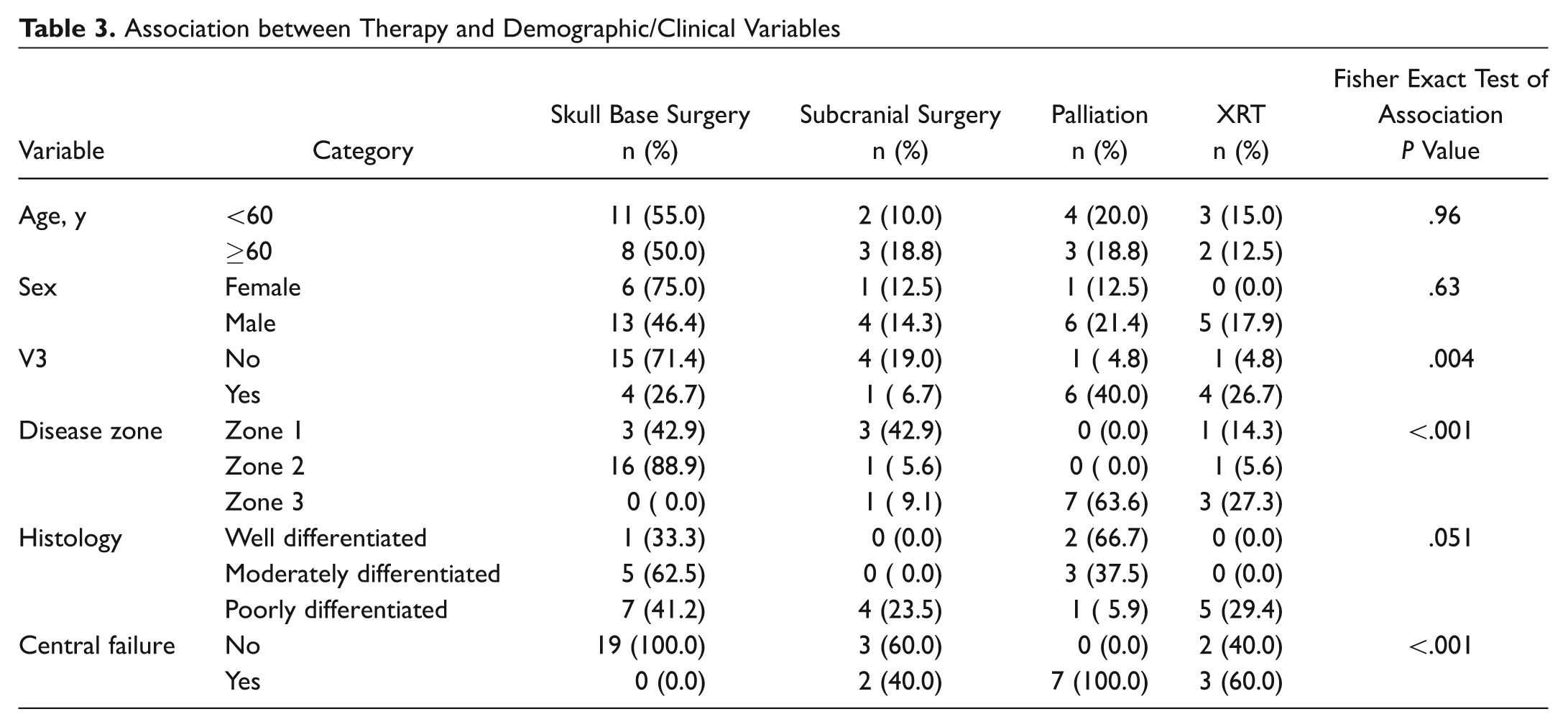
Central failure was significantly associated with the type of therapy overall (P < .001; Table 3 ). Patients who had subcranial surgery or radiation therapy had a similar likelihood of having a central recurrent event, while none of the patients treated with a skull base resection had a central recurrence. All patients who received palliative treatment had a central failure. Although none of the patients with skull base surgery had a central failure, 26.3% (5/19) had a peripheral recurrence. On the other hand, patients undergoing radiotherapy or subcranial surgery were equally likely to have a peripheral recurrent event (1 case in each group).
Discussion
The present study demonstrated that in CSCCHN with clinical PNI disease extent (ie, zones involved), type of therapy and involvement of V3 were significantly associated with the overall survival rate and rate of recurrence. The involvement of V3 remained significant after eliminating palliative patients. The type of therapy was significantly related to the disease extent and involvement of V3. In other words, therapy was driven by the extent of disease, and V3 involvement correlated with more extensive disease. In addition, this study confirms our clinical observations that patients with clinical PNI succumb to disease spread into the brainstem (ie, central failure). This is supported by the lack of central recurrence in patients who underwent a skull base resection with negative margins in contraposition to an increased rate of central disease progression in patients who did not have surgery (ie, primary radiation and palliative patients). Interestingly, an increased rate of peripheral failure, although not significant, was noted in patients who underwent a skull base resection, suggesting an alteration in the natural history of the disease. This study is limited by a small sample size, which precludes detailed multivariate statistical analysis; however, this limitation is inherent to the rarity of this disease process.
PNI in CSCCHN is a poorly understood entity. Little is known about the tumor biology that drives the neurotropic behavior.8,9 In addition, significant misunderstanding among clinicians exists with regard to the clinical behavior of large-nerve or clinical PNI versus incidental or histologic PNI. Clinical PNI occurs when a named branch of a cranial nerve is invaded and this invasion can be visualized on magnetic resonance imaging (MRI). 10 These patients present with neurologic deficits related to the affected nerve. Histologic or incidental PNI, on the other hand, occurs when nerve invasion is found incidentally on a surgical specimen. The literature shows that clinical PNI carries significantly worse prognosis.1,2 McCord et al reported on 62 patients with clinical PNI from cutaneous squamous and basal cell carcinoma of the head and neck and compared them with patients with incidentally found PNI. The survival was significantly decreased in patients with clinical PNI when compared with those with incidental PNI. While this study demonstrated a worse outcome for those patients with clinical PNI, only 23 patients (both squamous cell carcinoma and basal cell carcinoma) had radiologic evidence of nerve involvement, making it difficult to compare them with our patient population. 1
Our treatment philosophy is based on the anatomic extent of PNI along the cranial nerve. In our practice, extension beyond the boundaries of the Gasserian (V) or Geniculate (VII) ganglia usually deems the patient to be inoperable (attributed to the possibility of the tumor transgressing dural margins and the concern of potential subarachnoid seeding). Patients with anatomically operable disease who cannot withstand an operation for medical reasons undergo radiation therapy. Williams et al 7 described a zoning system to classify the extent of PNI. We retrospectively classified our patients based on this zoning system. Given that zone 3 disease corresponds to our criteria of inoperability, it is no surprise that the disease extent was a predictor of poor outcome and significantly related to the type of therapy. In other words, patients with a more advanced stage were less likely to have surgery, and patients who did not have surgery had a worse prognosis. V3 involvement was a predictor of poor outcome, and this was likely related to more advanced disease at presentation in this group of patients, as evidenced by a direct correlation between advanced disease and V3 involvement.
In a landmark study by Goepfert et al 11 that reviewed 520 patients with CSCCHN, 14% were found to have PNI. While a 14% incidence of PNI seems high, this reflects the referral bias of a tertiary care center. It is not clear from the study how many patients had incidental versus clinical PNI. Importantly, however, the authors noted that patients found to have PNI had an increased incidence of CNS involvement. The authors advocated aggressive surgical resection followed by radiation therapy. In 6 patients, a skull base resection was performed, and 2 of those patients were alive at last follow-up. Similar to the findings of Goepfert et al, it has been our clinical observation that patients with large-nerve PNI fail centrally. Our study confirms these anecdotal observations, as demonstrated by a 100% central failure rate in those patients who received palliative therapy. Importantly, a skull base resection with negative margins plus or minus postoperative radiotherapy was able to stop the natural progression of the disease, as evidenced by a 0% central failure rate, while more peripheral failures were observed. Overall, patients who did not have surgery were more likely to experience a central failure, suggesting that the only effective way to stop the central disease progression is to physically remove the nerve involved with clear margins.
Conclusion
In conclusion, we have reviewed our experience with large-nerve PNI as defined by cranial nerve deficits and MRI evidence of nerve involvement. We found that disease extent, type of therapy, and involvement of V3 were all significantly related to survival. Involvement of V3 was an independent predictor of survival. We confirmed our anecdotal observations that the natural history of the disease is central progression and that this can be halted by a properly planned skull base resection at the expense of an increased rate of peripheral recurrences some years later.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.