
Abstract
Objective. To evaluate the safety of tonsillectomy in a short-term medical mission setting.
Study Design. Retrospective chart review.
Setting. Catholic mission hospital in Guatemala.
Subjects and Methods. During 7 consecutive annual mission trips from 2004 to 2010, patients received tonsillectomy and adenotonsillectomy. Established safety protocol requires candidates for tonsillectomy to agree to stay within 1 hour of the hospital for 10 days following the operation. This study includes all tonsillectomy patients regardless of age or indication for tonsillectomy. The primary outcome measures include posttonsillectomy hemorrhage, nasopharyngeal reflux, readmission for dehydration, and mortality. This is a novel study as the work performed by most short-term medical missions is unregulated and unevaluated.
Results. Medical charts were available for 197 (96.6%) of the 204 patients receiving tonsillectomy in the 7-year period; this was the only inclusion criterion. Ninety-nine (50.3%) patients had tonsillectomy concomitantly with adenoidectomy. Patients ranged in age from 3 to 66 years. The mean (SD) age was 17.2 (14.0) years. The study team found documentation of postoperative complications in 3 (1.5%) patients; 2 experienced postoperative hemorrhage, 1 within the first postoperative hour and 1 at 96 hours. The final patient returned to the hospital within 24 hours symptomatic for dehydration.
Conclusions. The authors have evaluated a protocol for tonsillectomy patients in a specific setting and believe their data represent satisfactory outcomes for the reviewed patients. The generalizability of this information is uncertain, but safety protocols should be established on all short-term medical missions to prevent untoward complications.
Keywords
Our institution, a tertiary care university hospital, has established a relationship with a US-based medical mission organization. Since 2003, we have annually participated in a short-term medical mission (STMM) to Antigua, Guatemala. The trip includes surgical, medical, and audiological services. All of the surgeries occur in a Catholic mission hospital, Obras Socíales del Hermano Pedro, which serves patients from across the country regardless of their ability to pay. Tonsillectomy is one of the surgical procedures provided by our team. Our primary aim for this study is to retrospectively evaluate the safety of this procedure in this setting and assess the safety protocol we have in place to prevent mortality from posttonsillectomy complications. This is a novel study as the work performed by many STMMs is unregulated and unevaluated.
Tonsillectomy in STMM
Short-term medical missions are solely self-regulated, but ethical standards require that providers provide quality care to patients and follow the practice guidelines under which they typically operate.1-4 Tonsillectomy is among the most commonly performed major surgical procedures in children globally. 5 Publications from the late 1980s to the mid-1990s explore the safety of tonsillectomy and adenoidectomy as outpatient procedures.5-7 The predominant controversy surrounds the risk of postoperative hemorrhage. The proportion of patients reportedly experiencing hemorrhage secondary to tonsillectomy varies considerably in the literature, ranging from 0.8% to 30%. 8 In the Alexander et al 8 study, the majority (69.8%) of cases experiencing postoperative hemorrhage returned to the hospital between postoperative days 4 and 7, with the range being 2 to 15 days. These results were comparable to the results of previous studies. 8
In most cases, developing nations do not have timely access to quality emergency care. Emergency care provides a safety net to reduce morbidity and mortality from postoperative complications. Providing surgical care in developing nations requires consideration of this limitation. In the English literature, there is no known justification or description of the safety of tonsillectomy in a developing nation as a part of a STMM. There are, however, several studies in the plastic surgery literature describing the necessary components of high-quality surgical missions, including patient screening and follow-up recommendations.9,10 Unfortunately, those studies do not include any data evaluating the efficacy of these recommendations. Our intention for this study is to present our experience with tonsillectomy outcomes among patients operated on during an STMM and thus justify its safety when accompanied by a safety protocol and advocate for establishment of safety protocols in other STMMs.
Methods
Setting
Obras has an inpatient ward with a limited number of beds. Patients who are able must be discharged to make room for the surgical patients from the following day. For those patients who need to remain close but do not need full hospital services and are unable to afford hotel accommodations, Obras provides access to an alternative. Casa de Fé is a separate, local, dormitory-style residence providing lodging and 1 meal per day for Obras patients, free of charge.
Currently, Obras is able to provide outpatient care in general medicine and some specialties. Two doctors serve as full-time staff and see approximately 80 patients per day, providing general health care and identifying surgical candidates for surgeons who run specialty clinics on a limited basis. The hospital relies on volunteer groups to add to the spectrum of care. Each year, over 175,000 underpriviledged individuals access medical care at Obras. The hospital does not have access to otolaryngic care regularly. Several teams of physicians from different nations visit each year and provide this otolaryngic care. Our team provides numerous surgical procedures, and for the past 7 years, these services have included tonsillectomy.
From 2004 to 2010, otolaryngologist members of our mission teams performed tonsillectomy on 204 patients at Obras. Each team ranges in size from approximately 55 to 70 volunteers. Included in the teams are otolaryngologists, anesthesiologists, nurse anesthetists, pharmacists, audiologists, nurses, photographers, and students. All of these otolaryngologists are currently practicing in the United States, and most operate in an academic setting. Senior otolaryngology residents also participate in these trips and operate under the same supervised conditions required by their home institution. The institutional review board at our home institution and the administration of the Obras Socíales del Hermano Pedro Hospital approved this study.
Surgical Candidacy and Safety Protocol
All potential tonsillectomy patients see the surgeon, who determines surgical candidacy in a clinical setting. Local primary care providers screen these patients before appointments in the otolaryngology clinic are made. The diagnosis of recurrent tonsillitis was the most common diagnosis. As cultures are not common in developing nations, we used criteria of multiple infections with associated fever, pain, and treatment with antibiotics to determine severity of the infections. Sleep-disordered breathing was the second most common diagnosis. No sleep studies were available for these patients, so this was based only on family report. Patients were screened by anesthesia and were required to be ASA (American Society of Anesthesiology) status 1 or 2 before scheduling. Patients whose ASA status was 3 or over were not scheduled for surgery. Translators or Spanish-speaking team members are present in every meeting with patients and their family members. Mission team members explain potential complications and offer patients and their families the opportunity to ask any questions.
The scheduling team asks the patient or their family about the distance from their home to Obras. The team then informs patients and their families that our safety protocol requires that they remain within 1 hour of the hospital for at least 10 postoperative days and return to the hospital immediately if the patient begins to bleed, as this complication could be fatal if left untreated. Casa de Fé, as previously discussed, is available for patients and 1 family member to stay free of charge if they live more than 1 hour by available means of transportation (car, public transportation, or on foot) from the hospital. If the family refuses or is unable to stay in town for that duration of time, the surgery is not scheduled. All patients are required by the hospital to have screening blood work, which includes a complete blood count (CBC) and platelet count, as anemia is fairly common because of poor nutrition. The mission team will not approve surgery for patients whose blood counts are low. Tonsillectomy procedures are performed primarily on the first day of surgery, with a few patients on the second day. The patients who live the farthest away are done on the first day, leaving the second day for patients who live locally.
The operating facilities at Obras are similar to those in developed nations. There are 4 well-equipped operating suites. All disposable equipment has been brought from the United States, as well as most of the tonsil equipment trays. Donated Valley laboratory bovie units are present in each operative suite. A Central American representative from Arthrocare delivered the donated coblator units to us in Guatemala.
The procedures are performed under general anesthesia provided by our anesthesia team. Inhalational medications (sevoflurane) and most intravenous (IV) medications are brought into the country by our team. Narcotics used during the procedures are purchased from the pharmacy at the Obras because of local policies that prevent mission teams from bringing these medications into the country. Postoperative pain medications for the patients are primarily nonnarcotics, with acetaminophen being the most common medication used.
After surgery, all patients are required to spend the first night in the hospital under the care of nursing assistants and 1 supervising nurse. On the postoperative wards, there are no patient monitors. The nursing staff continues IV fluids on the floor, but there is no rate control available. During the past 2 years of data collection, an intensive care unit has been available for the most ill patients. These 3 beds have both cardiac and saturation monitoring.
The mission team and hospital staff discharge most patients home or to Casa de Fé the following day. The surgical team has members who stay in the area for at least 7 days after the tonsillectomy procedures to capture as many of the postoperative complications during the standard risk window. 8 General surgeons, as well as general surgical residents, who are on call at the hospital 24 hours a day, are trained each year to handle posttonsillectomy hemorrhage should it occur after the team leaves. The hospital has un-cross-matched blood available for emergencies.
Chart Review
Surgical logbooks maintained by the Obras staff list all procedures performed at the hospital by mission teams and the patient names. The primary author created a list of tonsillectomy patients for each year and reviewed the charts. Mission team members create a postoperative English chart similar to those at US institutions. These charts include details about perioperative complications, including hemorrhage, complications from anesthesia, or any other noted surgical complication. Electronic versions of this record are available for patients beginning in 2007. In addition, the primary author reviewed the full Spanish medical chart maintained by Obras in search of delayed postoperative complications, including secondary hemorrhage, readmission for dehydration, mortality, or any other delayed complication. The authors performed statistical analyses using SPSS 18.0 (SPSS, Inc, an IBM Company, Chicago, Illinois).
Results
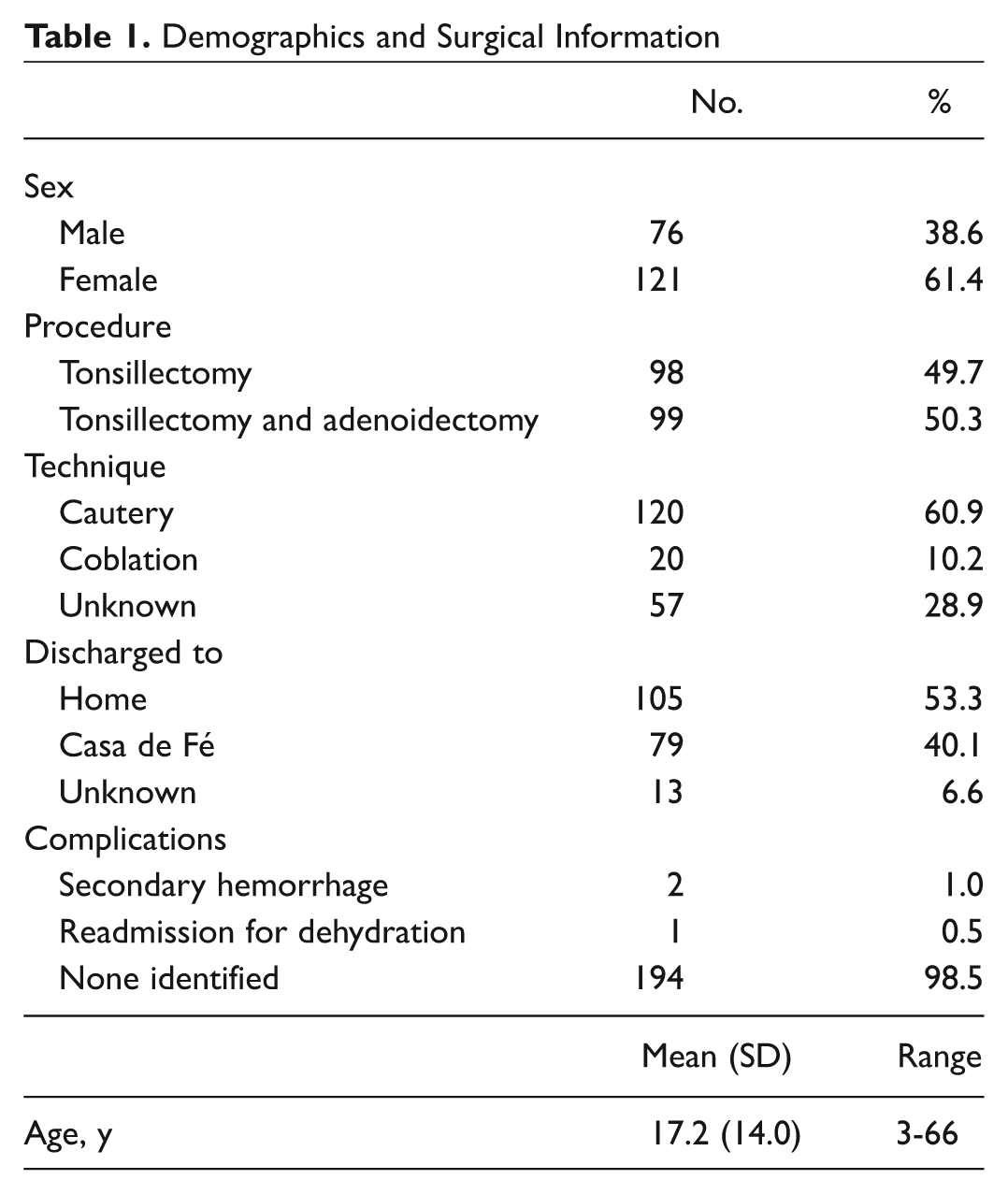
Medical charts were available for 197 (96.6%) of the 204 identified patients; this was the only inclusion criterion for this study. Among the included patients, 99 (50.3%) received tonsillectomy concomitantly with adenoidectomy. Table 1 presents the demographics and basic surgical information for the study population. The study sample included 121 females (61.4%) and 76 males (38.6%). Patients ranged in age from 3 to 66 years old. The mean (SD) age was 17.2 years (14.0 years; median, 11 years) old. Two-thirds (130) of the study population were younger than 18 years at the time of surgery. The number of tonsillectomy procedures performed annually fluctuated mildly, ranging from 16 to 36 cases per year with a median (interquartile range [IQR]) of 29 (9).
Demographics and Surgical Information
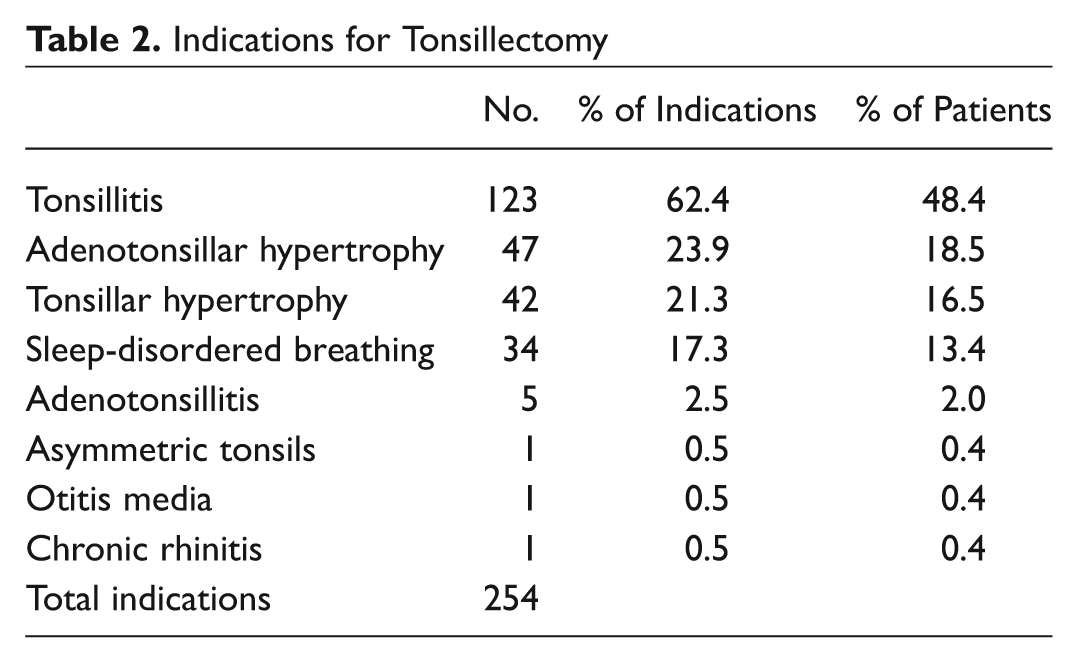
Data collection resulted in 254 total indications for tonsillectomy or adenotonsillectomy; however, the denominator for calculated proportions is 197 patients ( Table 2 ). The most commonly identified indication was tonsillitis with 123 (62.4%) patients, respectively. Forty-seven (23.9%) patients exhibited signs of adenotonsillar hypertrophy. Surgeons noted sleep-disordered breathing and/or tonsillar hypertrophy as the surgical indication for 76 patients (38.6%) and adenotonsillitis in only 5 (2.5%). The least commonly noted indications were asymmetric tonsils, otitis media, and chronic rhinitis, appearing only 1 (0.5%) time each.
Indications for Tonsillectomy
Specific surgical technique for the tonsillectomy or adenotonsillectomy was available for 140 (71%) patients. Cautery was by far the most common technique, employed for 120 (60.9%) patients. The remaining 20 patients received a tonsillectomy by coblation. The staff released 105 (53.3%) patients from the hospital to go home and 79 (40.1%) to Casa de Fé; 13 (6.6%) patients did not have this information recorded. According to our established safety protocol, patients must live within 1 hour of the hospital to go home rather than to Casa de Fé.
During the 7-year period under review, the study team found documentation of postoperative complications in 3 (1.5%) patients. One of these patients experienced postoperative hemorrhage within the first postoperative hour. One experienced postoperative hemorrhage at 96 hours; this patient reported aspirin use for pain management throughout the postoperative period leading up to the hemorrhage. The final patient returned to the hospital within 24 hours symptomatic for dehydration. The mission team managed all of these complications, and all resolved without sequelae. The review of the medical records revealed no other complications.
Discussion
The primary concern in tonsil surgery is postoperative bleeding, and the need for emergency care because of this bleeding to prevent mortality is possible. 5 For that reason, some STMM organizers may choose to avoid this procedure. The risk is unknown in the populations served by these STMMs, but there is no documented divergence from the expected rate of hemorrhage in the international literature.5,6,11 The need for this procedure, as documented by the increasing demand per year, remains, and considerations for the risk of complications must be weighed against the potential benefits for the patients. Our rate of secondary hemorrhage, 1%, falls within the published range (0.8%-30%). 8 Although our data do not include a direct comparison of the rate of hemorrhage in our Guatamala STMM with that of developed countries or STMMs in other locations, we suggest that the rate we observed is within an acceptable range for risk. The binomial exact 95% confidence interval for our rate is 0.1% to 3.6%, which falls largely within the published rates. Treatment for all complications succeeded without further sequelae.
Data collection for a STMM is challenging, and we recognize the limitations of its retrospective nature in our study. The distances that some patients travel to receive this care complicates our ability to ensure we have collected all of the complications experienced by our patients. Some may have sought treatment at the other private hospital in Antigua or a public hospital closer to their home. We are relatively certain that we captured all of the complications of patients returning to Obras, but there is a possibility that the 7 patients without locatable charts could have experienced complications. There are obvious limitations to our ability to require that patients remain at Casa de Fé, and patients who live close to a medical provider may feel comfortable leaving prior to the 10th postoperative day. There is the additional possibility that patients may return home after 10 days and experience secondary hemorrhage after that time. Although it is less likely based on previously published reports, the bleeding window may extend beyond this range. 8
Despite these limitations, our annual presence and the relationship established with Obras and the community lead us to believe that patients would notify either the staff at Obras or our staff of any severe complications. There is also documentation in many of the charts of follow-up visits with the full-time staff at Obras after the team’s departure; all of these return visits indicate that the patients are doing well and experienced no complications. During our time in Guatemala, we have heard numerous stories of families operated on returning later to Obras to see the permanent staff and requesting that another child or family member have the same operation. Obviously, this does not provide assurance of complete data; however, it does indicate a level of trust for Obras and, to some degree, our teams. Complications would compromise this trust and prevent patients from returning. Previous studies evaluating the incidence of secondary hemorrhage rely on self-reported treatment by surgeons, which has many of the same limitations we have identified. 6 Varying definitions of secondary hemorrhage also make comparisons across studies difficult. 8
Conclusions
Our experience indicates that there is a need for tonsillectomy in the developing nations served by STMMs. There is concern about long-term safety of all surgical procedures performed on STMMs, especially after the team leaves the country. We have established a protocol for this procedure in the setting under which we operate and feel that the data presented here represent satisfactory outcomes given some limitations on the collection of follow-up data. The potential severity of postoperative hemorrhage is concerning, but we believe that in the setting under which we operate in Guatemala with an adequate safety protocol in addition to patient and family counseling, tonsillectomy has been safely performed. The generalizability of this information is uncertain, but we would suggest that STMM directors and volunteers should establish safety protocols, such as ours, for all STMMs and subsequently evaluate them to prevent and detect untoward complications in developing nations.
Considerations for Future Research
Prospective data collection regarding our tonsillectomy patients and their outcomes could present a slightly different picture of the safety of this procedure in this setting. Performing active follow-up with these patients would require time beyond the standard STMM or the participation of local study team members but could include clinical outcomes measurement following tonsillectomy. This may be the next logical step for this study, but additional questions arise when we consider the often-unmeasured impact of STMMs. This impact could include negative economic impact on local physicians, positive impact on the overall health of the community, or even little impact on any aspect of the community served. More research is necessary to understand the impact of STMMs and to understand the outcomes of the services they provide, particularly as they relate to cost-benefit analysis and quality of care. Understanding the interaction between foreign physicians and the patients they serve in STMMs could provide interesting insight into the patient and family comprehension of risks and benefits of the treatments offered. In addition, evaluating the use of explanatory materials and their impact on this comprehension could alter the way preoperative counseling occurs for STMM. Finally, understanding what needs the community would self-identify as the most significant needs may provide a larger positive impact for the economic investment made by STMM organizations.
Author Contributions
Disclosures
Footnotes
Acknowledgements
The authors thank Dr Claudio Gonzalez; all of the staff at Asociación Obras Sociales del Santo Hermano Pedro in Antigua, Guatemala; and Medical Missions Foundation for their assistance and support of this research.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.