
Abstract
Objective
To examine the sources of litigation related to the practice of head and neck surgery.
Study Design
Analysis of malpractice claims directly related to the diagnosis and treatment of head and neck disease provided by 16 medical liability insurance companies.
Setting
Not applicable.
Subjects and Methods
Data were obtained from 16 members of the Physician Insurers Association of America. All claims were either filed or closed between 1978 and 2007. Claims were evaluated for patient age, the cause for the claim, any surgical complications, and indemnity paid.
Results
Three hundred fifteen claims were identified between 1978 and 2007. The mean patient age was 48 years (median, 47 years). The greatest number of claims came from the 36- to 45-years age group (n = 68, 24.6%). Perioperative complications represented the largest cause of claims (n = 169, 53.7%), followed by delay of or missed diagnosis (n = 109, 34.6%) and persistence or recurrence of disease (n = 21, 6.7%). Among perioperative complications, nerve injuries were the largest group (n = 64, 20.3%), followed by airway-related claims (n = 27, 8.6%), esophageal injuries (n = 14, 4.4%), poor cosmetic results (n = 14, 4.4%), vessel injuries (n = 11, 3.5%), and postoperative infections (n = 2, 0.6%). Overall, mortalities resulted in 62 (19.7%) claims.
Conclusions
Four important risks for malpractice litigation in head and neck surgery were identified: young patient age, perioperative complications, delay of or missed diagnosis, and persistence or recurrence of disease.
Keywords
Otolaryngologists play a central role in the treatment of diseases of the head and neck, from screening through long-term follow-up and surveillance. The complications and poor outcomes that may arise during this process are well documented, and in most cases, these outcomes are not the result of medical negligence but a result of the disease process despite our greatest efforts. With this in mind, however, injury due to medical error does occur and periodically leads to medical malpractice tort actions. The efficacy of this system is often debated and is not the focus of this report. It has been noted that most medical malpractice lawsuits do involve injury as a result of medical error. It has furthermore been suggested that nearly three-quarters of the time, the outcomes of these lawsuits are concordant with their merit. 1
Litigation analysis and physician education have been described as important methods of reducing the number of malpractice claims.2-9 Most of these reports, including all of those for the head and neck,3-10 are based on verdict summary analysis from legal databases (Westlaw, LexisNexis). The summaries included in these databases are those that attorneys evaluate for precedents, summary content, verdict outcomes, and size of judgments. 8 Suits that are settled or dropped without going to court are not included in these databases.8,10
To further understand the litigation trends in head and neck surgery, the current study seeks to analyze malpractice claims using data collected by medical liability insurance companies. These data include all claims filed, including those dropped or settled out of court. This report should aid physicians involved in the care of patients with disorders of the head and neck in risk management and prevention strategies.
Methods
Sixteen medical liability insurance companies—members of the Physician Insurers Association of America (PIAA)—provided data for malpractice claims related to head and neck surgery. These 16 companies represent 27% of the 60 member companies of PIAA covering physicians in all 50 states. The 60 member companies of the PIAA provide medical malpractice protection to more than 60% of America’s private practice physicians and are responsible for approximately 46% of the total industry premium. All claims were either filed or closed between 1978 and 2007 and include those claims settled or dropped without going to trial. Claims were included if they were related to the practice of head and neck surgery including but not limited to cancer.
Information extracted from these data includes the outcome resulting in the claim, procedure performed, and whether or not the claim was related to a mortality. Also available was the age and sex of the plaintiff and any indemnity received. Claims resulting from delayed/missed diagnosis, persistence/recurrence of disease, and perioperative complications were analyzed separately. The terms delay in diagnosis and missed diagnosis are used interchangeably throughout this data set and for analysis purposes will be considered the same. In a similar way, both persistence and recurrence of disease from a plaintiff standpoint represent a failure of treatment and will be considered one group in this review. Analysis was also made for claims resulting specifically from surgical complications and those related to mortalities. Approval was not required for this study by the Vanderbilt University Institutional Review Board.
Results
Of 1324 malpractice claims related to the practice of otolaryngology–head and neck surgery, 315 (23.8%) claims were identified that met the criteria ( Table 1 ). The plaintiffs had a mean age of 48 years and a median age of 47 years. The age group that brought the largest number of malpractice claims was aged 36 to 45 years with 68 (24.6%) suits ( Table 1 ). This group was followed by ages 46 to 55 years, 63 (22.7%); 56 to 65 years, 54 (19.5%); 26 to 35 years, 36 (13%); 66 to 75 years, 25 (9%); 17 to 25 years, 20 (7.2%); and greater than 75 years with 11 (4%) claims.
Head and Neck Malpractice Claims
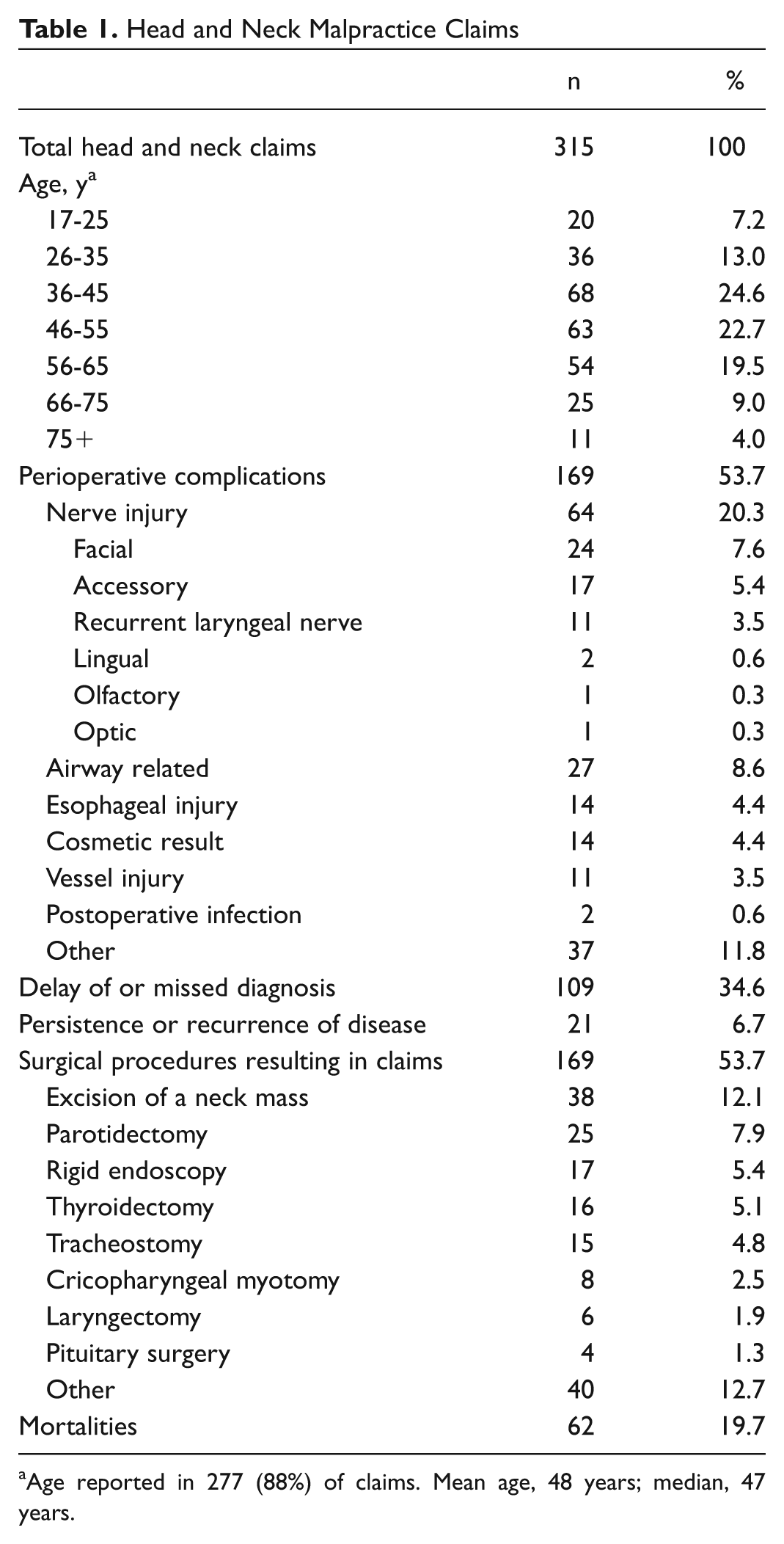
Age reported in 277 (88%) of claims. Mean age, 48 years; median, 47 years.
Overall, the greatest number of head and neck malpractice claims came from perioperative complications, representing 169 (53.7%) claims. These were followed by 109 (34.6%) claims related to delays in or missed diagnoses and 21 (6.7%) claims for persistence or recurrence of disease. Among perioperative complications, nerve injuries accounted for 64 (20.3%) claims, including facial (24, 7.2%), accessory (17, 5.4%), recurrent laryngeal nerve (11, 3.5%), lingual (2, 0.6%), olfactory (1, 0.3%), and optic (1, 0.3%) nerves. Airway-related complications led to 27 (8.6%) claims and resulted from loss of airway for various reasons. Most of these (14 of 27) were related to tracheostomy and occurred during the actual surgical procedure or at any time postoperatively. Other causes of airway loss were postoperative hematoma, unsuccessful management of disease-related obstruction, and loss of airway during induction or maintenance of anesthesia. Esophageal injuries accounted for 14 (4.4%) claims and were secondary to diagnostic endoscopy, surgical tumor ablation, and repair of esophageal diverticula. Patients who were unhappy with the cosmetic result of their operation were also included in this category and brought 14 (4.4%) claims. Vascular injuries resulted in 11 (3.5%) claims.
When perioperative complications were analyzed by procedure performed, excision of a neck mass accounted for 38 (12.1%) claims. Procedures included in this group were excisions of lymph nodes (excluding neck dissections), branchial and other cysts, lymphatic malformations, and carotid body tumors. Parotidectomy resulted in 25 (7.9%) malpractice claims, followed by rigid endoscopy (17, 5.4%), thyroidectomy (16, 5.1%), tracheostomy (15, 4.8%), cricopharyngeal myotomy (8, 2.5%), laryngectomy (6, 1.9%), and pituitary surgery (4, 1.3%; Figure 1 ). Overall, mortalities during any phase of the practice of head and neck surgery resulted in 62 (19.7%) lawsuits.
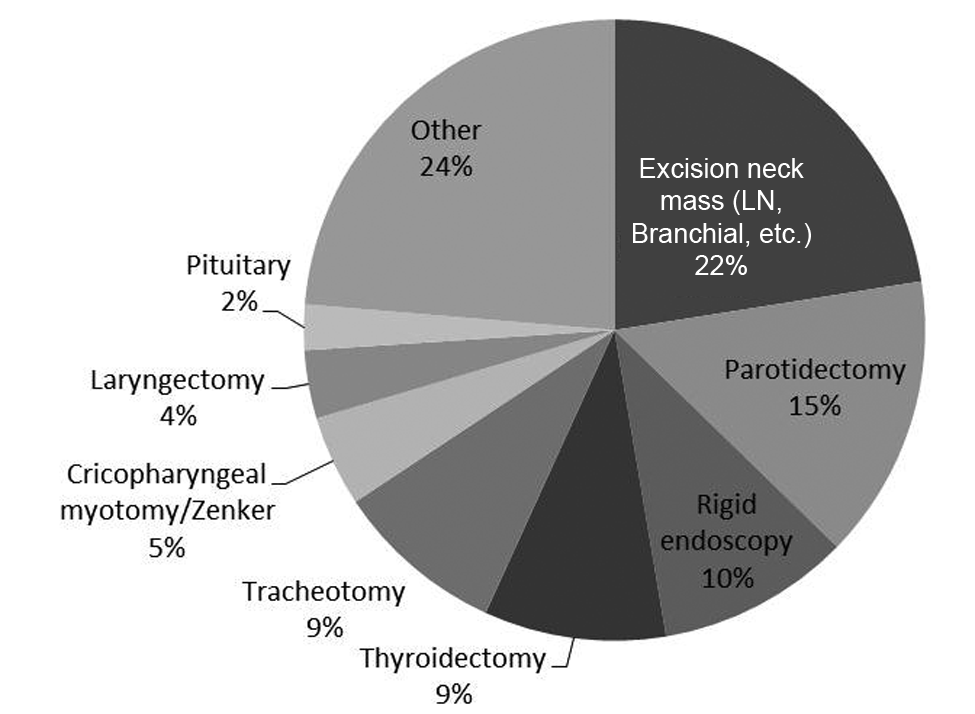
The most common head and neck procedures resulting in malpractice claims.
Award or settlement information was provided in 273 (87%) of the included claims. Of these, 121 (44.3%) claims resulted in a payment to the plaintiff. The overall mean indemnity award was $128,238. Payments in this series ranged from $1000 to $1,000,000. Payment information was further analyzed by claim ( Table 2 ). For delayed or missed diagnoses, 44 (36.4%) resulted in a payment to the plaintiff, and the average payment was $149,678. Nerve injuries resulted in 33 (27.3%) payments and a mean $157,769 per case. Airway complications led to 8 (6.6%) payments and an average of $150,616 paid. Claims filed for persistence or recurrence of disease ended in 13 (10.7%) payments and a mean $182,857 paid. Five (4.1%) payments resulted from esophageal injuries and averaged $229,000. Complaints of poor cosmetic outcome led to 2 (1.7%) payments and a mean $10,263 paid. Vessel injuries resulted in 5 (4.1%) payments and averaged $270,646 per case. When a claim included a mortality, a total of 20 (16.5%) payments were awarded, and the average amount was $165,530.
Number (%) of Plaintiffs Receiving Payments for Each Claim Type and Mean Indemnity Paid
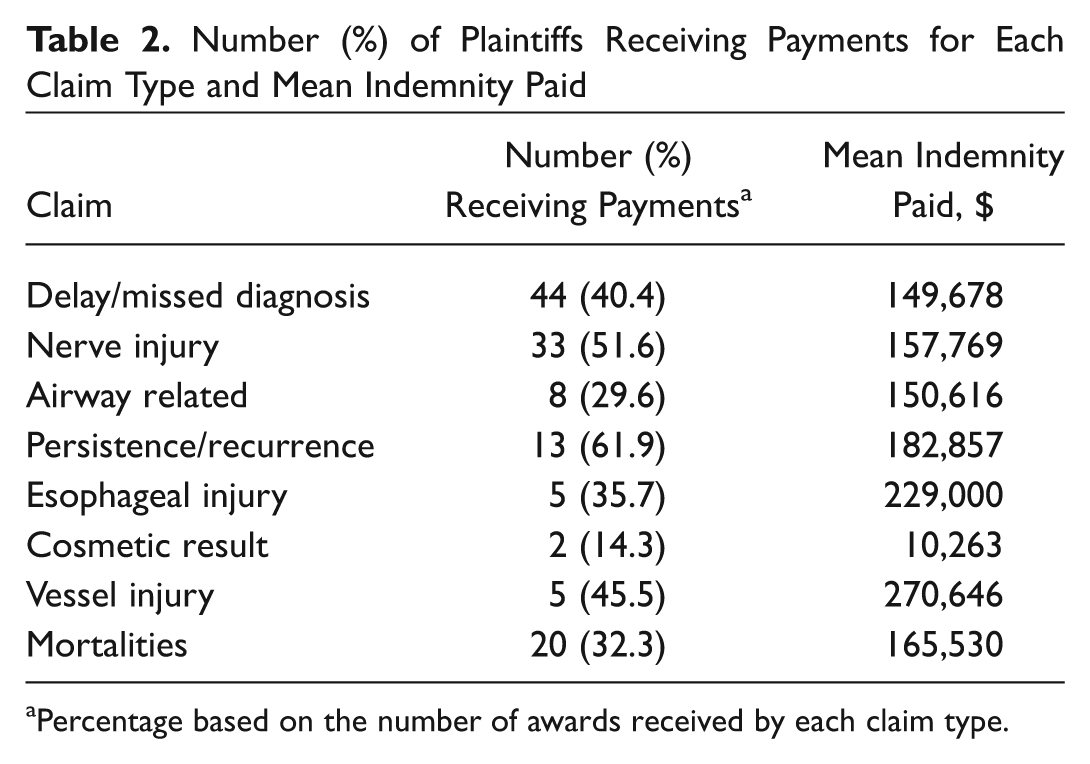
Percentage based on the number of awards received by each claim type.
Discussion
There are several, overlapping systems that exist to try to minimize medical negligence through different approaches. Morbidity and mortality conferences, medical review boards, hospital quality assurance programs, and medical malpractice law are some of these vehicles. Litigation analysis has been described as a method of reducing medical malpractice claims in various fields of medicine including head and neck surgery.2-9 The purpose is to identify common sources of litigation for a given medical specialty, procedure, or diagnosis to determine those sources that may be prevented. Most litigation analysis uses verdict summary data from legal databases that contain trial cases submitted by attorneys.2-10
The current review examines head and neck malpractice claims obtained from medical malpractice insurance carriers. Three hundred fifteen claims were identified as being related to the field of head and neck surgery. These data highlight 4 important sources of litigation: young patient age, perioperative complications, delays in diagnoses, and persistence or recurrence of disease.
Patient age has been reported as an important factor in head and neck surgery litigation.3,4,7,9 Plaintiff age was available in 88% of claims in the current review. The overall mean and median ages were 48 and 47 years, respectively ( Table 1 ). Similar mean and median ages were reported by Lydiatt for cancers of the larynx (49 and 46), thyroid (45 and 41), skin (49 and 50), and oral cavity (45 and 47). The age group that produced the greatest number of claims in our series was 36 to 45 years. Notably, these ages are significantly younger than the peak incidence for many cancers of the head and neck. 11 For instance, the peak age of incidence for cancers of the oral cavity and oropharynx is 80 to 84 years and for the larynx is 70 to 74 years. 11 This incongruence in peak age at the diagnosis of head and neck cancer and that leading to litigation suggests that young age is a significant factor in head and neck malpractice litigation.
Perioperative complications led to the greatest number of head and malpractice claims in this series, representing 53.7% ( Table 1 ). Nerve injuries represent the largest portion of perioperative complications, and injuries to the facial, accessory, and recurrent laryngeal nerves make up most (81%) nerve injury claims. This finding is not unexpected given the significant morbidity resulting from their injury and how commonly they are encountered during routine head and neck procedures.
Airway-related injuries accounting for 27 (8.6%) claims were the second most common source of claims from perioperative complications. This is a heterogeneous group of claims, including complications during initial airway management, anesthesia-related airway complications, and postoperative loss of airway. As expected, the mortality rate is high in this group, with 17 of 27 (62.9%) possibly explaining the high litigation rate. Indemnity awards were given in 29.6% of airway claims, with a mean award of $150,616. Overall tracheotomy was the fifth most common procedure resulting in lawsuits and led to 4.8% of all head and neck malpractice claims.
Of the 14 (4.4%) esophageal injuries, 6 were secondary to esophagoscopy and another 6 were related to crycopharyngeal myotomy often in treating diverticula. Of the 35.7% of claims resulting in indemnity payments, there was a surprisingly high mean award of $229,000, second only to that for vascular injuries. Complaints related to the cosmetic result of a procedure led to another 14 (4.4%) claims but resulted in the lowest percentage of payments (14.3%) and the lowest mean payment ($10,263).
Vascular injuries were a relatively uncommon source of malpractice claims with 11 (3.5%); however, of those claims that were filed, 45.5% led to awards. Monetary awards in this group were the highest, with a mean payment of $270,646. This is likely because these injuries often resulted in catastrophic neurologic injuries or death. It is possible that major vessel injuries represent an all-or-nothing phenomenon, where most are easily controlled or repaired with little perceived harm while the few that cannot be controlled are uniformly catastrophic.
The issue of informed consent cannot be overstated. This applies to all causes of medical malpractice but most specifically to claims related to surgical complications. Whether informed consent was provided and adequate was not stated in the present series, but its role in preventing malpractice claims in head and neck surgery has been reported.5-7,12,13 The ethics committee of the American Academy of Otolaryngology—Head and Neck Surgery has noted that in most states, it is the physician’s responsibility to disclose information that a reasonable patient would expect to know in order to make an informed decision. 14 This information should include (1) what is to be done; (2) anticipated benefits, probabilities, and expected consequences for the patient; (3) significant and/or frequent risks and their probabilities; and (4) all reasonable alternatives, whether performed by the surgeon or not. 14
Delay in diagnosis represents the second largest source of claims in this series. One hundred nine of the 315 claims have this allegation representing 34.6%. This contrasts with other studies, which have found delay in diagnosis to be the source of 54% to 86% or malpractice claims involving patients treated for cancer.2-4,7-9
It is important to note that a claim of delay in diagnosis alone is not enough to bring a suit in medical malpractice law. The plaintiff must prove among other things that harm or injury has occurred. 15 In the case of delay in diagnosis, this requires that the patient’s prognosis was worse because of the delay, which may arise not only from lack of action by the physician but also from mistakes made by support services, including clerical errors. The relatively high percentage of claims receiving awards in this series suggests that the courts agree that the prognosis was worse because of the delay. This is contrary to multiple studies showing that there is no correlation between delay and either stage of disease at presentation or survival.16-25
Persistence or recurrence of disease led to 21 (6.7%) of the head and neck malpractice claims in this review. In this series, patients were often noted to require additional surgery with greater morbidity. Notably, the tort system agreed with the patient’s claim of negligence nearly 62% of the time.
Interestingly, most head and neck surgeons consider persistence and recurrence of cancer an expected consequence of balancing the natural history and morbidity of the disease with that of the treatment. Close adherence to clinical practice guidelines for follow-up and surveillance may be the most important strategy in preventing malpractice claims related to persistence or recurrence of disease. 26 In addition, educating patients to appreciate symptoms of recurrent disease will possibly improve early detection. Agrawal and colleges 27 found that 40% of patients reporting new symptoms were ultimately diagnosed with recurrence during a routine follow-up visit, suggesting that earlier follow-up would have been possible had the patient recognized the symptoms and presented sooner than the planned visit.
There are some limitations to our study. First, the study represents a sample of data from 16 of the nearly 50 member companies of the PIAA. While it seems reasonable to extrapolate from our sample group, there could exist a selection bias of the groups who chose to participate in our study. Also, it should be noted that the PIAA represents privately insured physicians, and so physicians insured by academic centers are not included in the data set.
Conclusion
This study highlights 4 important sources of potential litigation related to the field of head and neck surgery: young patient age, perioperative complications, delays in or missed diagnoses, and persistence or recurrence of disease. These may be considered risk factors for litigation in head and neck surgery. Understanding these risks will help the head and neck surgeon to limit litigation in their practice and, most importantly, provide the highest level of care to their patients.
Author Contributions
Disclosures
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.