
Abstract
Objective
To test the strength of internal fixation of mandibular condyle fractures repaired with titanium miniplates versus titanium intramedullary implants.
Study Design
Prospective laboratory experimentation in urethane mandible models and human cadaveric mandibles.
Setting
Materials testing laboratory at an academic medical center.
Methods
Osteotomies of the mandibular condyle were created in 40 urethane hemimandible models and 24 human cadaveric specimens. Half of the samples in each group were repaired with traditional miniplates, and the other half were repaired with intramedullary titanium implants. Anteroposterior and mediolateral loads were applied to the samples, and the displacement was measured with reference to the applied force.
Results
Titanium intramedullary implants demonstrated statistically significant improved strength and stiffness versus miniplates in the urethane model experimental groups. Despite frequent plastic deformation and mechanical failures of the miniplates, a 1.6-mm-diameter titanium intramedullary pin did not mechanically fail in any of the cases. Intramedullary implantation failures were due to secondary fracture of the adjacent cortical bone or experimental design limitations including rotation of the smooth pin implant.
Conclusion
Mechanical implant failures that were encountered with miniplate fixation were not seen with titanium intramedullary implants. These intramedullary implants provide stronger and more rigid fixation of mandibular condyle fractures than miniplates in this in vitro model.
Fractures of the mandibular condyle pose a unique set of challenges to both physicians and patients. The continued academic debate and breadth of methods used in clinical practice to treat condyle fractures1-3 suggest that the ideal reparative procedure has yet to be perfected.
Current methods of treatment for condylar process fractures include rigid or elastic maxillomandibular fixation with or without reduction and open reduction and internal fixation of the condyle in situ through transfacial or transcervical incisions.1-3 In certain cases, the condyle can even be removed, plated ex vivo, and then reimplated into the patient.4,5 Although some of these methods do not restore the original anatomic relationships of the bone, they all share the goal of restoration of occlusion and masticatory function.
The cornerstone of mandibular function is its ability to withstand force at the condylar neck. Many authors have studied the forces acting on the mandible, and in particular the condyle, and have demonstrated that the condyle is only part of a complex system of loading and reactionary forces.6-8 The resulting forces acting on the working condyle have been demonstrated to fall within a range of vectors based on several factors, including the location of the bite, the action of the ipsilateral muscles of mastication, and the compensatory function of the contralateral muscles and bone.6-8 Koolstra et al 6 proposed a simplified mathematical vector of bite force loading, but in the presence of a surgical implant, it is also important to consider multiple loading scenarios to include the forces acting on the contralateral (or “balancing”) condyle and the mechanical behavior of the bone in the presence of the implant.
Compact bone resists compression better than it resists tension, and during biting, the posterior cortex of the condyle is subject to compression, whereas the anterior cortex is subject to tension. Lateral displacement forces are also exerted and are important to consider, especially in the case of the forces acting on the balancing condyle. Under this medial to lateral directed force vector applied at the temporomandibular joint, compression is placed on the lateral cortex and tension on the medial cortex. 7 These physiologic considerations demonstrate the forces that will act on a surgical implant that has been used to repair the condylar load-bearing system.
In a detailed study of forces acting on miniplates used to repair fractured condylar necks, Wagner and colleagues 9 demonstrated that the forces generated by biting were more than enough to exceed the strength of a titanium miniplate and can result in implant failure, a phenomenon that has been encountered in clinical practice. 10
We hypothesized that a short-segment titanium implant inserted into the medullary space above and below a condylar fracture ( Figure 1 ) would provide stable internal fixation in excess of the miniplates used in current clinical practice. Theoretical benefits that would result in increased strength with intramedullary (IM) fixation include eliminating the need to drill away healthy cortical bone for screw placement, placement of the implant in the central axis of the bone, and potential for increased thickness of the implant compared with external 1-mm-thickness miniplates (depending on individual patient anatomy). In addition, theoretical procedural benefits of this type of short-segment IM fixation include its potential for endoscopic application without the need for condylar periosteal stripping or the need for external incisions and their associated morbidity.
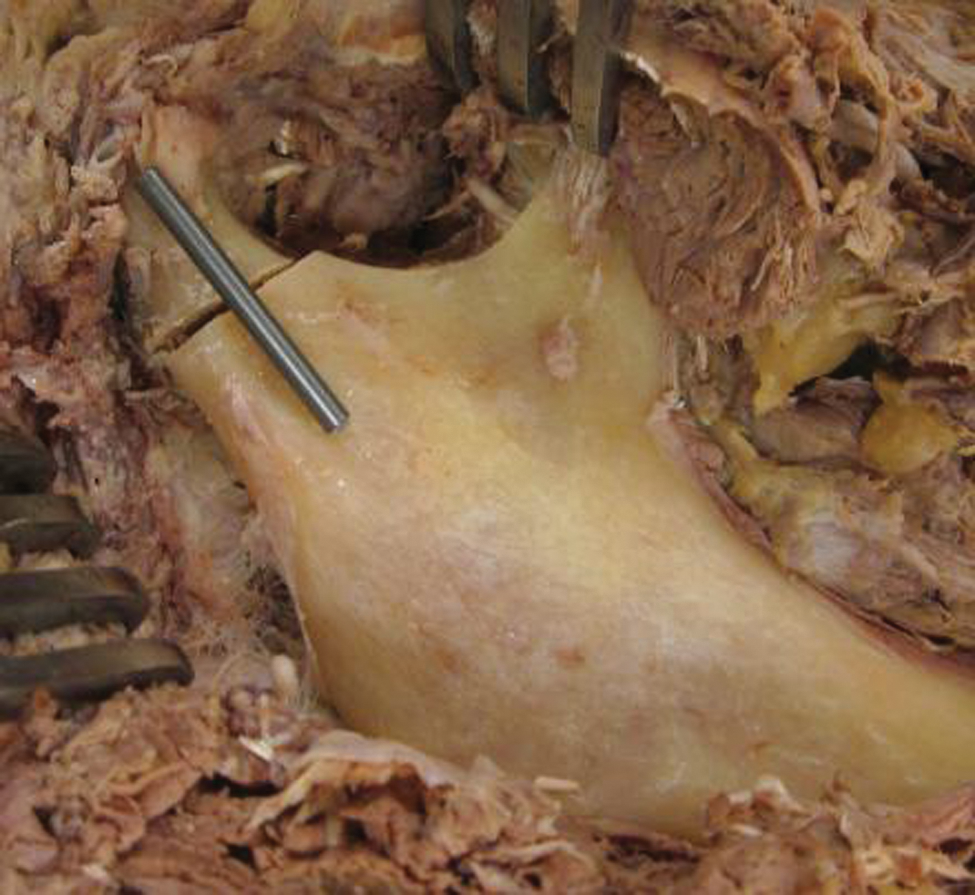
Demonstration of the anatomic location of the short-segment titanium intramedullary implant resting outside of a human cadaveric mandible. Once implanted, the entirety of the implant will be within the medullary space.
Methods
Materials
Synthetic urethane mandible models (Medical Accessories & Research Corp, Zeeland, Michigan) and preserved human cadaveric mandible specimens were used for implant testing. Four-hole 1-mm-thickness titanium miniplates with 2.3-mm-diameter 4-mm depth screws (Stryker, Kalamazoo, Michigan) or 2-cm-length IM pin implants fashioned from 1.6-mm-diameter titanium K-wire were used for fracture fixation. The titanium wire was prohibited from rotating for the purposes of experimentation by using epoxy applied in a stepwise manner in the medullary space with a double-layer paper collar to prevent the epoxy from contacting and adhering to the opposing fragment.
Definitions
For the purposes of this study, the following terms are defined as follows. Elastic deformation is the behavior of a material under stress, where it resists load but does not lose its shape. Plastic deformation refers to the behavior of a material under stress, where it resists force but is permanently distorted or bent while doing so. When stress is applied to a material, it first undergoes elastic deformation, then when it reaches its yield point, it begins to bend and plastically deform and finally undergoes catastrophic mechanical failure when it breaks. Strength is the amount of force an implant can withstand under specified conditions or displacements. Stiffness refers to the applied force divided by the displacement allowed by the implant. In this study, stiffness was calculated at a uniform displacement of 3 mm for all samples because at this distance, most samples were under load regardless of initial implant fit, and this displacement was seen prior to reaching the implant yield point in most cases.
The following types of strength are also referenced. Ultimate strength refers to the condition where the experimental specimen and its implant no longer maintained consistent material properties, and ultimate force is the amount of load needed to reach the material’s ultimate strength. Ultimate strength is then divided into subgroups based on the cause for this mechanical malfunction. The type of ultimate mechanical implant failure describes how the physical characteristics of the implant itself lose the ability to resist force. Physical observations included in the category include bending, warping, breaking, and extrusion of screws. Experimental construct failure is when the conditions of the experimental setup lead to the loss of resistance to force. Examples of experimental construct failure include crushing of the sample, movement of the condyle in degrees of freedom that are not being tested (ie, rotation or sliding). Finally, fracture of adjacent cortex refers to ultimate mechanical failure of the mandible substrate while the implant was continuing to bear load in either elastic or plastic deformation.
Experimental Methods
Experiments were conducted using an MTS servohydraulic testing machine (model 812.21; MTS Systems Inc, Minneapolis, Minnesota). Perpendicular application of either anteroposterior (AP) or mediolateral (ML) directed force was used. Load and displacement of the press were measured. Ultimate mechanical failure (either due to implant or mandible substrate failure, whichever occurred first) was measured at the apex of the load versus displacement curve and/or upon gross deformation of the implant or mandible.
Statistical Analysis
To control for experiment-wide type I error, we ran a 3-way multivariate analysis of variance (MANOVA) in SAS version 9.2 (SAS Institute Inc, Cary, North Carolina), with the independent variables treatment (intramedullary pin vs miniplate), force (AP vs ML), and material (urethane vs cadaver) and using 3 dependent variables: load at failure, displacement, and stiffness. This is a single omnibus test that allowed us to test the main effects of each independent variable while controlling for the others, on a linear combination of the dependent variables. The MANOVA model testing main effects found that treatment (intramedullary pin vs miniplate; P < .0001), force (AP vs ML; P < .0001), and material (urethane vs cadaver; P < .0001) were each independently associated with the linear combination of the 3 dependent variables. Since this is a single test, it allowed us to maintain the experiment-wide alpha level at P < .05. Significant results in this analysis were then explored further using individual 2-tailed independent samples t tests in MedCalc version 11.5 (MedCalc Software, Mariakerke, Belgium). P values of <.05 were considered statistically significant.
Correlations among the dependent variables were evaluated using Pearson coefficients.
Institutional Review Board Approval
This study is not subject to institutional review board review, as it does not involve live human subjects.
Results
Force versus Displacement Curves (Implant Strength)
Applied force versus displacement was graphed for each of the urethane mandible experimental groups over displacements from 1 to 5 mm. In the case of AP applied force, IM fixation demonstrated statistically significantly higher strength for all displacements (from 1-5 mm; Figure 2A ). In the case of ML applied force, IM fixation showed higher strength of fixation reaching significance at displacements of 2 to 5 mm ( Figure 2B ).
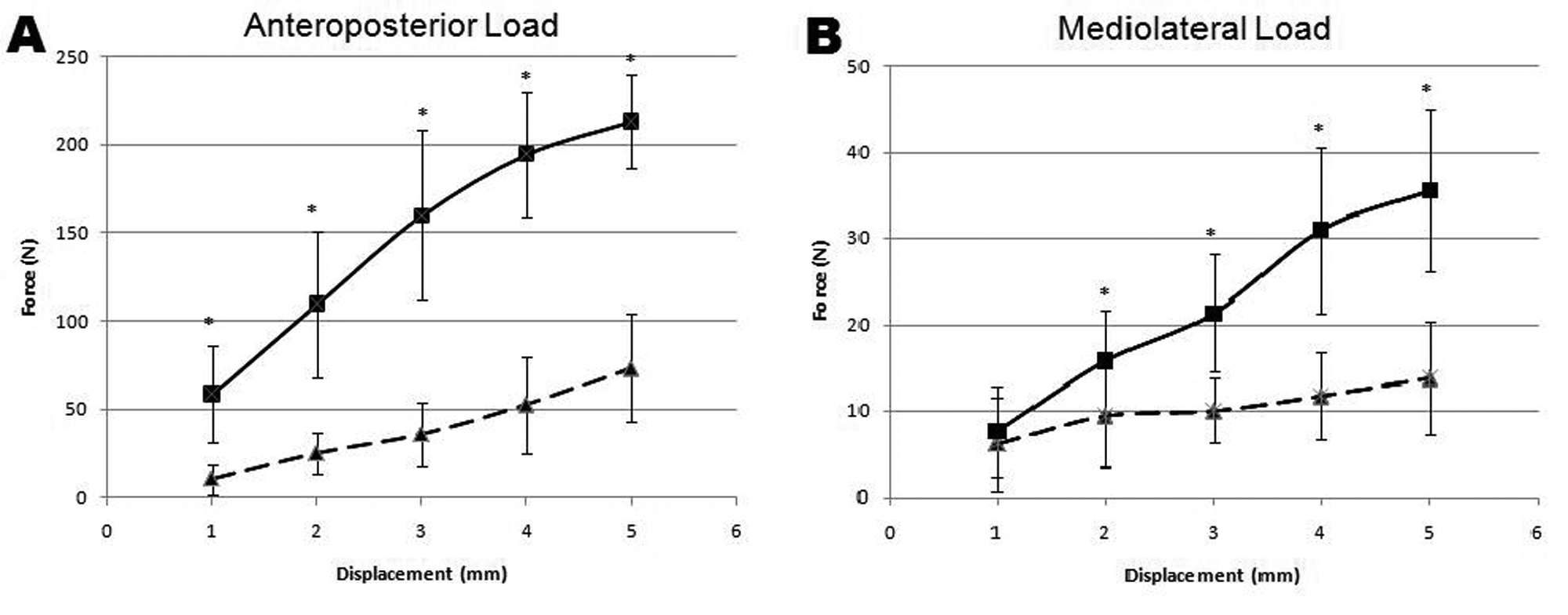
Force versus displacement curve of intramedullary (solid line) versus miniplate (dashed line) fixation of condylar neck osteotomies under anteroposterior (A) and mediolateral (B) directed load. Error bars represent standard deviation, and asterisk (*) denotes P < .05 in comparing the 2 types of fixation for each displacement point.
Despite significant data in the urethane groups, cadaveric mandible data for both miniplate and IM implant fixation failed to demonstrate statistically significant differences in strength. There was a higher degree of variability in this subset of data because of cases of poor implant fit and failure of fixation after only 2 mm of displacement.
Force for Implant Failure (Ultimate Force)
More than double the force was required to cause failure of fixation when IM implants were used versus traditional miniplates in the urethane mandible groups after application of either AP or ML force. This reached statistical significance with P < .001.
The cadaveric mandible group repaired with IM implants also required more than double the force to cause fixation failure after application of ML force when compared to its corresponding miniplate group. This was also statistically significant, with a P value of .017 ( Table 1 ). With respect to AP force, the cadaveric mandible group repaired with IM implants showed increased force required to induce failure compared with the miniplate group. However, this failed to reach statistical significance.
Summary Results for the Force Required to Cause Implant Failure, Displacement of the Condyle at Implant Failure, and Stiffness of the Implant at 3 mm of Displacement a
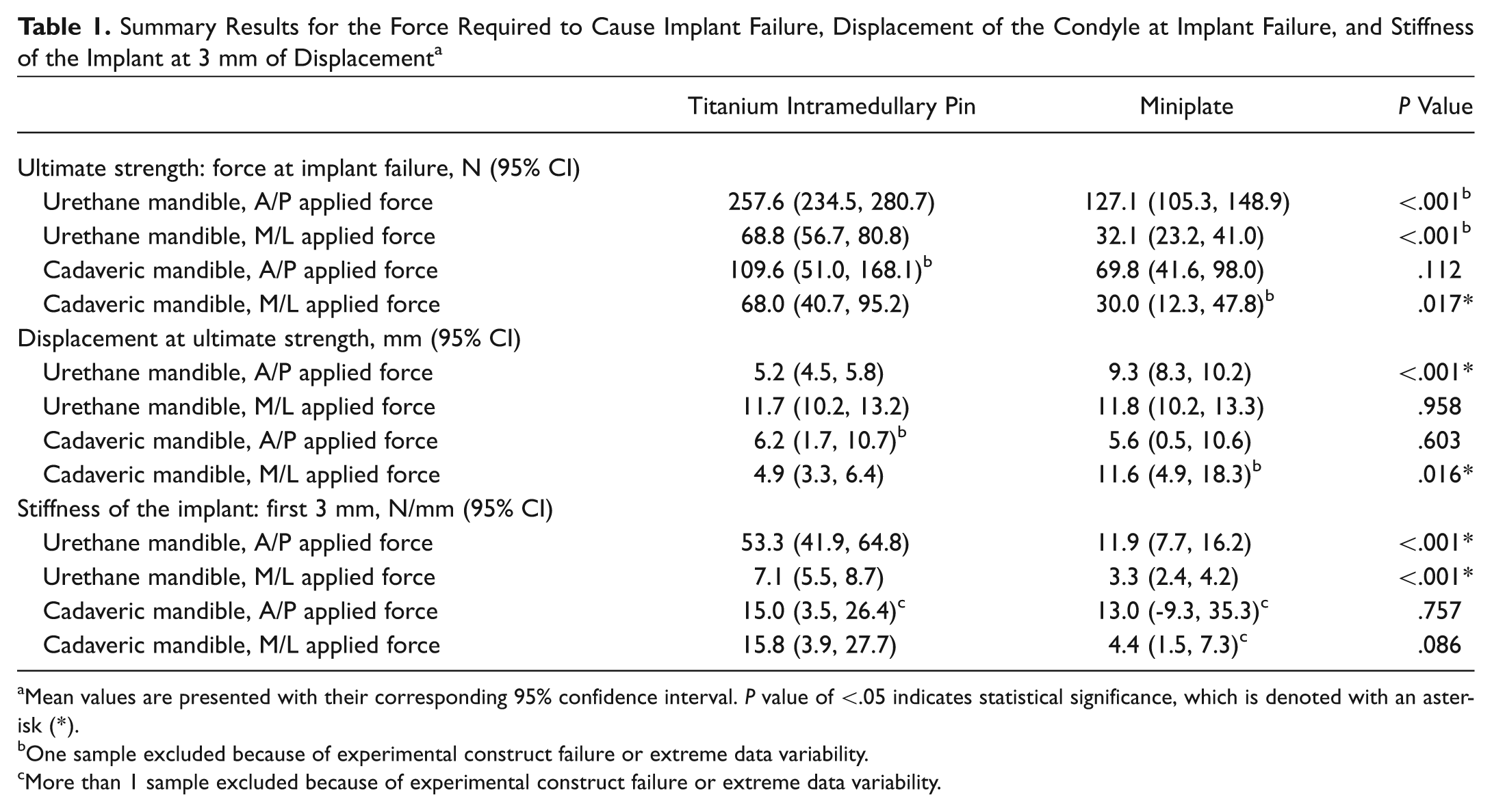
Mean values are presented with their corresponding 95% confidence interval. P value of <.05 indicates statistical significance, which is denoted with an asterisk (*).
One sample excluded because of experimental construct failure or extreme data variability.
More than 1 sample excluded because of experimental construct failure or extreme data variability.
Displacement at Ultimate Force
Compared with miniplates, IM implant fixation failed under higher forces but at nearly half of the displacement in the urethane mandible AP force group, indicating a statistically significant increased strength of fixation when IM implants are used (P < .001). When ML force was examined, the displacement at ultimate strength was similar in the mandible and miniplate groups ( Table 1 ).
There was a statistically significant (P = .016) difference in the mean displacement at ultimate strength when the ML load was applied to the cadaveric samples. However, there was no significant difference in the mean displacement at ultimate strength between the cadaveric specimen groups when AP force was applied to the miniplate and IM implants.
Stiffness of Fixation at 3 mm
Stiffness (force/displacement) was calculated at the displacement point of 3 mm. There was a statistically significant increase in the stiffness of IM implant fixation groups in the urethane mandibles for both AP (greater than 4× stiffness, P < .001) and ML (greater than 2× stiffness, P < .001) force directions. Cadaveric mandible group measurements failed to meet significance because of multiple failures prior to 3 mm of displacement and the experimental construct problems and anatomic variability mentioned previously ( Table 1 ).
Correlation between Dependent Variables
Raw Pearson correlations were −0.38 for ultimate force versus displacement at ultimate force, –0.60 for stiffness at 3 mm versus displacement at ultimate force, and 0.89 for stiffness at 3 mm versus ultimate force. These correlations are in accordance with the expected relationships of these material properties of the implants.
Types of Implant Failure
The IM implant and miniplate groups demonstrated markedly different patterns of fixation failure. These results are summarized in Table 2 . In detail, all 20 of the urethane models repaired with miniplates suffered ultimate mechanical implant failure ( Figure 3A ). Nineteen of the 20 IM implanted urethane models failed because of fracture (ultimate mechanical implant failure) of the adjacent cortex of the bone substitute prior to the IM implant’s reaching its ultimate strength ( Figure 3B ). There was 1 case of failure of the experimental construct in the urethane IM implant group.
Summary of the Types of Mechanical Failure for Each Experimental Implant and Mandible Substrate Combination a
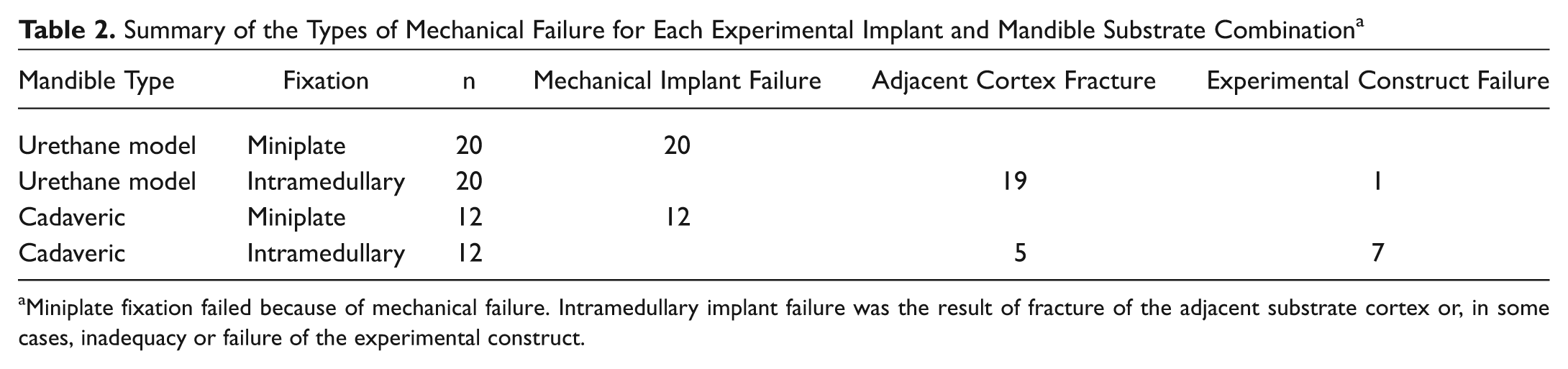
Miniplate fixation failed because of mechanical failure. Intramedullary implant failure was the result of fracture of the adjacent substrate cortex or, in some cases, inadequacy or failure of the experimental construct.
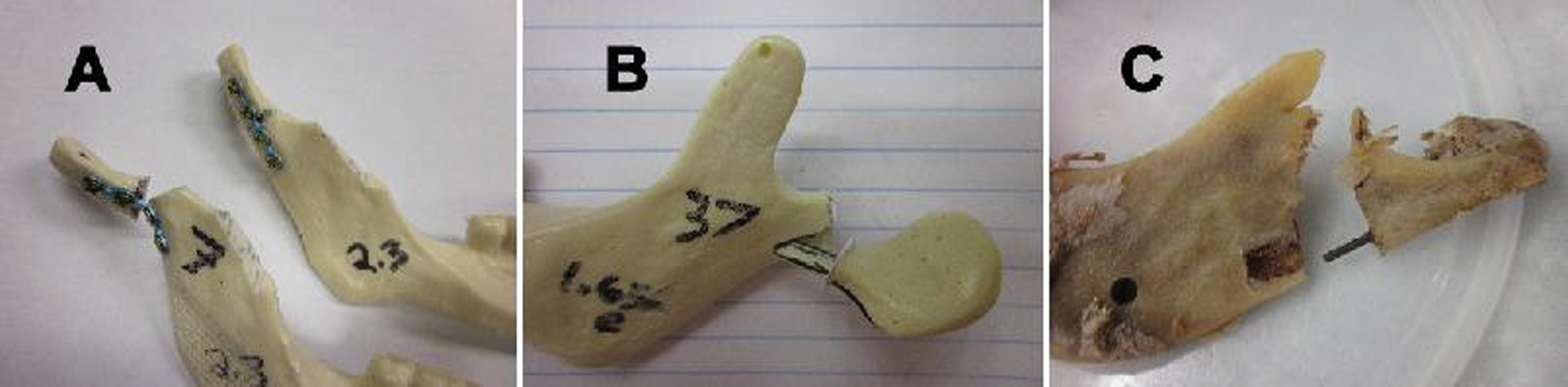
Photographs of several types of fixation failure. (A) Bending mechanical failure of a miniplate. (B) Secondary fracture of the adjacent urethane cortex. (C) Similar secondary fracture of cadaveric cortical bone when intramedullary implants are used for fixation. Note that in both (B) and (C), the intramedullary implant itself remains in its original conformation.
Similar to the urethane models, all 12 cadaveric samples repaired with miniplates suffered the same type of bending or screw extrusion implant failure. However, the cadaveric mandibles repaired with IM implants posed a more significant challenge to the experimental setup because of the wide variability of the size of the medullary space in human bones ( Figure 4 ). The same 1.6-mm-diameter implant size was used for experimental uniformity in all samples, but the fit was poor in many specimens. This led to more than half (7 of 12) of these samples failing because of poor implant fit causing rotation of the condylar head or sliding of the condyle along the axis of the implant. In the samples in which there was good implant fit, a similar fracture of adjacent cortical bone (as seen in the urethane mandibles) was encountered upon ultimate failure ( Figure 3C ).

Photograph demonstrating the variability in medullary space diameter and shape in cross sections of cadaveric condyles. This medullary space variability led to inconsistent data in the cadaveric groups because of poor implant fit (for uniformity the standard 1.6-mm-diameter IM implant was used in all specimens).
Discussion
The technique of IM fixation for fractures of tubular long bones was pioneered by German surgeons in the early 20th century. Küntscher advocated this technique for repair of femur fractures because of its benefits of rapid development of a firm callus, lack of damage to the periosteum and surrounding musculature, faster return to mobility and weight bearing, and greater ease in application compared with plates.11-13 These benefits mirror the goals of facial trauma surgeons when repairing fractures of the mandibular condyle.
Intramedullary fixation of the mandibular condyle has previously been attempted in the form of wires or lag screws applied from the inferior border of the mandibular angle, through the ramus, and into the condyle.14,15 These implants, which span the entire length of the ramus and condyle, are most readily applied when the profile of the ramus is a straight vertical line and it contains an intact medullary space throughout. Unfortunately, the natural curvature of the bone and variability in medullary space size and continuity complicate their application. Short-segment titanium IM condylar fixation may help to overcome these anatomical obstacles; however, the strength and mechanical properties of this type of fixation must be established first.
Based on the results of this study, the mechanical properties of 1.6-mm-diameter short-segment IM implants were superior to 4-hole miniplates in many respects. Short-segment IM fixation demonstrated superior ultimate strength and stiffness. These results were statistically significant for all of the urethane mandibular model experimental groups with the exception of fixation stiffness under ML applied force. The use of urethane mandibular models has been widely accepted as an experimental substitute for human mandibles because of their uniformity and physical properties.15-18 Many previous studies have used these models exclusively.15,17-19 Our data for urethane model fixation correspond with these previous studies and demonstrate the benefits of IM fixation.
When repaired with a titanium IM implant, the mean AP force required to fracture the adjacent cortical urethane and cause ultimate failure of fixation was 258 N. This is more than double the strength of miniplate fixation observed in this study (127 N) and reported by other groups (115 N). 15 Furthermore, the strength of short-segment titanium IM fixation correlates with the strength of other forms of IM fixation of the condyle, including the Ekelt lag screw. 15
The cadaveric specimens used here add an additional dimension to the assessment of the performance of these implants. Although complicated by inconsistent fixation due to anatomic variability, the cadaveric mandible groups demonstrated a positive trend favoring the strength and stiffness of IM implant fixation, which did not reach statistical significance. Small sample size, combined with experimental failures secondary to anatomic variability in the size of the medullary space, led to these inconclusive results. The diameter of the implant was kept constant for the purposes of measuring the material properties of the implant, but this led to a loose fit in the medullary space in many cases. The more useful of the cadaveric findings is that in the samples that did have adequate fit and fixation, the type of ultimate mechanical failure was the same as in the urethane groups. That is, the ultimate strength of the adjacent bone was overcome, and the cortex fractured before reaching the ultimate strength of the IM implant and observing failure of the implant itself. Therefore, with IM implants, unlike with miniplate fixation, the implant is no longer the mechanically weakest element of the repaired condyle.
The mechanical benefits of IM versus miniplate fixation have been demonstrated in this in vitro study. However, further experimentation is needed to refine the design and surgical application of short-segment titanium IM implants. If the theoretical benefits of total endoscopic application of these IM implants are realized, it may prove to be a less morbid method of achieving greater strength of fixation of fractures of the mandibular condyle.
Conclusion
Short-segment titanium IM fixation of mandibular condyle fractures shows superior strength and stiffness versus miniplate fixation in this in vitro model. The observed uniform ultimate mechanical failure of miniplates and lack of ultimate mechanical failure of the IM implants confirm the numerical findings that the IM implants are stable, rigid, and return a greater degree of strength to the condyle, so much so that the fixation remains durable until the adjacent bone fractures secondarily under higher forces.
Author Contributions
Disclosures
Footnotes
Acknowledgements
The authors would like to thank Mark Wagner, and the Materials Testing Laboratory at The George Washington University for their assistance with development and execution of the materials testing experimental protocol. We would also like to acknowledge Richard Amdur, PhD, for his assistance with the statistical analysis.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
This article was presented at the 2011 AAO-HNSF Annual Meeting & OTO EXPO; September 11-14, 2011; San Francisco, California.