
Abstract

Keywords
Thyroglossal duct cyst (TGDC) is the most common congenital neck anomaly in childhood, representing more than 75% of congenital midline neck masses. At least half are diagnosed in the second decade of life, although they may be presented later. 1 Although less common, TGDCs may be encountered in adults and in elder patients. 2 The average size of TGDCs is 2 to 4 cm in diameter. 3
Case Presentation
This work received the approval of the Edith Wolfson Medical Center institutional review board (IRB). A 35-year-old man with schizophrenia presented with a longstanding painless huge anterior neck mass. The overlying skin was irritated, with a peau d’orange appearance ( Figure 1 ). Accompanied by his family, he reported a previously known neck lump that had grown during recent years. He attended the clinic because of increasing dysphagia, discomfort, and drooling. There were no respiratory symptoms. Neither the patient nor his family members appeared disturbed by the extraordinary neck finding. The patient was pale, with a huge, soft, lobulated anterior neck mass measuring 30 × 24 cm, moving upon deglutition. The base of the tongue was pushed posteriorly by the cystic mass, causing a slight oropharyngeal obstruction and swallowing difficulties. However, the floor of the mouth was normal. Larynx appeared normal. A neck computed tomography (CT) study demonstrated a lobulated cystic neck mass, extending from the base of the tongue, adjacent to the floor of the mouth and anterior to the hyoid bone, the sternocleidomastoid muscles, and the normal-appearing thyroid gland ( Figure 2 ). The differential diagnosis included thyroglossal duct cyst, cystic hygroma/lymphangioma, thyroid neoplasm, epidermoid cyst, and plunging ranula, which may present as a midline neck mass. A diagnostic aspiration revealed abundant colloid, with a few pseudociliated epithelial cells, suggesting TGDC. Addressing the relatively large size, surgical planning mandated a wide horizontal neck incision to allow the safe exploration of the mass and its surroundings, including the hyoid bone, suprahyoid muscles, laryngeal skeleton, submandibular glands, and hypoglossal nerves. Partial excision of the body of the hyoid bone and the excess skin was also taken into consideration. Anticipating a possible difficult intubation, an awake, nasotracheal intubation was performed. The patient underwent an “extended” Sistrunk operation that included an en bloc resection of the cystic mass, along with the suprahyoid muscles that were adherent to it. A meticulous dissection of compressed nerves and vessels was necessary, in particular the left tortuous hypoglossal nerve. As planned, the middle portion of the hyoid bone, including a short, wide tract leading to the base of tongue and the overlying skin, was resected. The cyst colloid volume was 3 L. Pathological report confirmed thyroglossal duct cyst, with no signs of malignancy. The postoperative course was remarkable for worsening swallowing difficulties, which caused aspirations and required feeding gastrostomy and swallowing training. A remarkable improvement was observed at follow-up visits.
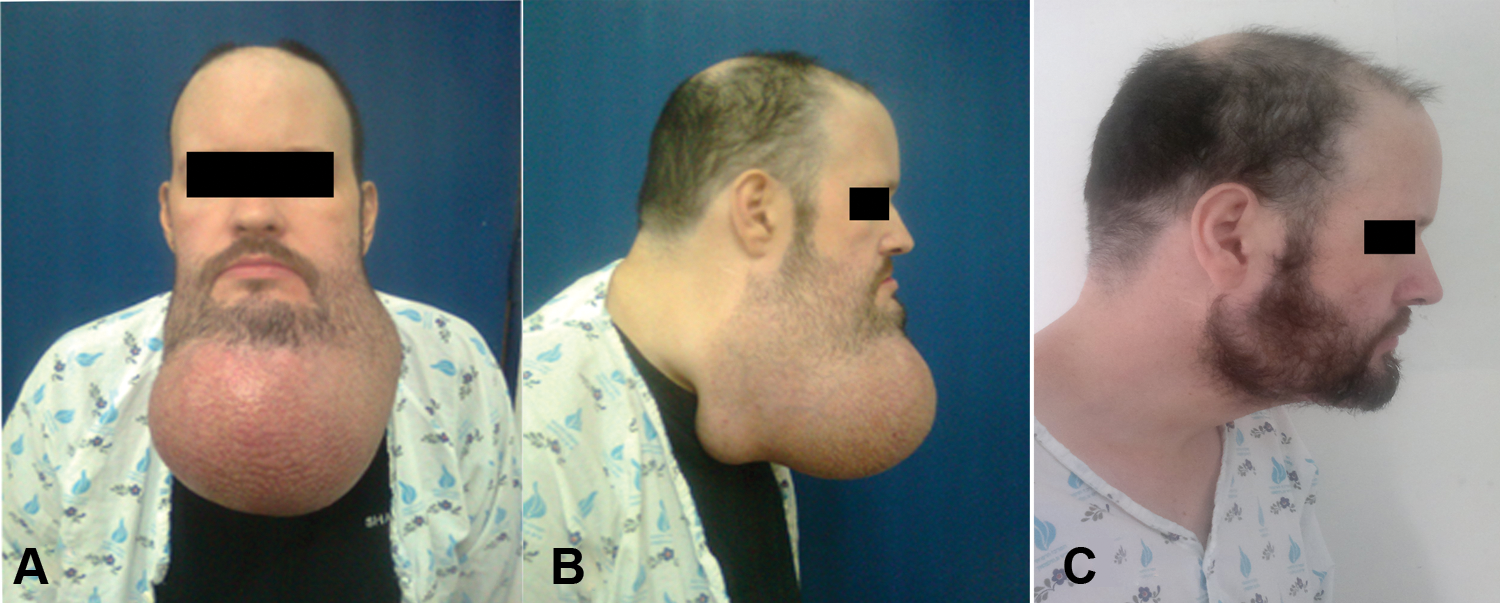
The patient before surgery. (A) Preoperative frontal view. (B) Preoperative lateral view, to the right. (C) Postoperative lateral view, to the right.
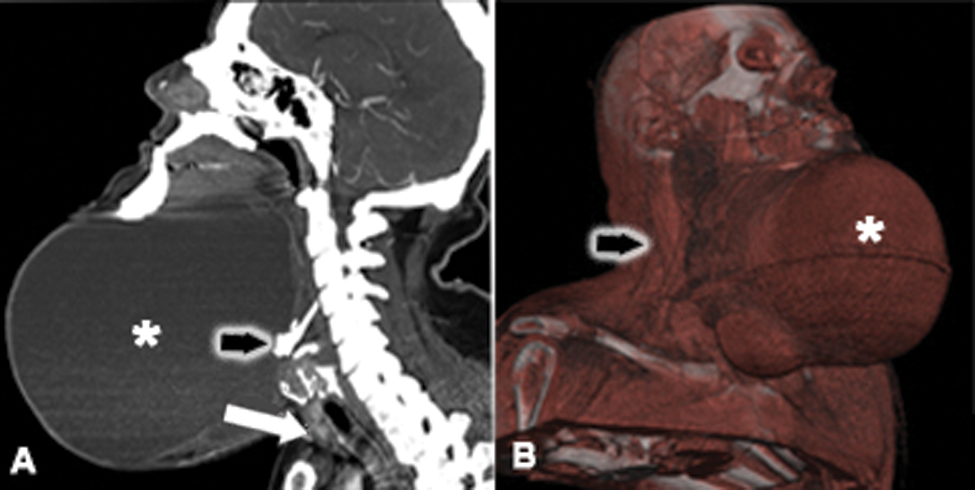
Contrast computed tomography demonstrating the neck mass. (A) Sagittal view of the anterior neck cystic mass (asterisk), anterior to the hyoid bone (black arrow) and the normalappearing thyroid gland (white arrow). (B) Three-dimensional oblique reconstruction, demonstrating the cystic neck (asterisk), anterior to the sternocleidomastoid muscle (black arrow).
Discussion
The usual appearance of a TGDC is a small, midline, sometimes more to the left, anterior neck mass, commonly accompanied with sore throat, dysphagia, globus sensation, dysphonia, and fistula formation. 4 The presented patient had an outstanding neck mass. Even more exceptional was the seemingly indifferent attitude of the patient toward his growing tumor, until pain and dysphagia occurred. Neglect or denial, by either the patient or his family, was a major contributing factor for the rather late presentation to medical caregivers. In addition, the psychiatric background, specifically an inadequate body image perception, often reported among schizophrenia patients 5 ; pathologic family perceptions, usually seen in such circumstances; and the slow growth pace of the lesion influenced both judgment led to the delayed decision to seek medical help. This unusual case demonstrates distorted body image awareness, ending up with an advanced neck tumor with significant morbidity.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.