
Abstract
Objective
To report the prevalence of anatomic variants on computed tomography (CT) in congenital aural atresia (CAA) and external auditory canal stenosis (EACS). Anatomic variants included inferiorly displaced/obstructing tegmen mastoideum, malleus-incus complex (MIC) directly lateral to stapes, facial nerve obstruction of oval window (OW) or middle ear, and incudostapedial joint (ISJ) angle.
Study Design
Cross-sectional study.
Setting
Tertiary care children’s hospital.
Subjects and Methods
An anatomic analysis of 130 CT scans (98 children, 32 bilateral) of CAA/EACS, performed by a blinded neuroradiologist. Both Jahrsdoerfer’s and new/modified anatomic considerations were graded in 32 atresiaplasty and 66 nonsurgical patients. Surgical data were analyzed for anatomic correlations related to surgical findings.
Results
Prevalence of anatomic variants was as follows: 13% of the ears had mild inferior displacement of tegmen, 4% had a significantly obstructing tegmen, and 24% had MIC directly lateral to stapes. The facial nerve obstructed access to OW in 41% and middle ear in 21%. Six atresiaplasty patients were reported to have a large MIC obstructing stapes access with increased intraoperative difficulty in viewing and assessing the integrity and mobility of the ISJ and stapes. Five of these 6 (83%) were noted on CT scan. The mean ISJ angle was 101° (range, 51°-155°).
Conclusion
A large obstructing MIC increases difficulty of atresiaplasty. Awareness of the presence of these anatomic variants is an aid in teaching temporal bone anatomy and may possibly influence the decision regarding atresiaplasty.
Keywords
The management of congenital aural atresia (CAA) and external auditory canal stenosis (EACS) presents significant challenges to otologic surgeons. The prevalence is 1 in 10,000 to 20,000 and is usually associated with microtia and ossicular malformations. Current surgical options include atresiaplasty and bone-anchored hearing aid (BAHA). Determining which procedure will give the best outcome is an important decision in managing these patients.1-4
To choose the most beneficial therapy, both audiologic and radiologic evaluation must be available prior to any intervention. Through auditory brainstem response, otoacoustic emissions, and/or audiometry, preoperative hearing can be successfully evaluated. A patient is not considered an atresiaplasty candidate if there is abnormal cochlear function.2,3
High-resolution computed tomography (CT) of the temporal bone is the standard radiographic test. Currently, the CT scan is evaluated based on the criteria developed by Jahrsdoerfer and colleagues. The numerical grade determines whether they are candidates for atresiaplasty. Jahrsdoerfer criteria are based on 9 anatomic considerations: each is given 1 point if favorable, except the stapes, which receives 2 points. A total score of less than 6 indicates that the patient is not a surgical candidate, while a score of ≥6 indicates that the patient may be a candidate for surgery. Studies have shown that the higher the Jahrsdoerfer score, the better the postsurgical hearing outcome.2,4 Favorable surgical candidates may undergo atresiaplasty. Alternatively, if the patient is not a candidate for atresiaplasty, or if the family declines to proceed with atresiaplasty, the BAHA is a suitable option.5,6
In our pilot study, we performed a similar but more limited anatomic analysis in a smaller (n = 32) cohort of patients. 7 In the present prospective, blinded anatomic study, we sought to evaluate a much expanded number of anatomic features in patients with CAA/EACS. A much larger cohort was evaluated in the present study (n = 130 ears), which should provide a more representative sample of the true prevalence of these interesting anatomic variants of temporal bones in CAA/EACS. We therefore analyzed Jahrsdoerfer criteria, the new/modified anatomic points considered in our pilot study, as well as the incudostapedial joint (ISJ) angle. 8 We also performed a retrospective medical review of operative findings in the subset of patients who had undergone atresiaplasty.
Methods
This was a cross-sectional study of patients with CAA/EACS from 1994 to 2010 at Children’s Hospital of Pittsburgh (CHP) of the University of Pittsburgh Medical Center (UPMC). Approval of the Institutional Review Board at UPMC was obtained. All pediatric patients with a diagnosis of CAA/EACS were reviewed by computerized electronic medical record search.
Of the 159 patients, 98 patients met the following inclusion criteria: atresia was not acquired and the patient underwent a high-resolution temporal bone CT. Furthermore, 32 of these patients had atresiaplasty surgery performed at CHP, a preoperative CT scan, and preoperative and postoperative audiologic assessment.
Medical records were reviewed for all eligible patients, and a database with the following variables was established:
Demographics: age at surgery and CT scan, and sex
Primary diagnosis: right, left, or bilateral, CAA/EACS
Radiographic assessment
Intraoperative findings
Procedures
Outcomes: preoperative and postoperative audiograms
Ninety-eight CT scans of both atresiaplasty and nonsurgical patients were reviewed. The typical examination was performed on a 64-detector-row scanner without the use of intravenous contrast. Initial acquisition consisted of 0.6-mm axial images with kVP of 120 and mA of 130. Small field-of-view reconstructions were performed for each ear, and multiplanar reformats were performed at 1-mm spacing and 1-mm thickness. The interpretation was performed by a Certificate of Added Qualifications–certified neuroradiologist with 12 years of special expertise in temporal bone anatomy, who was blinded to all patient information. We evaluated Jahrsdoerfer criteria, new/modified considerations, and ISJ angle.7,8
The following were the specific anatomic criteria and associated points awarded during evaluation of the CT scans of the temporal bones in CAA ( Table 1 ):
Modified Grading System for Computed Tomography in Congenital Aural Atresia/External Auditory Canal Stenosis
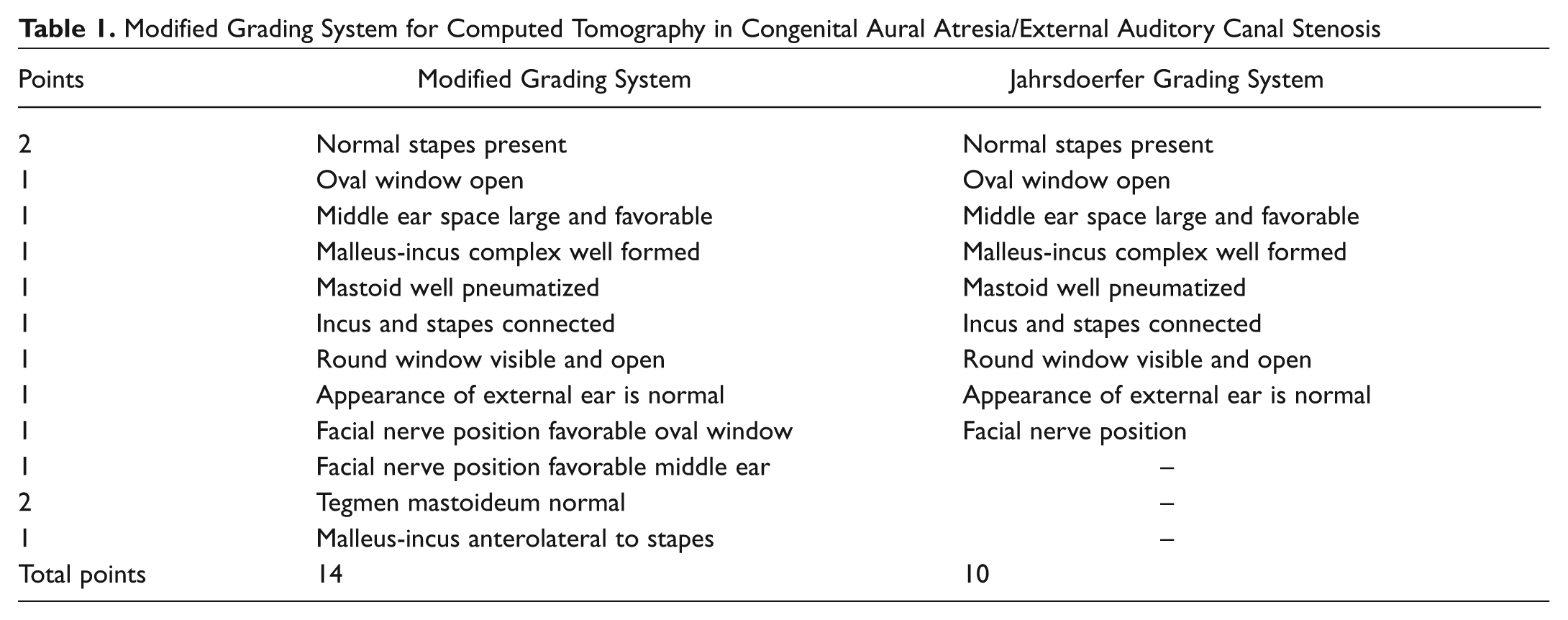
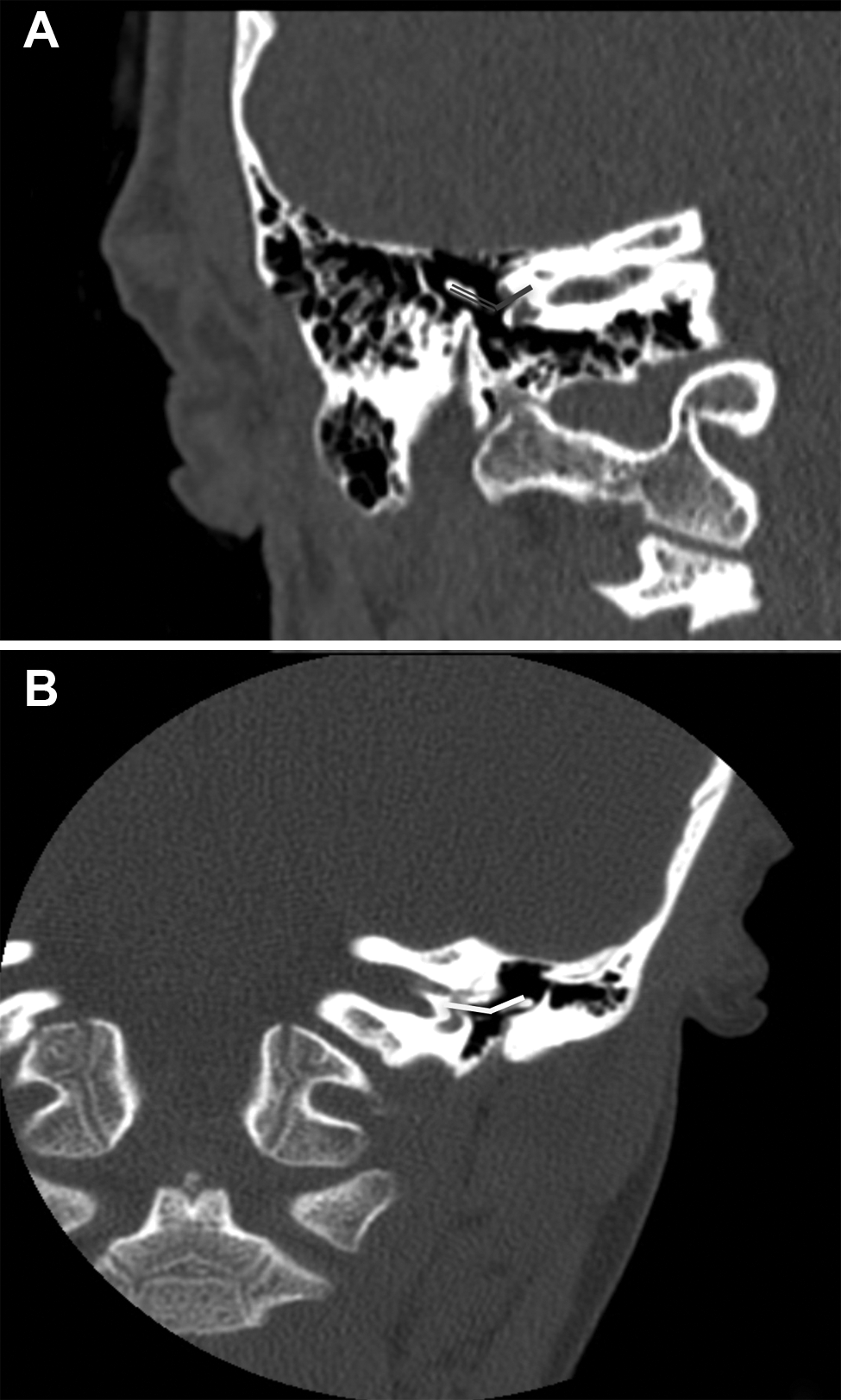
Position of tegmen mastoideum. Displacement of the tegmen mastoideum was judged relative to the middle ear height (ie, the vertical distance between the roof of the epitympanum and the inferior aspect of the hypotympanum). Two points were assigned if the tegmen was in a normal superior position (nondisplaced or displaced less than 25% of the middle ear height). One point was assigned if the tegmen was mildly inferiorly displaced (25% to 50% of the middle ear height; Figure 1A ). Zero points were awarded if there was severe inferior displacement (>50% of the middle ear height; Figure 1B ).
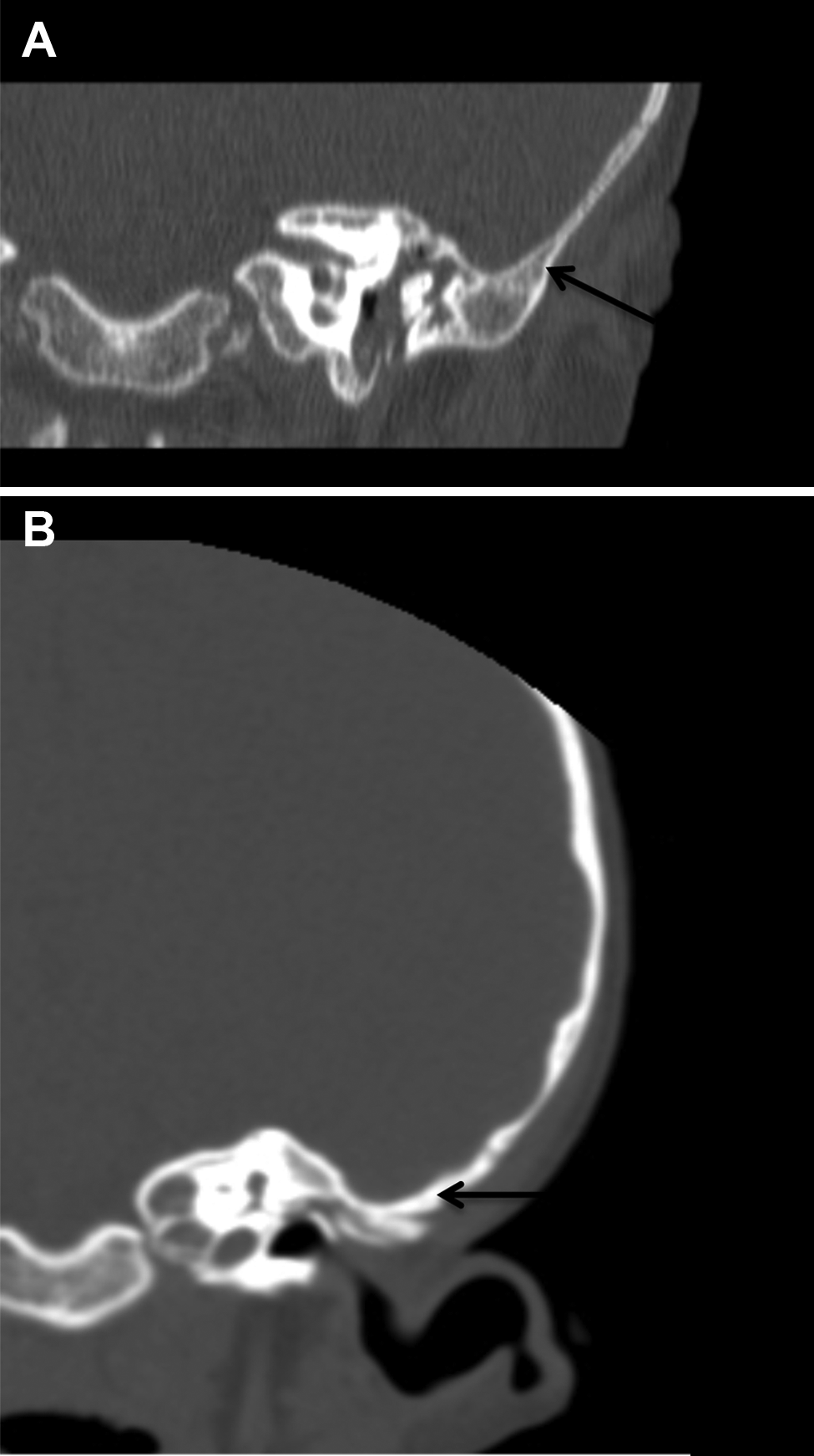
Size and position of the malleus-incus complex (MIC) in relation to stapes. The normal anterolateral MIC position was awarded 1 point. When the MIC was large and positioned directly lateral to the stapes, 0 points were awarded ( Figure 2 ).
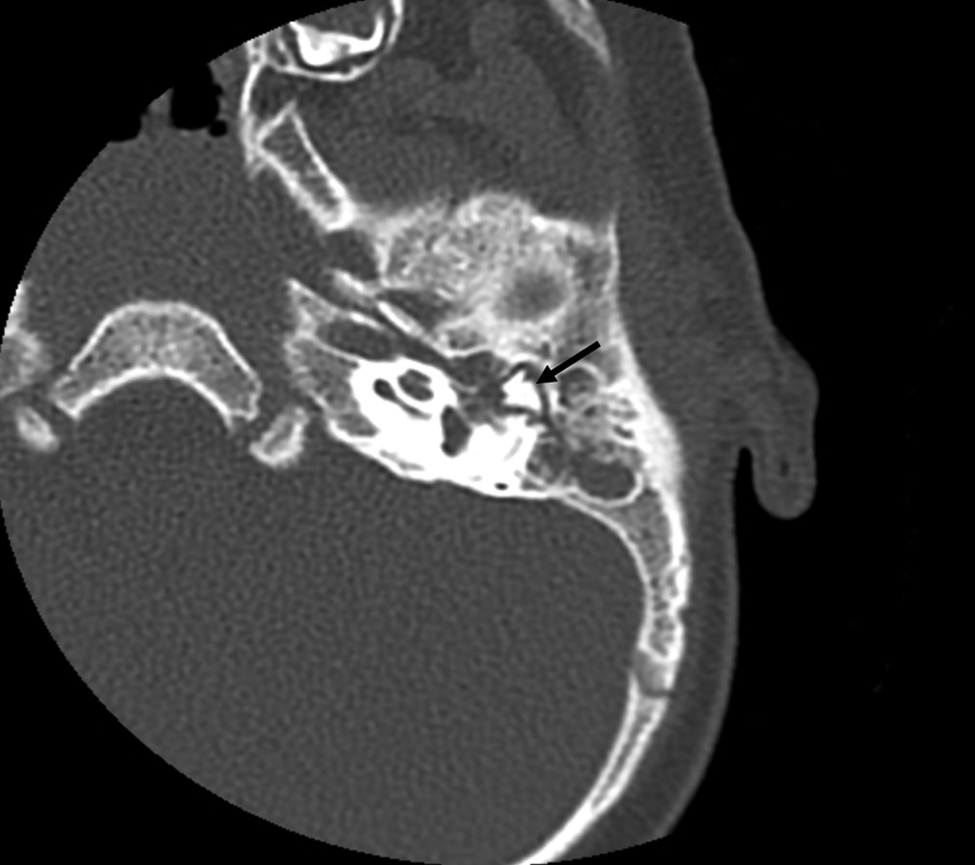
Position of facial nerve relative to the oval window (OW). If the horizontal portion was inferiorly positioned and possibly obstructing the OW, 0 points were assigned ( Figure 3A ). If the nerve was superior to the OW with no obstruction, 1 point was awarded.
Position of facial nerve relative to middle ear. If the mastoid portion turned anterior and lateral and possibly obstructed access to the middle ear space, 0 points were awarded ( Figure 3B ). If the nerve had the normal vertical course, 1 point was awarded.
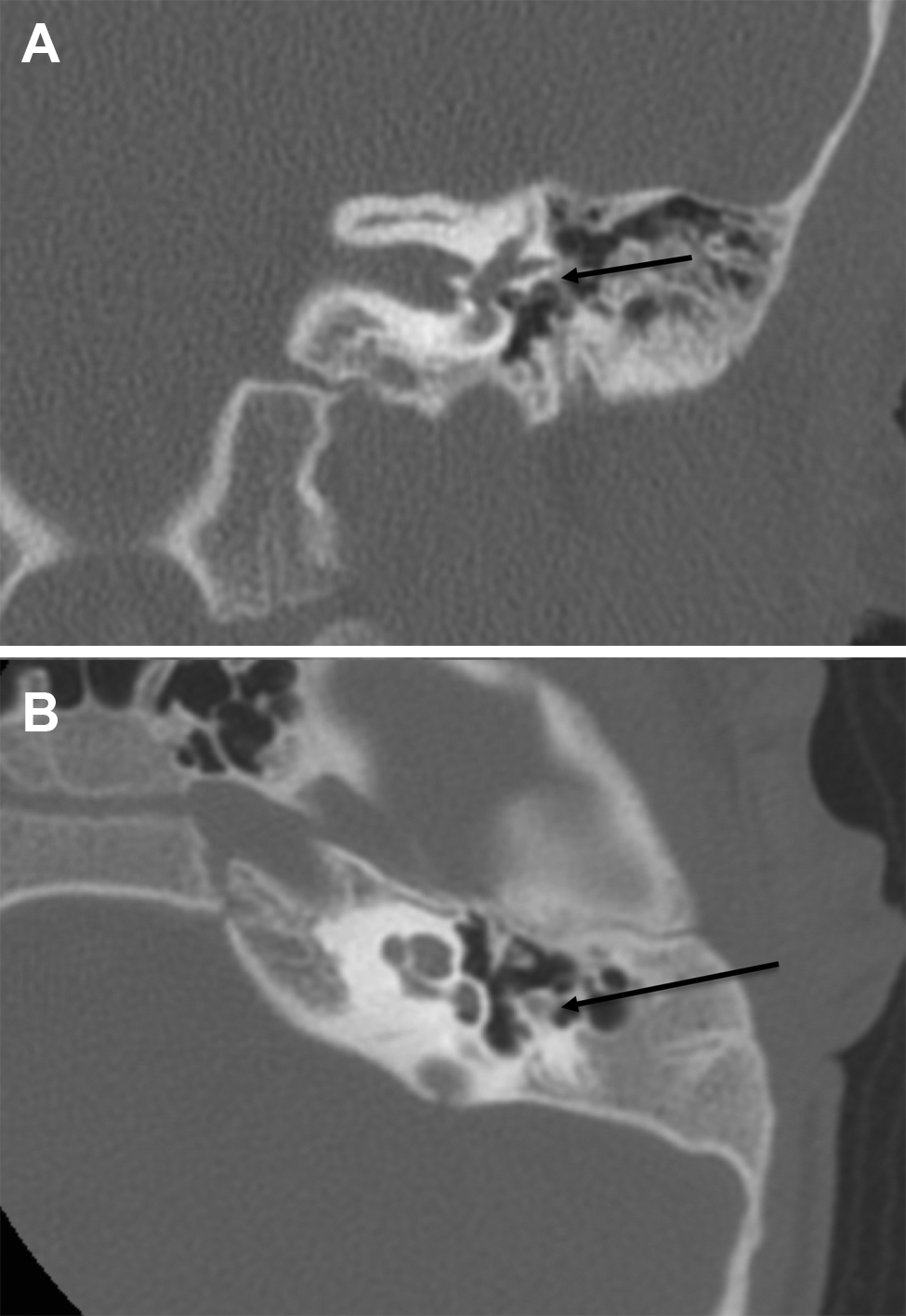
ISJ angle. We measured the angle on coronal sections at the level of the OW ( Figure 4A , B ).
Unfavorable tegmen position. (A) Moderate. Coronal computed tomography (CT) of the left temporal bone in a child with congenital aural atresia reveals a slight inferior displacement of the tegmen mastoideum. (B) Extreme. Coronal CT of the left temporal bone in a child with congenital aural atresia reveals a significant inferior displacement of the tegmen mastoideum.
Unfavorable malleus-incus complex (MIC) position. Axial computed tomography of the left temporal bones in a child with aural atresia shows a large MIC, which can obstruct the view of the incudostapedial joint (ISJ) and stapes. This anatomic variant makes assessing the ISJ and stapes integrity and mobility more difficult.
Unfavorable facial nerve position. (A) Coronal computed tomography (CT) of the left temporal bone shows the tympanic segment of the facial nerve overlying the oval window, which possibly causes obstruction of surgical access from a lateral approach. (B) Axial CT scan of the left temporal bone in a child with congenital aural atresia shows the mastoid portion of the facial nerve coursing anterolaterally, which could possibly obstruct access to the middle ear space during the lateral surgical approach.
Incudostapedial joint (ISJ) angle measurement. (A) Coronal computed tomography (CT) of the right temporal bone in a child with congenital aural atresia reveals an ISJ angle that measures 97°. (B) Coronal CT of the right temporal bone in a child with congenital aural atresia reveals an ISJ angle that measures 165°.
Results
CAA/EACS was identified in 98 patients. Of these patients, 32 (33%) had bilateral congenital anomalies, resulting in a total of 130 CT scans for review. Sixty-six (67%) were male, and 32 (33%) were female. There were 55 left (42%) and 75 right (58%) anomalies. The average age at time of CT scan was 4 years. Thirty-two (33%) patients underwent atresiaplasty. BAHA was performed in 15 (15%) patients, and 3 of these followed failed atresiaplasty.
We analyzed a total of 130 CTs of the temporal bones with both Jahrsdoerfer criteria and new/refined considerations. The prevalence of new considerations was as follows: significant obstruction by the tegmen with limited surgical access to epitympanum occurred in 5 (4%) ears. A milder inferior displacement of the tegmen with possible partial obstruction of surgical access to the epitympanum occurred in 17 (13%), and 108 (83%) ears had a normal tegmen position with no obstruction. The MIC was noted to be large and directly lateral to the stapes in 31 (24%) ears. In 53 (41%) ears, the facial nerve position was low-lying and unfavorable and would possibly obstruct surgical access to the OW, and in 27 (21%) ears, the position was unfavorable with possible obstruction of surgical access to the middle ear space. Eighty-four (65%) CT scans had a measurable ISJ angle, with a mean angle of 101° (range, 51°-155°). The average Jarhsdoerfer grade was 6, and the average grade including the new/modified criteria was 10.
All 32 operative reports were reviewed. A large MIC positioned directly lateral to the stapes was reported in 6 (19%) atresiaplasty patients. This large, lateral MIC reportedly blocked the view of the stapes and was a major operative finding reported to increase surgical difficulty due to the inability to assess integrity and mobility of the ISJ and stapes. Five of the 6 patients (83%) had a CT scan confirming these intraoperative anatomic MIC findings. In 22%, a facial nerve bony dehiscence was noted, but it did not interfere with the surgical procedure. Statistical multivariate analyses were performed to detect any possible associations between atresiaplasty hearing outcomes and all anatomic variants. No significant associations were noted, and thus these data are not presented.
Discussion
Jahrsdoerfer criteria is the most well-known anatomic grading system used to evaluate CT scans of CAA for surgical candidacy.4,9,10 The stapes is awarded 2 points as it is thought to be the most important factor. The other 8 anatomic factors are given 1 point each. If the course of the facial nerve is possibly obstructing and unfavorable for the atresiaplasty approach, no points are awarded.11-13
A total Jahrsdoerfer score of ≥6 allows consideration of atresiaplasty. 14 Multiple studies have validated the grading system by showing a correlation between higher grade and better atresiaplasty hearing outcomes.15-17 These studies did not report long-term hearing results. In contrast, Lambert reviewed 46 patients with long-term follow-up (1 to 7.5 years), which showed that 70% had a speech recognition threshold of <30 dB with <1 year follow-up, and 50% had similar results after >1 year follow-up. 18 Others have supported that some degradation in hearing occurs as patients are followed after their first postoperative year.18-20 Furthermore, Patel and Shelton 21 concluded that surgeon experience affected surgical outcome. Surgeons who performed at least 15 cases started to have better hearing results with atresiaplasty, with further improvement after 45 cases. 21
Approximately 33% of atresiaplasty patients undergo revision surgery.5,6 Most complications are restenosis, infection, persistent conductive hearing loss, and lateralization of the tympanic membrane graft. Rare complications include facial nerve injury and sensorineural hearing loss. Facial nerve injury has been reported in 1% to 7% and in 6% as a transient palsy.3,21-23 Sensorineural hearing loss was reported in 1% to 7.5%, most likely from excess transmission of energy through the ossicles from the drill.3,21-23
The BAHA is a low-risk alternative to atresiaplasty. It has yielded very predictable, reliable, long-lasting results with high patient satisfaction and improvement in quality of life. However, there are some potential disadvantages, including poor cosmesis, daily wound care, possible site infections, and possible need for revision surgery.24-27
Our pilot study described a modified grading system that expanded on Jahrsdoerfer’s criteria. In that study, we reviewed 32 CT scans and found 16% with inferiorly positioned tegmen, 38% with MIC directly lateral to stapes, 53% with facial nerve possibly obstructing access to the OW, and 16% possibly obstructing access to the middle ear space. 7 However, there was no correlation with surgical findings. In the present study, we reviewed the same and also analyzed ISJ angle in 130 CT scans.7,8
In contrast to the pilot study, in the present study we awarded 2 points for a normal, nonobstructing tegmen. If it was severely inferiorly displaced and thought to possibly significantly block surgical access, 0 points were given. A moderately low-lying tegmen was awarded 1 point if it had the potential to increase surgical difficulty by narrowing lateral approach surgical access but not necessarily make atresiaplasty impossible. Most patients (83%) had a normal position, while 4% were significantly inferiorly displaced and 13% had a milder inferior displacement.
The next anatomic consideration was facial nerve position. This is currently included in the Jahrsdoerfer grading system; however, his system did not initially specifically address the anatomic locations of obstruction. Jahrsdoerfer did discuss these 2 specific anomalies in subsequent publications.4,12,14,28 In our pilot study, the facial nerve possibly obstructed surgical access to the OW in 53% and possibly obstructed surgical access to the middle ear space in 16%. 7 The present study supports these earlier findings, with possible obstruction with respect to the OW and middle ear being 41% and 21%, respectively. This grading of the facial nerve at 2 locations may help in systematic grading of the nerve and for teaching of facial nerve anatomy.
Another important consideration was MIC position and size. The MIC normally is positioned anterolateral to the stapes, which allows good surgical access and visualization of the stapes and ISJ during the lateral atresiaplasty approach. However, if the MIC is large and directly lateral to the stapes, it may increase the difficulty of atresiaplasty. Additional time for drilling to view the stapes and ISJ is required, and visualization may still not always be possible because of this anatomic limitation. This potentially compromises the surgeons’ ability to assess the stapes and ISJ integrity and mobility. In the present study, we found 24% with an MIC that was large and lateral to the stapes. In the pilot study, we found 38% of the MICs were directly lateral to the stapes, but there was no evaluation of MIC size in the first study, which could account for the discrepancy in our findings. 7 In 6 operative cases, the MIC was obstructing the view of the stapes and ISJ and increased the difficulty of atresiaplasty according to the retrospective review of operative reports. In 5 (83%) of these patients, these intraoperative anatomic findings correlated with the CT scan grading. It is not clear why the CT was not 100% predictive of the difficulty of assessing the ISJ and stapes integrity and mobility when the MIC lies directly lateral to the stapes. Volume averaging, motion artifact, or some other unique unidentified anatomic factor may have been responsible for this discrepancy.
A recent study by Kim analyzed the ISJ angle of 181 ears, 149 of which had CAA. They found that patients with obtuse angles (>120°) had less favorable hearing outcomes than did patients with narrow angles (≤120°). 8 Only 65% of our population had an intact ISJ, and our measurements ranged from 51° to 155°, with a mean of 101°. We believe the measurement of the ISJ angle may be helpful in defining the 3-dimensional relationship of the ossicles with each other and the middle ear space. These factors may be important in surgical planning.
This study confirms the frequencies of new/modified anatomic considerations on temporal bone CT of patients with CAA/EACS that were originally reported in our smaller pilot study. 7 Awareness of these anatomic findings is useful for teaching temporal bone anatomy. Clinical correlation with some anatomic variations will never be possible. For example, one could never demonstrate poor hearing results of atresiaplasty in patients with significantly inferiorly displaced tegmen mastoideum since one would never operate on such anatomically unfavorable cases. The other anatomic points await validation with a larger cohort of atresiaplasty patients.
In addition, we were not able to demonstrate correlations between anatomic findings and hearing outcomes because of the small number of atresiaplasty cases, variable times of audiologic testing, and missing data. The retrospective nature of this study also has intrinsic limitations. Thus, surgical hearing outcome validation of the importance of the new/modified anatomic considerations was not possible in this study. Therefore, the study should be interpreted as a purely anatomic study, with the exception of the finding of increased intraoperative difficulties with a large obstructing MIC, which was intraoperatively reported to increase difficulty in viewing and assessment of ISJ and stapes integrity and mobility.
Conclusion
The decision of whether to perform an atresiaplasty has largely relied on the Jahrsdoerfer grading system as well as the surgeons’ careful scrutiny of the CT anatomy and ability for development of a successful surgical plan. We have prospectively identified new/modified anatomic considerations that occur frequently on CTs in a large cohort of patients with CAA/EACS. Review of surgical data shows that a large obstructing MIC makes stapes and ISJ viewing and assessment of integrity and mobility more difficult and thus increases the difficulty of atresiaplasty. A large obstructing MIC does not necessarily preclude atresiaplasty. The presence of these anatomic variants may influence the decision for or against atresiaplasty. A larger cohort of surgical candidates is needed to validate some of the anatomic findings.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.
This article was presented at the 2011 AAO-HNSF Annual Meeting & OTO EXPO; September 11-14, 2011; San Francisco, California.