
Abstract
Objective
To describe 2 subapproaches of the middle fossa approach: the transillumination method and transection of lines using the foramen spinosum, greater superficial petrosal nerve, and trigeminal impression to locate the malleus head for safe identification and decompression of the geniculate ganglion and facial nerve.
Study Design
Cadaver study.
Setting
A tertiary university hospital anatomy laboratory.
Subjects and Methods
The present study was conducted using 7 formalin-fixed cadaver heads (14 sides). A 0° endoscope was introduced into the external ear canal toward the posterosuperior quadrant of the tympanic membrane, after which transillumination was used to locate the malleus head. The brightest point indicated the convergence of the greater superficial petrosal nerve and a line drawn along the superior semicircular canal. An additional line was drawn parallel to the petrous ridge from the foramen spinosum and along the pathway of the greater superficial petrosal nerve. A third line connected the trigeminal impression to the zygomatic root. The area posterior to the intersection of these 2 lines separately with the third line was considered the zone of location of the malleus head. Among 17 patients undergoing surgery for facial paralysis between 1993 and 2011, transillumination was used in 6 patients to identify the malleus head to locate the geniculate ganglion.
Results
These techniques were proven to be reliable in locating the malleus head to find the geniculate ganglion in 14 dissected cadaveric temporal bones.
Conclusion
Two methods of locating the malleus head for facial decompression were defined.
The middle fossa lacks easily identifiable landmarks, which complicates the middle fossa approach and necessitates detailed knowledge of the anatomy of the temporal bone, petrous apex, and middle cranial fossa. William House 1 popularized the middle fossa approach for the resection of acoustic neuromas. Vestibular schwannomas are being diagnosed earlier as a result of increased clinical awareness and improved imaging modalities, making hearing preservation surgery a more realistic option for many patients. The middle fossa approach, one such surgical method, is one of several options for the treatment of vestibular schwannomas.
In traumatic temporal bone fractures with facial paralysis, the middle fossa approach is used when the transmastoid approach is not possible. Most techniques used to access the internal acoustic canal (IAC) are avoided when the facial nerve is the only structure to be exposed. Here, we describe 2 subapproaches to facilitate the middle fossa approach for facial decompression due to temporal bone fracture.
Materials and Methods
This study was conducted using 7 formalin-fixed adult cadaver heads (14 sides). All cadaver heads were dissected under 1× magnification. The head of the malleus (HOM) was located using the techniques described below, with distances and angles of crucial structures measured with calipers (accuracy ±0.05 mm) and goniometry (error 0.5°) independently by 2 authors. All measurements were repeated twice, and their average values were calculated. The study was approved by İzmir Katip Çelebi University Faculty of Medicine Local Ethics Committee.
Two methods were used to locate the HOM in order to find the geniculate ganglion. In the first method, a 0° endoscope was introduced into the external ear canal toward the posterosuperior quadrant of the tympanic membrane, and transillumination was used to locate the HOM. The brightest point indicated the convergence of the greater superficial petrosal nerve (GSPN) with a line drawn along the superior semicircular canal (SSCC; Figures 1 and 2 ). The arcuate eminence (AE) is one of the most commonly used landmarks in the middle fossa approach but is not always prominent, necessitating the use of other landmarks. The second method began with the identification of the middle meningeal artery (foramen spinosum) and the GSPN. Imaginary lines were drawn parallel to the petrous ridge from the foramen spinosum (x) and along the pathway of the GSPN (y). A line (z) originating from the trigeminal impression and passing through the zygomatic root (inner cranial table) was drawn, and the angle between this line and the petrous ridge was measured. The area located medial to (x), lateral to (y), and posterior to the convergence of line z with line y and x separately was defined as the safe zone for dissection and the identification of the HOM ( Figure 3 ).
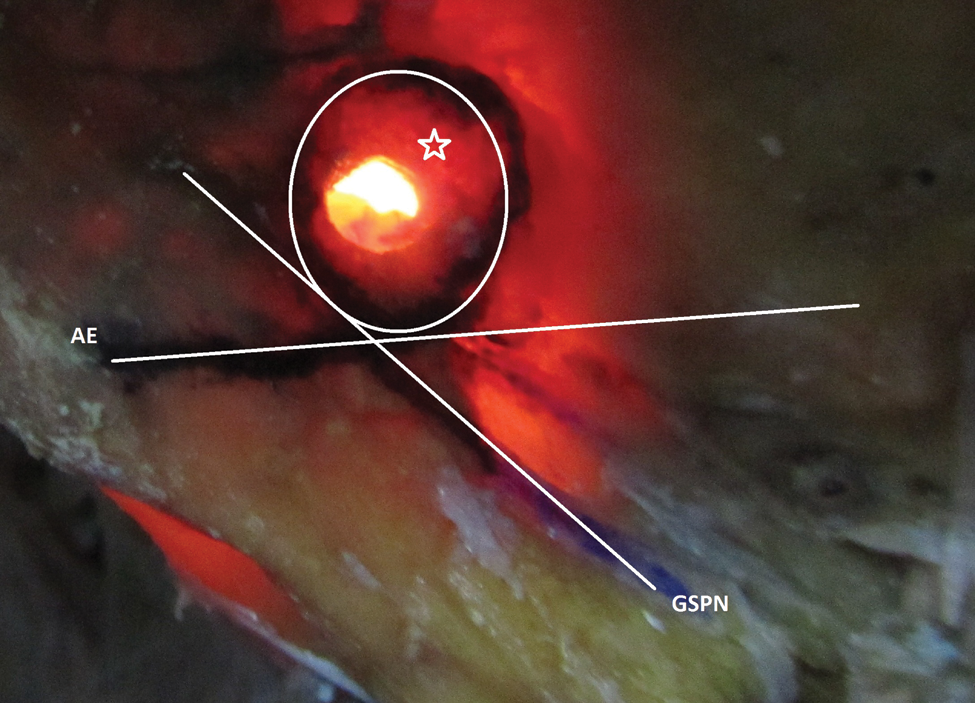
Transillumination method in a cadaver head. The convergence of lines drawn along the greater superficial petrosal nerve and along the superior semicircular canal. The encircled area (star) shows the safe point of entry to locate the malleus head. Left temporal bone as viewed from medial edge of middle fossa. AE, arcuate eminence; GSPN, greater superficial petrosal nerve.
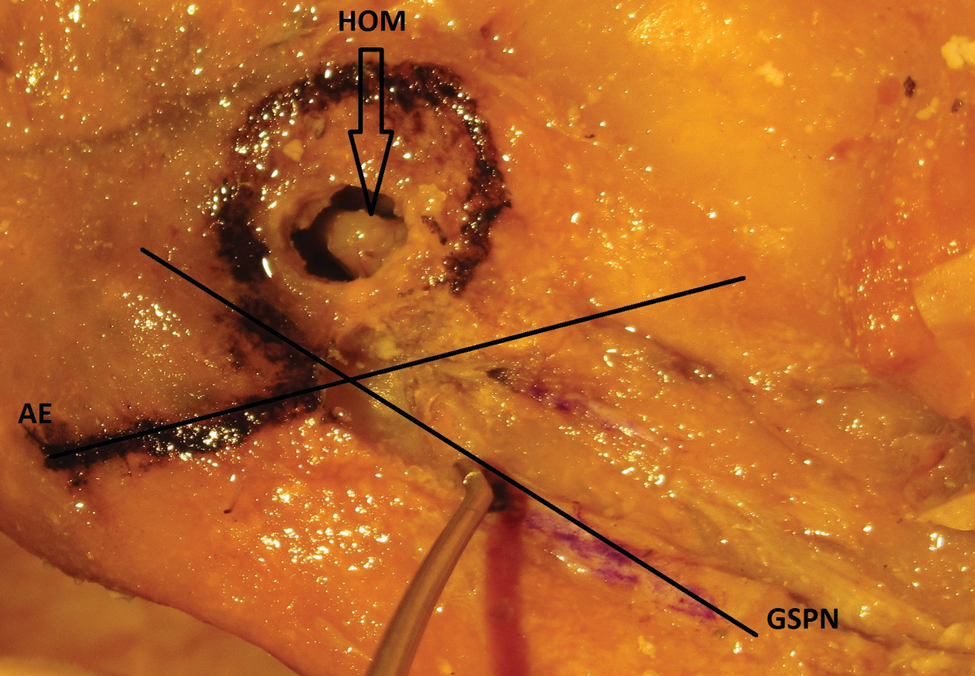
The convergence of lines drawn along the greater superficial petrosal nerve and along the superior semicircular canal. Head of malleus exposed. Left temporal bone as viewed from medial edge of middle fossa. AE, arcuate eminence; GSPN, greater superficial petrosal nerve; HOM, head of malleus.
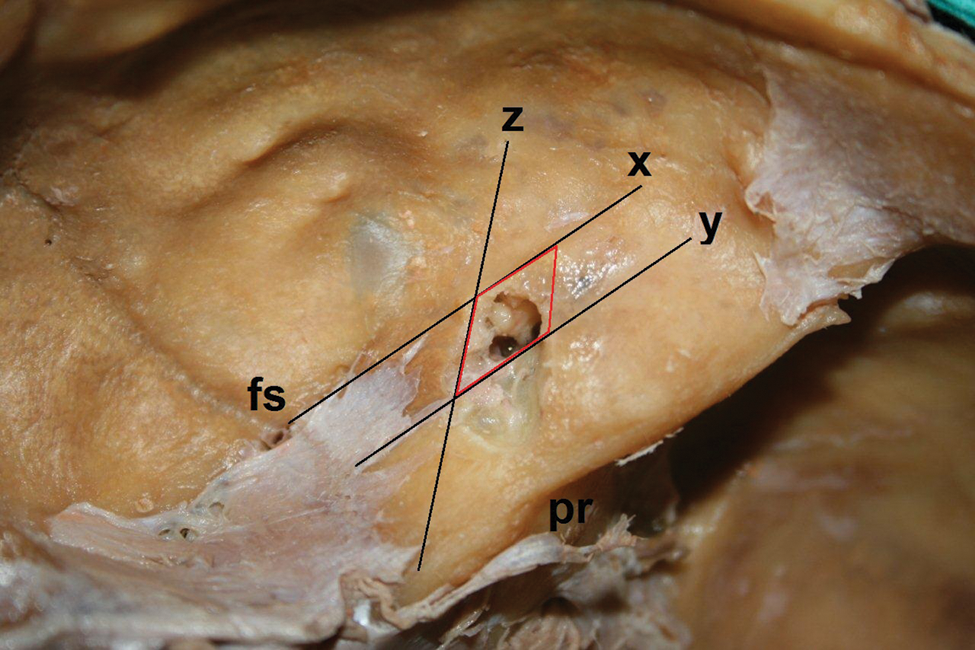
The red area shows the safe point of entry to locate the malleus head. The letter x denotes an imaginary line originating from the foramen spinosum and drawn parallel to the petrous ridge. The letter y denotes a line drawn along the pathway of the greater superficial petrosal nerve. The letter z denotes a line originating from the trigeminal impression and passing through the zygomatic root (inner cranial table). Right temporal bone as viewed from medial edge of middle fossa. fs, foramen spinosum; pr, petrous ridge.
We measured certain distances that may be important for the described procedures—namely, the distance between the HOM and (1) the most prominent point of the AE, (2) the foramen spinosum, (3) the horizontal semicircular canal, (4) the cochlea, (5) the geniculate ganglion, (6) the acoustic porus (AP), (7) the closest segment of the tympanic branch of the facial nerve, (8) the zygomatic root (measured from the inner cranial table), and (9) the petrous ridge.
Statistical Analysis
SPSS software (version 16.0 for Windows; SPSS, Inc, an IBM Company, Chicago, Illinois) was used for statistical analysis. The Mann-Whitney U test was used to evaluate differences between the left and right sides. A P value <.05 was considered statistically significant.
Results
We defined 2 methods to locate the HOM in order to find the geniculate ganglion for facial decompression via the middle fossa approach. We also measured distances between structures that might be important for these procedures ( Table 1 ).
Distances between HOM and Several Important Structures Critical for Surgical Procedures Described
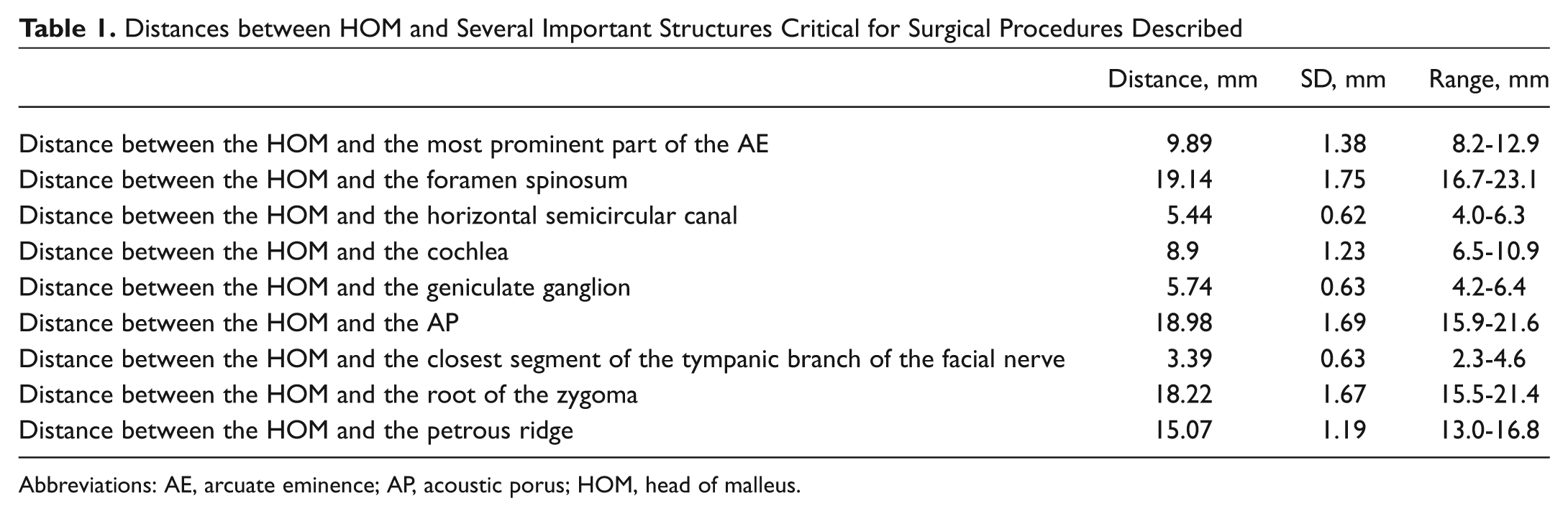
Abbreviations: AE, arcuate eminence; AP, acoustic porus; HOM, head of malleus.
No difference in these measurements was identified between the right and left sides (P > .05). On the introduction of an endoscope into the external ear canal, the brightest point indicates the convergence of the GSPN and a line drawn along the SSCC. This convergence creates a mean (SD) angle of 124.34° (7.0°; range, 110°-135°).
An imaginary line (z) originating from the trigeminal impression and passing through the root of the zygoma (inner cranial table) was drawn, and the angle between this line and the petrous ridge was measured. The mean (SD) value was 41.3° (4.12°; range, 35°-48°).
In both methods after the HOM was exposed, the cochleariform process was identified, and a second portion of the facial nerve was visualized. The geniculate ganglion was reached by following the tympanic segment of the facial nerve.
Clinical Cases
Between 1993 and 2011, we operated on 17 patients with temporal bone fractures and facial paralysis using the middle fossa approach. All operations were performed by the senior author (H.K.). In the last 6 cases, the HOM was located using the transillumination method in a manner similar to other techniques described in the literature. 2 The HOM was the primary landmark used to locate the geniculate ganglion. No cerebrospinal fluid leak, meningitis, or brain herniation was seen.
Discussion
Decompression of the facial nerve in patients with temporal bone fracture can be performed by a transmastoid approach or a middle cranial fossa approach. The transmastoid approach is attempted first, and if this technique is inadequate, the middle fossa approach may be used. The middle fossa approach is a challenging technique that relies on poorly discernible landmarks that are risky to identify on surgical dissection.
Several studies have investigated the use of various landmarks to guide access to the IAC and facial nerve in middle fossa surgery. House 1 located the GSPN and traced it posteriorly to identify the geniculate ganglion and IAC. However, the GSPN is often difficult to identify where it exits the facial hiatus. Later, Fisch 3 proposed the use of the AE to locate the SSCC. He further described the use of a 60° angle between lines drawn through the SSCC and IAC, respectively. Garcia-Ibanez and Garcia-Ibanez 4 demonstrated that the intersection of a line drawn along the course of the GSPN exiting the facial hiatus with a line drawn through the SSCC creates an angle that approximates the position of the IAC. Both techniques require drilling the SSCC and, therefore, carry the risks of inadvertent fistulization, sensorineural hearing loss, and vertigo.
Catalano and Eden 5 proposed the use of the lateral cortex of the temporal squamosa at the zygomatic root to locate the HOM as an external reference for IAC identification. The distance from the HOM to the zygomatic root was 18 mm. They then identified the IAC using the House, Fisch, or Garcia-Ibanez method. The lateral end of the IAC was consistently 7 to 8 mm medial to the HOM. They revealed that the HOM lies along a line drawn between the zygomatic root and the IAC. Lee and Lee 6 also used the HOM to identify the geniculate ganglion and trace the facial nerve to locate the IAC and found it to be a reliable and consistent landmark. They especially focused on finding a method of identifying the geniculate ganglion that avoids the risk of inner ear damage and investigated the relationships among the HOM, IAC, and geniculate ganglion. They recommend the use of their technique in all cases in which surgically tracing the facial nerve to the IAC is planned through a middle fossa approach, including vestibular nerve section and intracanalicular acoustic tumor surgery. Exceptions include pediatric cases and cases with severe temporal bone fracture with ossicle dislocation.
Miller and Pensak 7 presented reference data for locating and delineating petrous structures critical to middle fossa surgery. The intersection of two 19-mm arcs drawn from the zygomatic root and the foramen spinosum approximates the location of the HOM. Thus, they used the root of the zygoma, an extratemporal landmark, to consistently find an intratemporal landmark, the HOM. They found that a line drawn from the root of the zygoma to the HOM can be used to identify the IAC and the AP.
The AE is one of the most commonly used landmarks in middle fossa surgery.3,4 However, Kartush et al 8 doubted the reliability of the AE as a guide to the SSSC, stating that the AE may be featureless and difficult to identify on the middle fossa in about 15% of cases. Although the AE can be identified in 85% of patients, the SSSC deviated from the AE in 50% of cases. 8
Here, we present one novel and one modified technique for the middle fossa approach. The foramen spinosum, trigeminal impression, and GSPN were used to locate the HOM. As described, 3 imaginary lines were drawn from the foramen spinosum parallel to the petrous ridge, along the GSPN, and between the trigeminal impression and the zygomatic root. The area posterior to the intersection of these 2 lines separately (the line drawn from foramen spinosum parallel to the petrous ridge and the second line along the GSPN) with the line between the trigeminal impression and the zygomatic root was proven to be a safe and reliable drilling zone in 14 dissected cadaveric temporal bones. It is important to avoid drilling medial to the imaginary line along the GSPN or lateral to the imaginary line drawn from the foramen spinosum. This technique is most useful when the AE is obscured.
The second method can be used when no landmark can be identified. A 0° endoscope is inserted into the external ear canal. The brightest point in the middle fossa approach represents the HOM topographically. This technique was first reported by Kobayashi and Nakao. 2 We confirmed that the brightest point matched the location identified by the angle created by the convergence of imaginary lines drawn along the paths of the GSPN and SSSC. No such relationship was reported in Kobayashi and Nakao’s article. This convergence creates a mean (SD) angle of 124.34° (7.0°) (range, 110°-135°). We confirmed this technique in 14 dissected cadaveric temporal bones and in 6 patients in whom we used the middle fossa approach to treat temporal bone fracture with facial paralysis. As stated by Bento et al, 9 this approach avoids the risk of complications (cerebrospinal fluid leak, meningitis, brain herniation) inherent in opening a space in the tegmen tympani because it does not require entry into the dura or IAC. We encountered no such complication in our subjects.
In both techniques, knowledge of anatomic relationships is mandatory. Location of the HOM can be justified using external and internal reference points (in our study, the distance between the HOM and the root of the zygoma was 18.22 mm, the distance between the HOM and the petrous ridge was 15.07 mm, and the distance between the HOM and the foramen spinosum was 19.14 mm). Using these measurements with the techniques described makes identification of the HOM more accurate. After the HOM is exposed, avoiding complications is the main task for a surgeon. The relationships of important structures must be kept in mind (in our study, the distance between the HOM and the horizontal semicircular canal was 5.44 mm, the distance between the HOM and the cochlea was 8.9 mm, the distance between the HOM and the geniculate ganglion was 5.74 mm, and the distance between the HOM and the closest segment of the tympanic branch of the facial nerve was 3.39 mm) to avoid dreadful complications.
Although our cases consisted of patients with temporal bone fractures, the transillumination technique should be used with caution in traumatic cases because the fracture line may blur or disseminate the brightest point.
Conclusion
The middle fossa approach is a complex surgical technique, and no technique can be regarded as easy. We confirmed both techniques in 14 dissected cadaveric temporal bones and the transillumination technique in 6 patients in whom we used the middle fossa approach to treat temporal bone fracture with facial paralysis. The techniques described here simplify the middle fossa approach. Both methods can be used concurrently with the techniques in the literature for a more reliable identification of the HOM.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.