
Abstract

Desmoid tumors are rare nonmetastasizing fibrous lesions that tend to invade locally. 1 The main treatment for desmoids is wide local excision, 2 but incomplete resection of the tumor margin occasionally occurs, resulting in relapse and the need for repeat operation. Chemotherapy and radiotherapy have been attempted with good responses for unresectable or recurrent lesions,1,2 but the side effects may offset the advantages. We present a case of desmoid tumor in the neck region. Hyogo Cancer Center Institutional Review Board approval and informed consent were obtained. This patient underwent 5 operations, but the tumor continued to relapse after every surgery. Intriguingly, the tumor finally regressed after the use of a nonsteroidal anti-inflammatory drug (NSAID) for neck pain.
Case Report
The patient was a 53-year-old man who first presented with nasal obstruction and dyspnea at our institute in 1997. Otolaryngologic examination revealed a mass occupying the left side of the neck from the oropharyngeal to hypopharyngeal wall. Computed tomography (CT) scan and magnetic resonance imaging (MRI) showed a 6-cm well-enhanced left parapharyngeal mass ( Figure 1 ). The first operation was performed to alleviate the nasal obstruction and dyspnea and to determine the diagnosis. The tumor expanded from the superficial aspect of the omohyoid muscle to the left prevertebral space. The patient underwent en bloc resection of the mass. Histologically, the mass was diagnosed as a desmoid tumor. Although the deep margins of the resected mass were microscopically positive for tumor, the patient did not pursue any further adjuvant therapy. Subsequently, the tumor recurred 4 more times within a span of 5 years (first tumor detection was in 1997, the last one in 2002), and dyspnea appeared with each mass growth; thus, further excision was performed for each regrowth. However, despite the repeated excisions, the regrowths could not be totally removed, and the frequency of local recurrence after excision remained high. Because the patient did not wish to undergo further surgery, we decided on an observational approach. During the next 4 years, with the subsequent gradual increase in tumor size, the patient experienced increasing neck pain; thus, oral NSAID (diclofenac, 50 mg twice daily) administration was initiated in 2006. During the next 2 years, diclofenac was continued without any evidence of side effects, and interestingly, the lesion slowly decreased in size, such that the patient became free from neck pain. He does not currently take NSAIDs, the residual tumor is not palpable, and CT showed regression of the lesion with poor enhancement ( Figure 2 ).
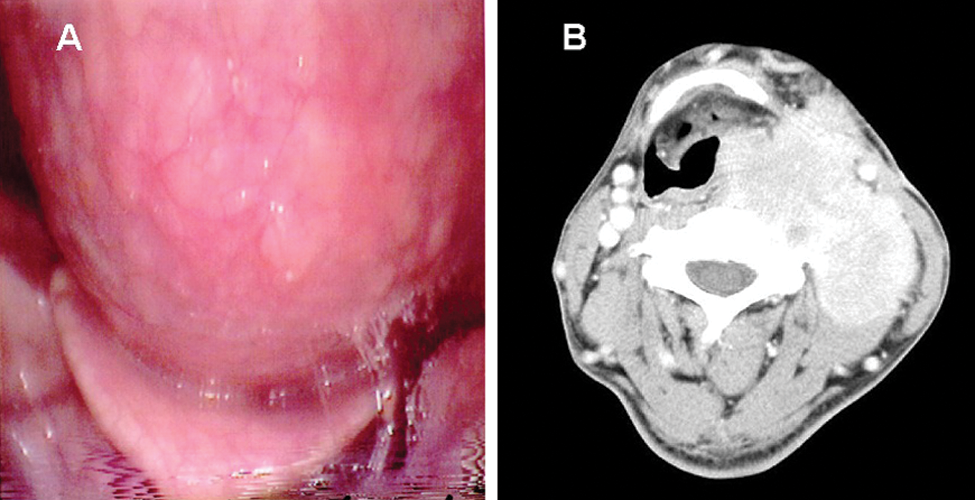
(A) The tumor displaced the oropharyngeal posterior wall, and the upper airway became stenosed. (B) A computed tomography scan demonstrated a well-enhanced mass in the left neck region. This figure was taken after several surgeries but before administration of nonsteroidal anti-inflammatory drugs.

(A) The tumor is no longer palpable upon inspection. (B) A computed tomography scan demonstrated scarring of the tumor. This figure was taken after administration of nonsteroidal anti-inflammatory drugs.
Discussion
Desmoid tumors are locally aggressive and frequently invade surrounding structures; therefore, local control is difficult to achieve in terms of preservation of function. Surgical resection, including a wide margin, is the standard treatment modality of desmoid tumors.1-3 If positive margins are found after surgery, subsequent local control by radiotherapy is preferred. 3 By contrast, the efficacy of NSAIDs and antiestrogen medication in the treatment of desmoid tumors has been reported by some investigators.4,5 In this case, the patient did not opt for irradiation of the tumor; therefore, symptomatic therapy with NSAIDs was administered. We sought to evaluate the relationship between the CT images taken before and after 11 years, the first one at initial presentation in 1997 and a subsequent one during the follow-up period after NSAID treatment, respectively. A CT taken before NSAIDs demonstrated a huge mass with a well-enhanced interior; however, following drug administration, the tumor underwent a remarkable shrinkage with a poorly enhanced interior. Tumors that are strongly enhanced before therapy consist of densely distributed fibroblasts and tumor blood vessels with abundant collagen fibers. On the other hand, regressed tumors that are poorly enhanced displace the consolidated and scarring tissue with collagen fibers, poorly formed blood vessels, and fibroblasts. Several reports indicate the possibility that endogenous prostaglandin synthesis may play a role in fibroblast and tumor blood vessel growth.2,4,5 Nonsteroidal anti-inflammatory drugs are reported to be effective in desmoid tumors through their inhibition of prostaglandin synthesis. 5 The results of this case demonstrate that administration of NSAIDs twice or more a day leads to tumor shrinkage, which is sustained even after discontinuation of treatment. In conclusion, we report that NSAIDs may promote shrinkage of desmoid tumors as evidenced by CT. Thus, in unresectable cases of desmoid tumors, NSAIDs may be an effective therapeutic alternative in combination with surgery.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.