
Abstract
Objectives
The aim of the study was to gather information on outcomes and effect sizes of 2 surgical methods of glossectomy by using a grade system and an objective measure of artifacts in micrometers (µm). The collected data would be used to plan a definitive study.
Study Design
Pilot study.
Setting
Tertiary referral center.
Material and Methods
Nineteen patients affected with tongue cancer were consecutively enrolled in a pilot study and treated by partial glossectomy. Eleven patients (57.89%) of group A were treated with monopolar electrocautery, while 8 patients (42.10%) of group B were treated with Harmonic Focus Curved Shears. Specimens were examined by a pathologist blinded to the surgical procedure, using a 4-grade system for margin artifact assessment (margin fragmentation, cautery/crush artifact, extravascular blood clot, capillary congestion) and for measuring artifact depth.
Results
Artifact depth was more relevant in group A (765,633 µm) than in group B (473,939 µm). The difference between groups was significant at the 95% confidence interval (P < .0001). Margin fragmentation and capillary congestion compared between the 2 groups were of no significance. There were less cautery/crush artifacts and extravascular blood clots observed in the harmonic shears group.
Conclusion
When used to perform a partial glossectomy, Harmonic Focus Curved Shears produce less cautery/crush artifact and a smaller artifact depth compared with monopolar cautery.
Cancer of the oral cavity is the eighth most common tumor worldwide, and 300,000 new cases are reported each year. 1 Tongue cancer is the most frequent cancer of the oral cavity. The incidence rate is 4.3 out of 100,000 in males and 1.7 out of 100,000 in females, with existing broad geographical differences. 2 The frequency of the cancer of the oral cavity is increasing, especially in the younger population due to a correlation with human papillomavirus infection.3,4
Primary surgical treatment of the T1-T3 anterior two-thirds of the tongue is recommended.5,6 It is the most frequent procedure performed in oncological centers. However, tongue surgery must abide by and respect the following key parameters: wide excision with clear margins, good hemostasis, and preservation of function. An accurate evaluation of margin status is required to quantify the minimal distance of the tumor from margins or margin infiltration, depth and pattern of invasion, perineural invasion, and lymphocytic response. These issues are crucial for the prognosis and in the decision-making process regarding adjuvant treatments.7-9
Different surgical instruments are available for performing various types of glossectomy. These include cold steel scalpel and scissors, monopolar and bipolar electrosurgery, laser (carbon dioxide, argon laser, etc), ultrasonic scalpel, and shears. Monopolar cautery is the most commonly used cutting tool in head and neck surgery. By and large, it facilitates cost-effectiveness, availability, and maneuverability. However, there are some limitations associated with its use in terms of thermal damage such as wound healing and crust formation. 10
In applying various surgical techniques, there are different histological features that have a direct relationship between tissue distortion at the surgical margin and hemostasis. Cold steel scalpel creates less tissue distortion; however, adjunctive measures are needed in case of hemostasis, including ligation, transfix suture, and cautery, that could interfere with clinical healing.
Kirakala et al 11 reported the approach of assessing margin distortion for glossectomy in a rat model.
To our understanding, the evaluation of histological features after carrying out a glossectomy and the measurement of artifacts in micrometers have not yet been described in humans during surgery. The purpose of this pilot study was to gather information on outcomes and effect sizes of 2 surgical methods of glossectomy (monopolar cautery and harmonic shears) translating into human practice the trial in the rat model. The collected data would be used to plan a definitive study.
Materials and Methods
Between January 2009 and December 2010, a total of 129 patients with tongue carcinoma were treated at the Department of Otolaryngology–Head Neck Surgery of the National Cancer Institute, Rome, Italy. Among all the patients with tongue carcinoma, 19 were included in the study and considered eligible for a hemiglossectomy (transoral or “pull-through” approach). Patients treated with a procedure more or less aggressive than those described were excluded. Previously irradiated patients were also excluded. There were 10 male and 9 female patients (male/female ratio: 1.1). The mean age was 59 years. Tumors were clinically staged as 8 T1 (42.1%), 10 T2 (52.6%), and 1 T3 (5.3%) according to the 2009 TNM classification. 12 All patients were affected by histology proven squamous cell carcinoma of the lateral border of the mobile tongue. Surgical treatment consisted of hemiglossectomy (performed with a transoral excision) in 17 patients (89.5%) and pull-through operation in 2 patients (10.5%). The final pathology report documented well-differentiated carcinomas in 3 (15.8%) cases, moderately differentiated carcinomas in 10 (52.6%) cases, and poorly differentiated carcinomas in 6 (31.6%) of the 19 cases.
Patients were divided into 2 groups. Eleven patients of group A (57.89%) were treated with monopolar electrocautery (KLS Martin ME400 Gebrüder Martin GmbH &Co, KG Tuttlingen-Germany), while for the 8 patients in group B (42.10%), the Harmonic Focus Curved Shears (Ethicon Endo-Surgery, Inc, Cincinnati, Ohio) were adopted.
All patients were operated on by the same experienced attending surgeon. Cutting with a coagulation current using monopolar electrosurgery was set at a power of 40 W (cutting modality) adopting a standard tip to complete the excision.
In the ultrasonic shear group, the tongue was grasped at the mucosa incision line between the curved shears of the handpiece and control was activated at a power level of 3.
The advocation of a minimum free margin of resection was 1.5 cm, 13 and the line of resection was outlined by blue dye at the beginning of the operation. This study was approved by the local ethics committee of the National Cancer Institute Regina Elena of Rome (n. 11/07/R/9).
Histopathologic Comparison
Specimens were inked at the cut margin, oriented, fixed in formalin 10%, and embedded in paraffin. The blocks were serially sectioned (3 µm deep) and slides stained with hematoxylin and eosin. Slides were reviewed by a pathologist blinded to the surgical procedure. Margin distortion in these different surgical techniques was quantified by a grading scale. Three adjacent 25× fields were examined.
The subtypes of evaluated margin distortion were margin fragmentation, cautery/crush artifact, extravascular blood clot at the cut margin, capillary congestion, and artifact depth. A 4-grade scale for margin distortion was adopted as follows: grade 0 (no distortion at margins), grade 1 (distortion from 1% to 25% of margin), grade 2 (distortion from 26%-50% of margin), and grade 3 (distortion greater than 51% of margin). 11
Margin fragmentation was defined as either partial or complete disruption of tissue from the inked edge. Cautery/crush artifact was defined as a marked distortion of cells and/or streaking of nuclei. An extravascular blood clot at the cut margin was defined as blood outside vessels at the inked margins. Capillary congestion was considered as red blood cells crowding capillary beds. Artifact depth was the mean of 3 measurements as the greatest depth of any tissue distortion in micrometers (µm) and was measured by digital optical Leika DM 2000 (Leika Application Suite V3.2.0).
Statistical Analysis
Descriptive statistics were used to summarize pertinent study information. The association was analyzed by the Fisher exact test. Comparisons between harmonic shears and monopolar electrosurgery were carried out for different variables using the Mann Whitney U test (not parametric test). The level of significance was set at P ≤ .05.
SPSS software (SPSS version 18.0, SPSS Inc, Chicago, Illinois) was used for all statistical evaluations.
Results
The mean grade of cautery/crush artifacts was 2.64 (range, 1-3; SD, 0.674) in group A and 1.75 (range, 1-3; SD, 0.707) in group B. The difference between the 2 groups was significant (P = .01).
The extravascular blood clot at margin was lower in group B (mean of grading, 0.38) than in group A (mean of grading, 1.09; P < .02).
The mean artifact depth in group A was 765,633 µm (median, 778,580; range, 550,450-954,922; SD, 186,307), while in group B it was 473,939 µm (median, 456,497; range, 388,981-571,988; SD, 85,865; Figure 1 ). The difference between groups was significant in the nonparametric tests (Mann Whitney U test, P < .0001; Table 1 ; Figures 2 - 3 ).

Comparison of surgical techniques with respect to tissue margin distortion.
Difference between Groups in Nonparametric Test a
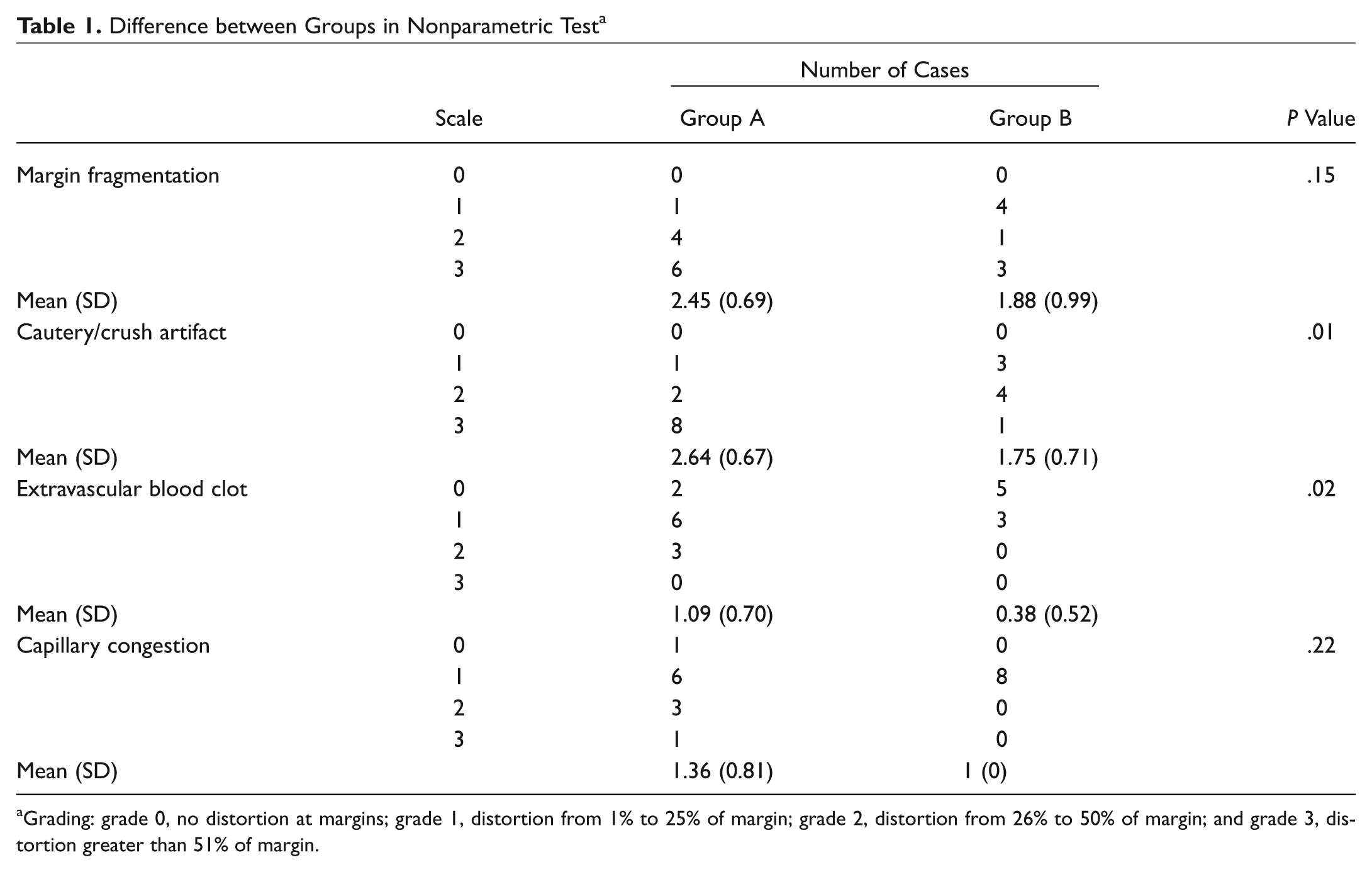
Grading: grade 0, no distortion at margins; grade 1, distortion from 1% to 25% of margin; grade 2, distortion from 26% to 50% of margin; and grade 3, distortion greater than 51% of margin.
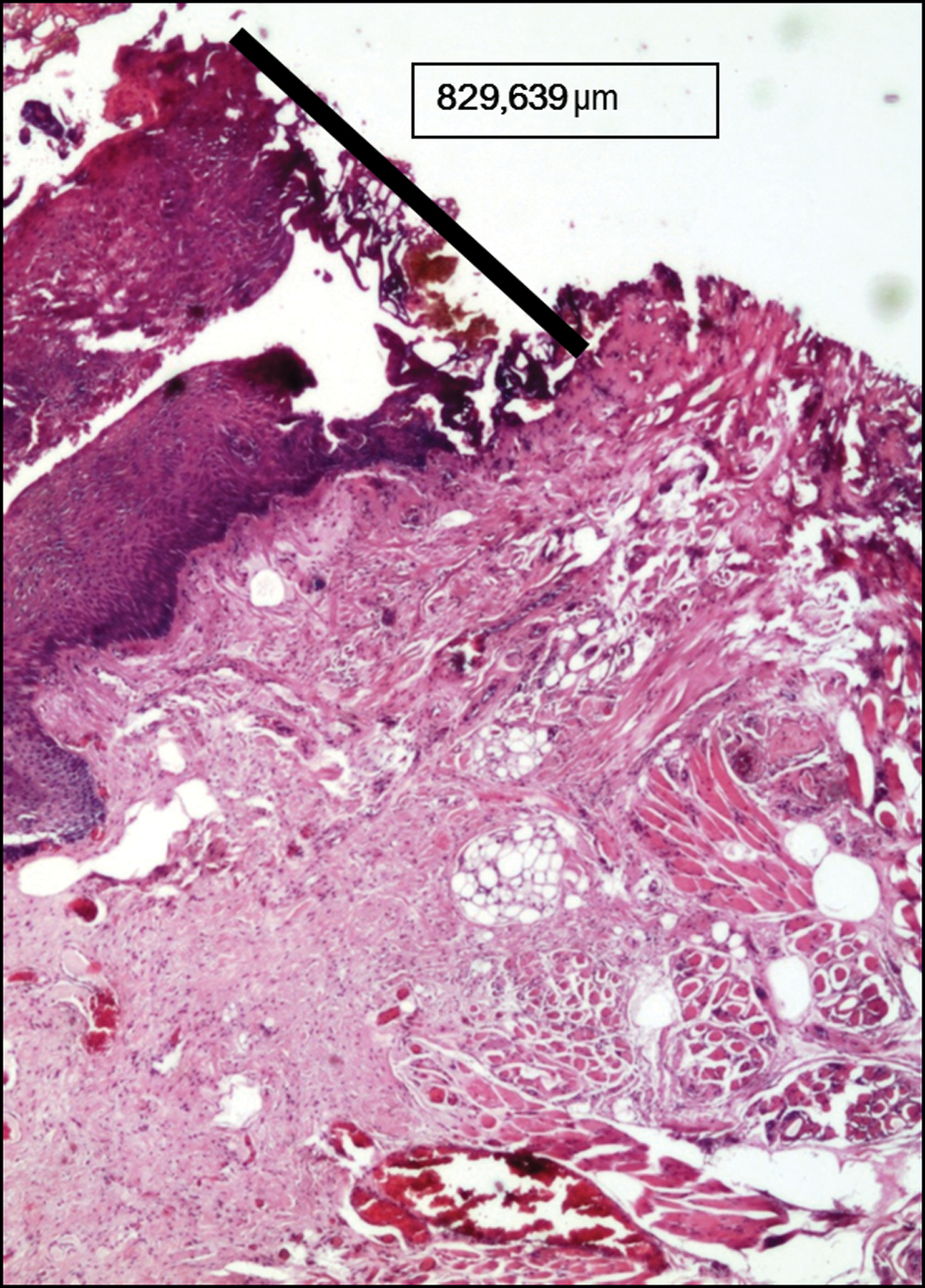
Margin fragmentation (hematoxylin-eosin 25×) monopolar.
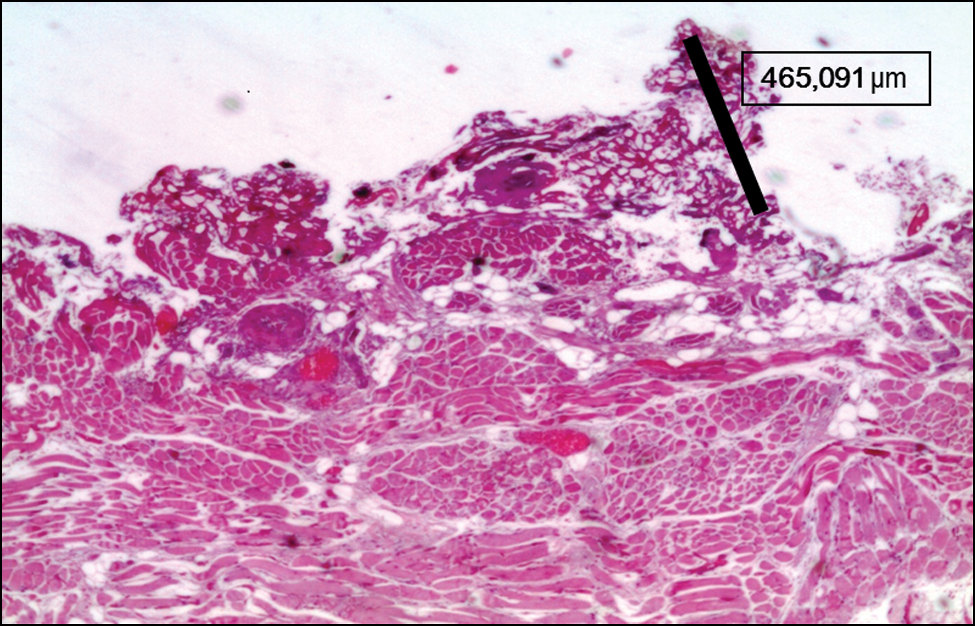
Margin fragmentation (hematoxylin-eosin 25×) harmonic shears.
No statistical significance was observed between group A and group B, according to margin fragmentation (P = .15) and capillary congestion (P = .22).
The mean margin clearance was 15 mm for group A and 1.4 mm for group B (P > .05).
Table 2 and Figure 1 show the results of the comparison of surgical techniques with respect to tissue margin distortion.
Comparison of Surgical Techniques with Respect to Tissue Margin Distortion

Discussion
The development of an ultrasonically activated coagulating scalpel in the early 1990s has provided an alternative method in performing dissections. This device divides tissue by using high-frequency (55,000 Hz) ultrasonic energy transmitted between the instrument blades. The active blade of the instrument vibrates longitudinally against an inactive blade over an excursion of 50 to 100 µm 14 by disrupting tertiary hydrogen bonds within the tissue. 15 This takes place at a relatively low temperature (80°C), causing less tissue injury than the other adopted techniques.16,17 Given that the water part of the tissue does not reach the boiling point, the relatively mild increase in temperature causes the proteoglycans and the collagen fibers in the tissues to become denatured and mix with intracellular and interstitial fluids to form a gluelike substance (a coagulum). 18
The generation of local water vapor was questioned for triggering the release of cancer cells. However, it is demonstrated by animal studies that viable air-borne cancer cells are not released by using a harmonic scalpel. 19
The fact that the shaft of the instrument remains cool and there is no electrical current conducted through the handpiece may decrease the risk of inadvertent injury to surrounding structures such as the lingual nerve or the hypoglossal nerve at the time of the hemiglossectomy. This was not demonstrated in the present study, but because it was demonstrated for the facial and the inferior laryngeal nerves, it seems reasonable to think that it could be safe also for the lingual and hypoglossal nerves.20,21 In addition, it does not interfere with any external or implanted stimulators (pacemaker, defibrillation devices, cochlear implants, etc). 22
The device is used by switching between 2 modality buttons present on the handle; maximum power mode for cutting is indicated by the number 5 on the device, and the minimum power level for coagulation is indicated by the number 3.
The benefits of simultaneous hemostasis and cutting would facilitate the surgery without interruption for hemostasis even with clear margins and a bloodless field. The most critical aspect in surgical resection is deep and posterior margins, especially for deep infiltrations or an ill-defined tumor edge with islands of tumor cells in advance of clinical tumor edge.
To better identify larger vessels and the lingual artery, it is recommended to avoid a large section of tissues using harmonic scissors and perform a step-by-step technique. 23
Monopolar electrosurgery works by alternating electrical current with various frequencies applied to the patient’s tissue according to Joule’s law of thermodynamics in which the relationship of the amount of heat to the electric current (I), the ohmic resistance (R), and the duration (t) is expressed as H = I2 × R × t. Electric charge is absorbed by molecules, which leads to a heating of the tissue to an average of 300°C to 400°C. This results in disruption by either boiling or coagulating, depending on the settings and application of the device. It is important to note that the amount of heat dissipated (blood flow) can reduce the temperature generated at the active electrode. 24 This heat-based mechanism of action is responsible for the comparatively large zone of tissue injury adjacent to the surgical incision. 25 Monopolar cautery requires an adjunctive procedure for hemostasis. This mechanism seems to be associated with postoperative scar contractures, wound-healing delay, and postoperative pain.26,27 In monopolar electrosurgery, current flow interferes with electrostimulator devices such as pacemakers, implanted programmable defibrillators, and so forth, as reported by the company.
The device artifacts described in this study are relevant especially in specimens after monopolar cautery. Ultrasonic scalpels created less tissue distortion than monopolar electrosurgery. Margin fragmentation did not show any statistically significant differences between the 2 groups (mean, 2.45 vs 1.88; P = .15). Given the type of technique used, these data show that both of the procedures were expected not to cause trauma at the surgical margin in terms of fragmentation because they are more ergonomic and thus less tiring.
Furthermore, there were no differences between the 2 techniques in terms of capillary congestion (blood cells crowding capillary beds) probably due to a similar hemostatic effect.
Numerous studies on formalin fixation of head and neck cancer evaluated the margin of shrinkage from in vivo to in vitro. In an animal study, Johnson et al 28 found that the mean shrinkage rates of the lingual surface, deep tongue, and labiobuccal mucosal margins were 30.7%, 34.5%, and 47.3%, respectively. In another study on oral cancer, Mistry et al 29 showed that the mean shrinkage rates of the tongue and buccal mucosa margins were 23.5% and 21.2%, respectively, whereas the mean shrinkage rates of the margins in T1/T2 and T3/T4 tumors were 25.6% and 9.2%, respectively.
Cheng et al, 30 in their study on margin discrepancy in oral squamous cell carcinoma, found that the mean discrepancy rates in buccal mucosa, mandibular alveolar ridge, and retromolar trigone margins were 71.90%, 53.33%, and 42.14%, respectively. So, this issue should be considered by the pathologist at the moment of the margin evaluation.
According to our data, there was no difference between the 2 groups in terms of margin clearance, but artifact depth was present with a mean of 781,877 µm in the electrocautery specimen group and 443,410 µm in the harmonic shears group. This should be considered when treating malignant neoplasia, where margins can be considered positive if the distance from the tumor is less than 1 mm or a close margin when it is comprised between 1 and 5 mm at the final pathology report.31,32 In addition, the pathologist has to consider the data in the artifact area, which is approximately 1 mm in the electrocautery group. From a clinical point of view, this could lead to making the wrong decision in terms of under- or overtreatment when considering a close margin after surgery. A patient with a close margin after electrocautery should be considered in a different manner from patients treated with harmonic shears. For example; a close margin using harmonic shears could have fewer errors in comparison with a close margin of monopolar electrosurgery. In this circumstance, repeated surgery or complementary radiotherapy would be considered. These data may be correlated with this surgical technique given that when using the harmonic shears, the tissue is held in place between the branches of the instrument with a more uniform excision. In contrast, monopolar dissection seems to cause a wider artifact area due to the contraction of intrinsic muscles of the tongue stimulated by the electrocautery and to the natural movement of the hand of the surgeon.
Harmonic shears are preferable in terms of thermal injury due to the lower cautery crush artifacts.33,34 These data can be explained by the lower temperature of the instrument.
Blood count was significantly (P = .02) different between the 2 groups and is correlated with better hemostasis regarding the water part of the tissue. In addition, red clots are denaturized with a mild increase in temperature and mix with intracellular and interstitial fluids to form a gluelike substance (a coagulum).23,35
Patients with tumors less aggressively treated or who had a mandibulotomy approach were excluded from the study to avoid the risk of bias related to different techniques. We adopted the elements reported in the grading system by Kirakala et al, 11 who referred to the results obtained in the rat model. Our data are related to the clinical practice. Differences between humans and animals or inanimate models can be expected due to different hemostasis patterns, inflammation, and reaction to the tumor.
The use of harmonic instruments in other anatomic sites has already been reported in the literature; for example, in endoscopic surgery, time sparing and blood loss have been already documented, but no mention of the margin artifacts was reported.36-38
Histological data using Harmonic Focus Curved Shears and monopolar electrocautery showed important differences in terms of artifact depth and blood count at surgical margins. This is the first study that has analyzed, in clinical practice, this particular histological aspect using harmonic shears for hemiglossectomy. Monopolar surgery gives a deeper artifact area and less hemostatic effects compared with the harmonic scalpel. The first parameter should be considered in the evaluation of margins, and the second parameter should be respected in intraoperative and postoperative bleeding. Further studies should evaluate the relation between cautery crush formation and clinical healing and postoperative pain after surgery of the tongue, including additional investigation on local recurrence and survival, pain, speech, swallowing, and quality of life. A randomized study with same objectives and a larger recruitment of patients will take place in the future.
Conclusions
When used to perform a partial glossectomy, Harmonic Focus Curved Shears produce less cautery/crush artifact, fewer extravascular blood clots, and a smaller artifact depth compared with monopolar cautery.
Author Contributions
Disclosures
Footnotes
Acknowledgements
The authors acknowledge Ms Tania Merlino for her spelling corrections and grammatical suggestions.
No sponsorships or competing interests have been disclosed for this article.