
Abstract

Pneumolabyrinth is a condition in which the vestibule and/or cochlea is filled with air. 1 Eustachian tube insufflation (ETI) is a type of treatment for recurrent serous otitis media that is still popular in Europe. It exploits the anti-inflammatory and mucolytic effects of thermal waters containing sulfur and bromo-iodine gas.
To our knowledge, no case of a pneumolabyrinth due to barotrauma provoked by ETI has been described previously. The aim of this article is to present a patient who developed a pneumolabyrinth following ETI.
Case Report
A 55-year-old woman was referred to our hospital complaining of vertigo and profound hearing loss in the left ear. One month before, she had undergone ETI because she had recurrent otitis media with effusion (OME). Immediately after the first insufflation, she developed vertigo, hearing loss, and tinnitus. Ten years earlier, she had a successful operation for left stapedotomy. Since then, she has denied symptoms or signs of perilymph fistula (PLF) as attacks of vertigo or hearing impairment.
Otoscopy was normal bilaterally. Pure-tone audiometry revealed profound hearing loss in the left ear, and type A tympanograms were bilaterally observed. No spontaneous nystagmus was detected. Caloric test, vestibular-evoked myogenic potentials (ocular-VEMPs; cervical-VEMPs), and video head impulse test (vHIT) revealed a complete left areflexia. High-resolution computed tomography (HRCT) of the temporal bone revealed pneumolabyrinth ( Figure 1 ). An exploratory tympanotomy showed fibrous tissue around the prosthesis with a small hole creating a communication between the middle ear and the scala vestibule. The oval window was sealed with fat and reinforced with perichondrium. Notwithstanding this, the symptoms did not improve and, 3 weeks postoperatively, HRCT showed the persistence of air in the inner ear. Another exploratory tympanotomy failed to heal the pneumolabyrinth. Thus, it was decided to perform a subtotal petrosectomy with blind sac closure of the external auditory canal (EAC) and obliteration of the eustachian tube. Finally, the middle ear and mastoid were obliterated with abdominal fat.
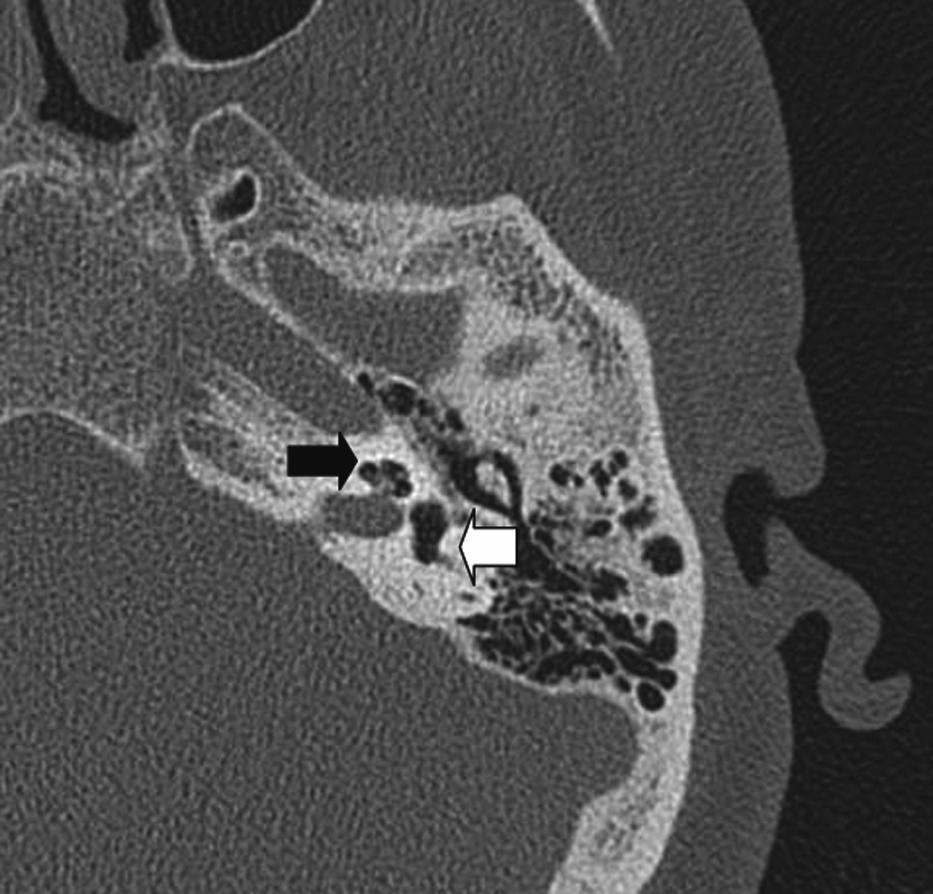
Preoperative high-resolution computed tomography scan: air inside the cochlea (black arrow) and in the vestibule (white arrow).
Vestibular symptoms improved the day after this surgical procedure and had disappeared at 1 month. At this time, profound hearing loss persisted, and vHIT and VEMPs still revealed left areflexia. 2 The HRCT scan performed postoperatively at 2 ( Figure 2 ) and 6 months showed no signs of pneumolabyrinth. The institutional review board of Sapienza University approved the study.
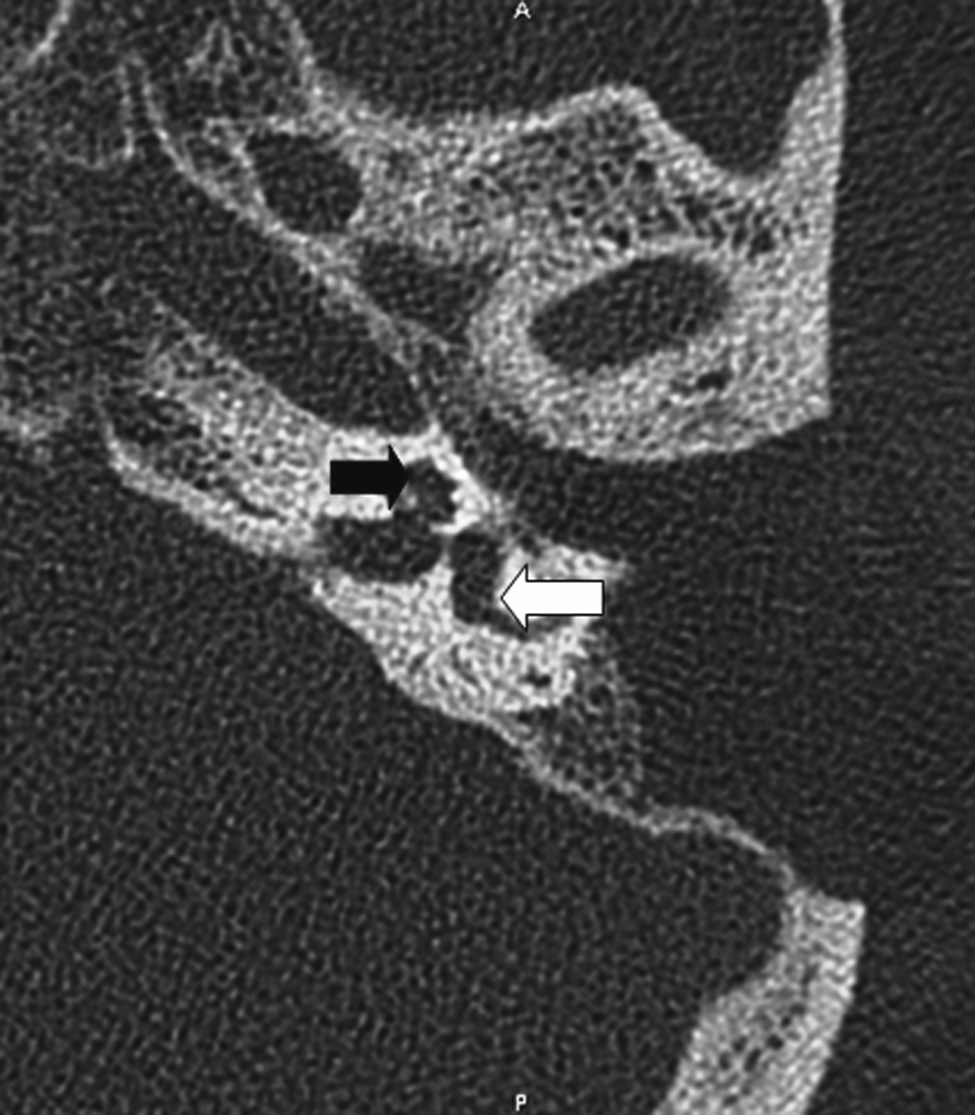
Postoperative high-resolution computed tomography scan: no air into the anterior (black arrow) and posterior (white arrow) labyrinth.
Discussion
Pneumolabyrinth is a rare clinical manifestation of PLF resulting from temporal bone fractures, traumatic stapes dislocation, stapedectomy, cochlear implantation, barotrauma, chronic ear disease, and neoplasms of the middle ear.3-5
In our case, the pathogenesis of pneumolabyrinth may be reasonably linked to the PLF resulting from ETI in the presence of a poststapedotomy fistula with air trapped through a one-way valve mechanism. Eustachian tube insufflation is a type of treatment for recurrent OME that uses the anti-inflammatory and mucolytic effects of thermal waters containing sulfur and bromo-iodine gas. It consists of conveying the gas with a pressure of 0.5 atm for 2 minutes with a gas temperature of 37.5°C into the middle ear by introducing a small probe, the “Itard catheter,” into the patient’s nose until reaching the pharyngeal ostium of the eustachian tube. Although this procedure is considered safe, some cases of pneumocephalus caused by ETI have been reported. 4 To our knowledge, this is the first report of a pneumolabyrinth following this procedure.
There is no definite management strategy for pneumolabyrinth. 5 The surgical option should not be postponed to increase the chances of successful hearing. In our case, because of the persistence of the pneumolabyrinth after 2 subsequent procedures, we preferred performing a subtotal petrosectomy instead of plugging the eustachian tube with insertion of a pressure equalization tube to increase the chance of successful outcome.
A thorough history and physical examination are necessary prior to considering ETI for recurrent OME. Because of the risk of perilymph leakage and pneumolabyrinth, providers should exercise caution when recommending this treatment option or other particular processes of cannulation of the eustachian tube for patients with a history of stapes surgery. Although Mandalà et al 3 also reported a poststapedectomy pneumolabyrinth from barotrauma secondary to rapid altitude changes in the ear, our one case report obviously does not justify advising every single stapes patient not to “pop their ears” on a plane or in the mountains. This dramatic pronouncement would unnecessarily label stapes surgery as potentially unsafe.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.