
Abstract
Objective
This study aimed to investigate whether adding low-molecular-weight dextran to oral steroids in patients with idiopathic sudden sensorineural hearing loss resulted in better hearing outcomes than those in patients receiving oral corticosteroids alone.
Study Design
Historical cohort study.
Setting
Tertiary teaching hospital.
Subjects and Methods
The authors reviewed the clinical records of 166 patients with idiopathic sudden sensorineural hearing loss. Therapeutic effectiveness was measured by the gain of pure-tone averages and 4 categories of hearing outcome (complete recovery, marked recovery, mild improvement, or no improvement). To manage potential confounding factors associated with treatment allocation, the authors matched the subjects from each group according to the propensity score (ie, the predicted probability that they would receive a specific treatment).
Results
The authors identified 50 pairs of propensity score–matched subjects (n = 100) without significant difference of all clinical factors (P > .05). Subsequent analyses demonstrated that the average hearing gain in subjects receiving additional dextran to oral steroid was 31.7 ± 21.5 dB, which did not differ from 33.0 ± 21.8 dB in subjects receiving steroids alone (P = .76). Difference of hearing outcomes between the 2 groups was also nonsignificant (P = .92).
Conclusion
Matching propensity scores successfully balanced the heterogeneity between the dextran and steroid groups. Analytical results demonstrated that adding low-molecular-weight dextran to oral corticosteroids was not associated with greater hearing gain or better hearing outcome in idiopathic sudden sensorineural hearing loss.
Idiopathic sudden sensorineural hearing loss (ISSHL) is defined as sudden-onset hearing deterioration of at least 30 dB for at least 3 contiguous frequencies that develops within 72 hours. 1 Although most cases are regarded as “idiopathic,” 2 several theories have been proposed to explain the pathophysiology of ISSHL, including vascular compromise, viral infection, intratympanic membrane rupture, and autoimmune disease.3-6
Reflecting the multiple potential etiologies, ISSHL treatment is diverse and the “standard” regimen is lacking. For example, vasodilators, rheologic/vasoactive agents, anti-inflammatory agents, and antiviral agents have all been investigated in the management of ISSHL,7-10 either as monotherapy or as combinations of several medications, known as the “shotgun” regimen. 11 Although the mechanisms and the clinical effectiveness are not fully clear, 12 corticosteroids are, by far, the most frequently recommended treatment in ISSHL. 13 In addition to steroids, low-molecular-weight dextran is another common therapy that may improve microcirculation in the cochlea.14-16 However, dextran has been associated with several potentially serious adverse effects, such as pulmonary edema, oliguric renal failure, and coagulopathy.17-19 Furthermore, intravenous administration of dextran requires the inconvenience of hospitalization and increases medical expenses.
Propensity scores, which represent the probability of assignment to a particular treatment option based on the observed covariates, 20 have been widely used to compare the effectiveness and associated risks of medical interventions.21,22 For observational studies, matching the propensity scores may result in an unbiased comparison between treatment options, approximating the strength of randomized studies. 23 Several otolaryngological studies have applied propensity scores to compare survival outcomes and treatment effectiveness.24,25
Although dextran is commonly prescribed in the management of ISSHL, the effectiveness of dextran has never been demonstrated in the literature.26-28 Therefore, we conducted this propensity score–matched study to evaluate whether corticosteroid-treated ISSHL patients receiving additional dextran therapy demonstrated better hearing outcome than patients receiving corticosteroids alone.
Methods
Study Subjects
Clinical records were retrospectively reviewed in subjects with unilateral ISSHL visiting a tertiary teaching hospital. Both air and bone conduction hearing thresholds were performed (MA-53 audiometer; MAICO, Berlin, Germany), and subjects with the presence of air-bone gaps were excluded from the study. Other exclusion criteria included age younger than 18 years, preexisting hearing loss, history of otitis media, or previous ear surgery. 29 The mean hearing level was calculated by averaging 4-tone thresholds (ie, 500, 1000, 2000, and 3000 Hz). 30 Recorded information included delay in the treatment, age, sex, presence of vertigo, and history of diabetes mellitus (DM), hypertension, and cardiovascular disease. Since patients with a delay in treatment for more than 14 days did not receive routine therapy in our department, we also excluded such patients from this study. 29 This study was approved by the institutional review board of Far Eastern Memorial Hospital.
Treatment Protocols
Each patient received oral prednisolone (1 mg/kg/d) that was administered for 7 consecutive days and gradually tapered over another 7-day course. For the subjects who received additional dextran therapy, intravenous low-molecular-weight dextran (500 mL administered by an intravenous drip for more than 4 hours, twice a day) was prescribed for 7 consecutive days. Repeated pure-tone audiometry was carried out every other day during admission. Outpatient follow-up and a series of audiometric examinations were performed monthly for at least 3 months unless complete hearing recovery was documented. The gain of pure-tone average was calculated by subtracting the final hearing level (HL) from the initial hearing level (dB). Hearing outcome was classified into 4 categories: complete recovery (hearing improvement >30 dB HL and side difference ≤10 dB HL), marked recovery (hearing improvement >30 dB), mild improvement (10 dB < hearing improvement ≤ 30 dB), and no improvement (hearing improvement ≤10 dB). 31
Statistical Analysis
Demographic data and clinical information between the 2 groups were compared using the Student t test, χ2 test, or Fisher’s exact test. To eliminate bias due to the uneven distribution of the confounding factors, we matched subjects between the dextran and steroid groups using the propensity score. 32 First, we conducted a multiple logistic regression model to determine the likelihood of receiving dextran therapy (ie, the propensity score, ranging from 0-1), as a function of confounding factors, including age, sex, pretreatment hearing levels, delay in treatment, vertigo, DM, hypertension, and cardiovascular disease. In the second step, each subject from the steroid group was matched to 1 subject from the dextran group, using the nearest neighbor matching method. The difference of the propensity score between each matched pair should be less than 0.02. Subjects without a match were dropped.
Subsequent evaluation of the treatment outcomes was conducted among the propensity score–matched subjects from the dextran and the steroid groups. We applied the Student t test and the Cochrane-Armitage trend test to compare the gain of pure-tone average and the 4 categories of hearing outcome, respectively. A P value of less than .05 was considered significant.
Results
This study recruited 166 ISSHL patients, including 91 men and 75 women, with a mean (SD) age of 50.4 (13.9) years. Table 1 illustrates the demographic data and clinical information of the patients in the dextran and steroid groups. Although age and sex distributions demonstrated no significant differences between the 2 groups (P > .05), the pretreatment hearing threshold in the dextran group was significantly higher than that in the steroid group (90.8 vs 83.6 dB, P < .01, Student t test). In patients receiving dextran therapy, the average treatment delay was 2.9 ± 2.4 days, compared with 5.4 ± 4.0 days in subjects receiving steroids only, which also demonstrated a significant difference ( Table 1 , P < .01, Student t test). Otherwise, the occurrence of vertigo, DM, hypertension, and cardiovascular disease did not differ significantly between the 2 groups (P > .05, χ2 test and Fisher’s exact test). Among the 166 ISSHL patients, both hearing gain of pure-tone averages and 4 categories of hearing outcome demonstrated nonsignificant differences between the steroid and dextran groups ( Table 2 , P > .05).
Demographic Data and Clinical Information of 166 ISSHL Patients in the Dextran and Steroid Groups
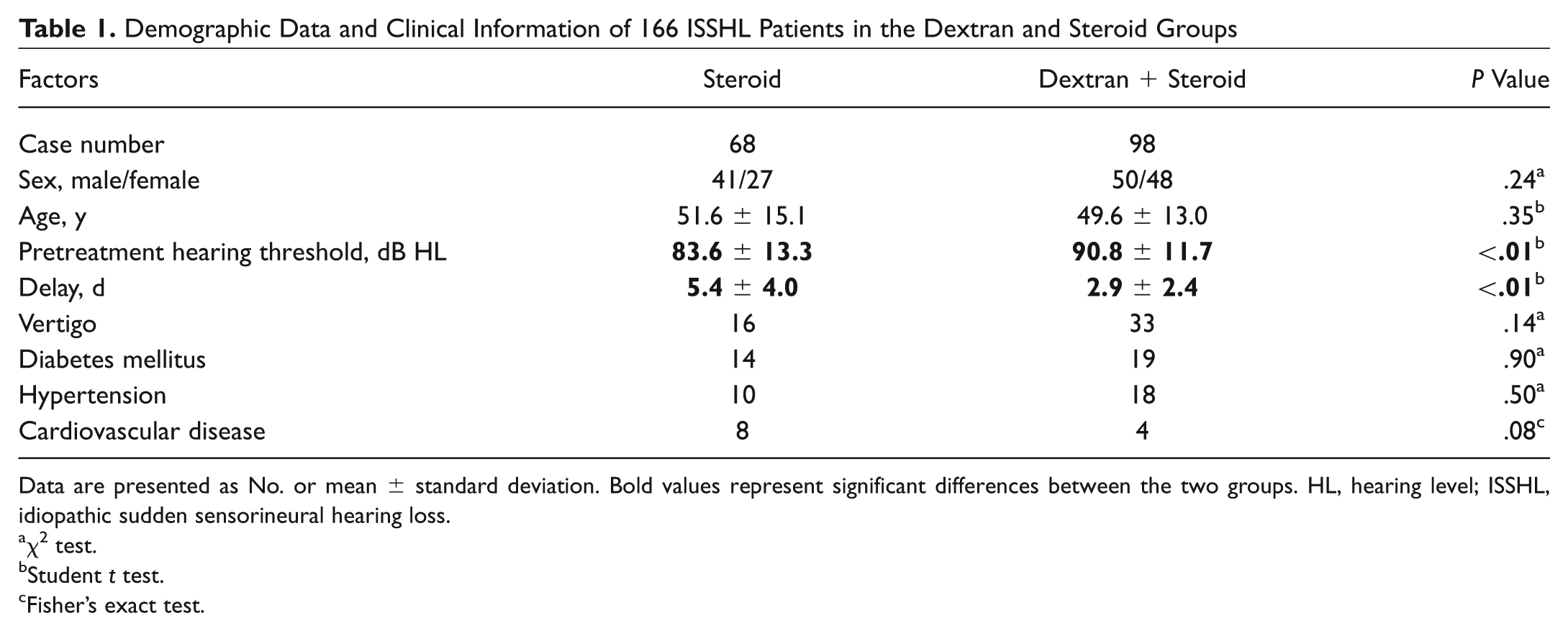
Data are presented as No. or mean ± standard deviation. Bold values represent significant differences between the two groups. HL, hearing level; ISSHL, idiopathic sudden sensorineural hearing loss.
χ2 test.
Student t test.
Fisher’s exact test.
Treatment Outcome between the Dextran and Steroid Groups in the 166 ISSHL Patients
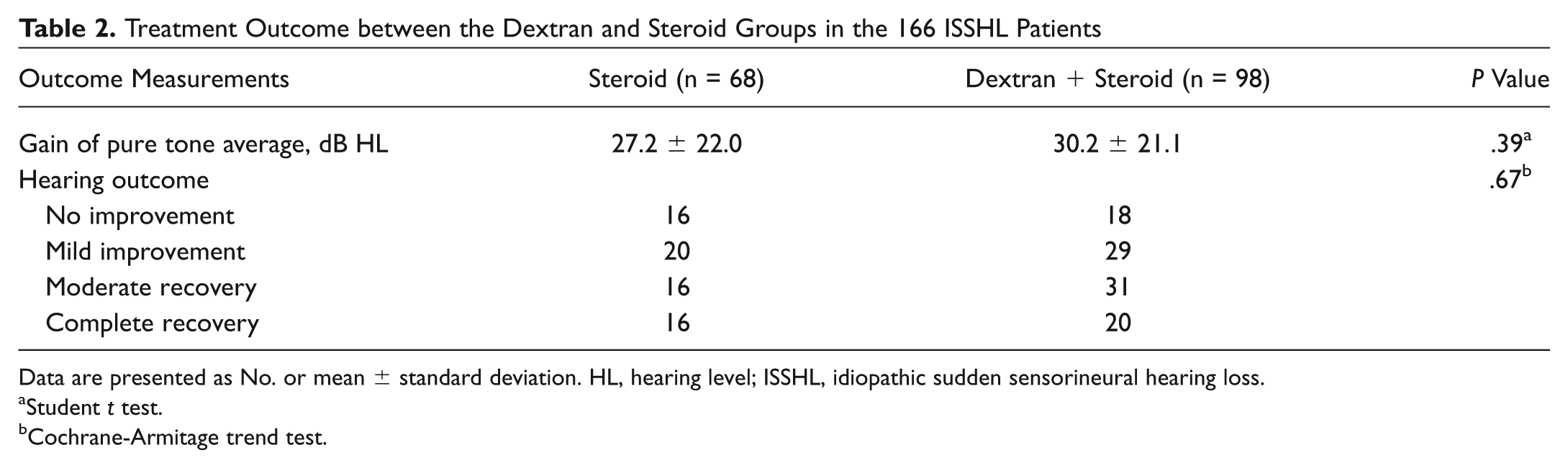
Data are presented as No. or mean ± standard deviation. HL, hearing level; ISSHL, idiopathic sudden sensorineural hearing loss.
Student t test.
Cochrane-Armitage trend test.
To manage the unbalanced clinical data between the steroid and dextran groups, we matched subjects from the 2 groups according to the propensity scores. As a result, 50 pairs of propensity score–matched subjects were identified (n = 100) and the potential confounders did not differ significantly between the 2 groups ( Table 3 , P > .05).
Demographic Data and Clinical Information of the 100 Propensity Score–Matched ISSHL Patients
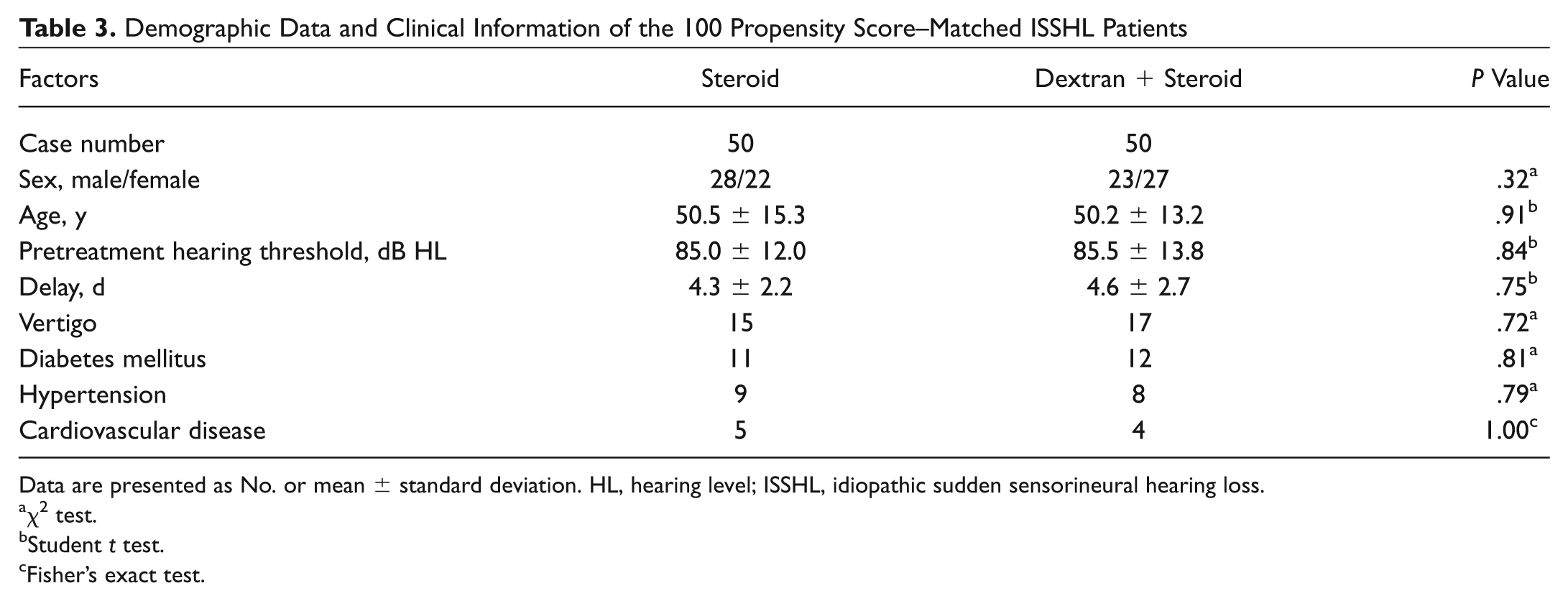
Data are presented as No. or mean ± standard deviation. HL, hearing level; ISSHL, idiopathic sudden sensorineural hearing loss.
χ2 test.
Student t test.
Fisher’s exact test.
Among the 100 propensity score–matched patients, we compared the treatment outcome by the gain of pure-tone averages (dB HL) and 4 categories of hearing improvement. The average hearing gain in subjects receiving dextran therapy in addition to corticosteroids was 31.7 ± 21.5 dB, which did not differ from 33.0 ± 21.8 dB, the value found in the subjects receiving steroids only ( Table 4 , Student t test, P = .76). Similarly, comparison of hearing improvement by 4 categories failed to demonstrate significant differences between the 2 groups ( Table 4 , Cochrane-Armitage trend test, P = .92).
Treatment Outcome between the Dextran and Steroid Groups in the 100 Propensity Score–Matched ISSHL Patients
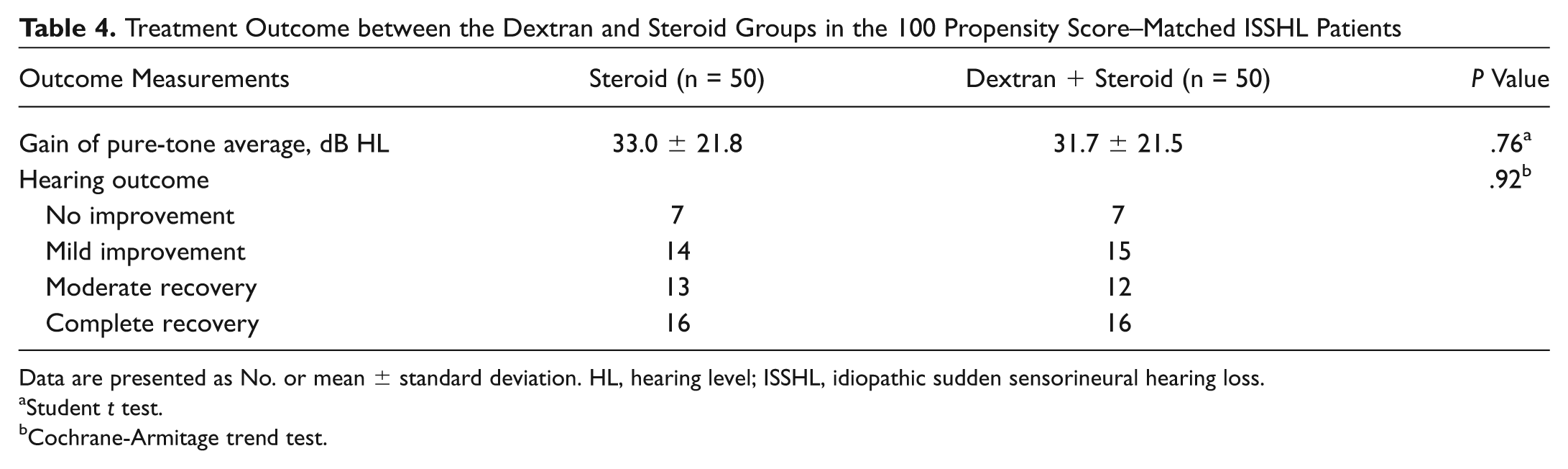
Data are presented as No. or mean ± standard deviation. HL, hearing level; ISSHL, idiopathic sudden sensorineural hearing loss.
Student t test.
Cochrane-Armitage trend test.
In the 98 patients receiving low-molecular-weight dextran therapy in this series, only 1 patient experienced an adverse effect of treatment (1%). This complication was an instance of acute oliguric renal failure. The 68-year-old woman, who had DM controlled by oral hypoglycemic agents, suffered from the sudden onset of hearing loss, vertigo, and tinnitus. She visited our clinic 2 days later, and pure-tone audiometry revealed total deafness on the right side. Under the diagnosis of ISSHL, she was admitted for oral steroids and intravenous dextran therapy. Unfortunately, oliguria developed after 7 days of dextran infusion, and the serum creatinine level increased to 9.6 mg/dL. After 2 courses of emergent hemodialysis, the urine output gradually recovered and the serum creatinine level decreased to 2.2 mg/dL, at which time the patient was discharged from the hospital. Final audiometry 3 months later showed mild hearing improvement with a pure-tone threshold of 88 dB.
Discussion
Idiopathic sudden sensorineural hearing loss is one of the most frequently encountered otologic emergencies, with an annual incidence rate ranging from 5 to 20 cases per 100,000 persons. 33 Conceptually, the management of ISSHL should target the postulated disease mechanism. For example, corticosteroids have been shown to reduce the neuronal edema caused by ischemic injury, postviral infection, or autoimmune processes. 34 In addition, vasoactive agents, such as low-molecular-weight dextran, are prescribed by some providers as an adjuvant of steroid therapy to improve microcirculation in the cochlea by hemodilution and volume expansion. 35 Despite the pathophysiological support of applying vasoactive agents in the management of ISSHL, the evidence from the existing literature is controversial. 36 Besides, since the administration of low-molecular-weight dextran is associated with potential life-threatening adverse effects, it is obligatory to investigate whether additional dextran therapy to oral corticosteroids will be associated with a better treatment outcome.
The major strength of this study is the identification of 2 homogeneous and comparable groups, by matching the propensity score between patients receiving steroid alone and those receiving oral steroid with additional dextran therapy ( Tables 1 and 3 ). Since the propensity score represents the conditional probability of receiving specific treatment based on the patient’s baseline characteristics, matching the propensity scores ensures a similar distribution of the characteristics between the 2 treatment options. 37 Based on literature reports and the presenting research, propensity scores appear to be a valuable tool for controlling potential bias and enhancing result quality of observational studies.
This study demonstrated that dextran therapy in addition to oral steroids was not associated with greater hearing gains (dB) or better hearing outcomes than those receiving oral steroids alone ( Table 4 ). Effective elimination of selection bias by matching the propensity scores between the 2 treatment groups has increased the reliability and the validity of our results. Considering the life-threatening adverse effects of dextran, the lack of a positive effect on hearing improvement from the current study, and the paucity of the existing supportive literature, we suggest this high-risk treatment for ISSHL should be abandoned.
This study possesses several limitations. First, despite our considerable efforts to correct for multiple confounders, unknown ISSHL prognostic factors may still exist. Therefore, we cannot fully eliminate the possibility of subtle differences between the matched subjects in the dextran and steroid groups. We acknowledge that a well-conducted randomized controlled trial remains the best solution to solve this problem. Based on the literature, a change of less than 10 dB in pure-tone average may not be clinically differentiable. 29 Accordingly, post hoc analysis in this propensity score–matched cohort study demonstrated that a sample size of 100 has 95% power to discriminate a difference larger than 10 dB between the 2 groups (2-sided α level: 0.05; G*power software, version 3.1.3, University of Düsseldorf, Düsseldorf, Germany). 38 Therefore, before the definite answer is obtained by large-scale clinical trials, our results remain a useful reference for clinicians in daily practice. Second, although speech discrimination score is a meaningful parameter of reporting hearing outcome, we are not able to provide a comprehensive analysis based on the obtainable records of speech testing. Finally, the extent of hearing loss in our study population was quite profound, which may be explained by the fact that severe cases are more likely to be referred to teaching hospitals than those with mild initial hearing loss. In addition, only adult patients were recruited in this series. Consequently, our results may not be applicable to patients with a lesser extent of ISSHL and patients younger than 18 years. Further studies are required to determine the effectiveness of dextran in milder forms of ISSHL and in pediatric/adolescent patients.
Author Contributions
Disclosures
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
This article will be presented as a poster at the 2012 AAO-HNSF Annual Meeting and OTO EXPO; September 9-12, 2012; Washington, DC.