
Abstract
Objective
To develop a consensus statement on the appropriate use of computed tomography (CT) for paranasal sinus disease.
Subjects and Methods
A modified Delphi method was used to refine expert opinion and reach consensus by the panel.
Results
After 3 full Delphi rounds, 33 items reached consensus and 16 statements were dropped because of not reaching consensus or redundancy. The statements that reached consensus were grouped into 4 categories: pediatric sinusitis, medical management, surgical planning, and complication of sinusitis or sinonasal tumor. The panel unanimously agreed with 13 of the 33 statements. In addition, at least 75% of the panel strongly agreed with 14 of 33 statements across all of the categories.
Conclusions
For children, careful consideration should be taken when performing CT imaging but is needed in the setting of treatment failures and complications, either of the pathological process itself or as a result of iatrogenic (surgical) complications. For adults, imaging is necessary in surgical planning, for treatment of medical and surgical complications, and in all aspects of the complete management of patients with sinonasal and skull base pathology.
Computed tomography (CT) is an essential diagnostic tool that has become an integral part of the diagnostic paradigm for patients with clinical conditions involving the paranasal sinuses and skull base. Computed tomography imaging has facilitated the diagnosis of various pathologic entities (eg, benign, malignant, inflammatory, traumatic) causing sinonasal disease and is routinely used in contemporary management of patients in a variety of clinical settings, including point-of-service (POS) care. In addition to obtaining an accurate diagnosis, paranasal sinus CT imaging is critically important for preoperative surgical planning and avoidance of surgical complications. Moreover, advances in CT technology have improved the speed and safety of image acquisition while producing high-quality images.
Computed tomography imaging, however, may also be associated with significant costs, excessive radiation exposure that may lead to increased cancer risk, and overuse concerns. Radiation exposure is much greater with imaging modalities such as multiphase studies; abdomen, pelvis, and chest CT imaging; interventional radiology procedures; and nuclear medicine studies compared with standard sinus and skull base CT imaging (conventional and cone beam CT [CBCT]).
Overall, the average per capita exposure to ionizing radiation from imaging examinations increased by nearly 600% from 1980 to 2006 in the United States. 1 Reports have indicated that cumulative exposure to radiation over time increases the risk of adverse health outcomes, and the result of cumulative exposure causes a corresponding increase in the incidence of malignancies most associated with medical radiation exposure, such as leukemia, breast and thyroid malignancy, and possibly cardiovascular disease in exposed patient populations.2,3 Overall, the literature suggests that up to 2% of cancers in the United States could be attributable to radiation exposure associated with CT imaging.4,5
As of 2006, diagnostic imaging costs were among the fastest growing Medicare expenses. 6 In 2006, it was estimated that more than 62 million scans were performed, as compared with about 3 million in 1980, including at least 4 million for children. 4 Although CT utilization has increased significantly over the past several years, a recent report from the Access to Medical Imaging Coalition indicates that the volume of advanced imaging services provided to Medicare beneficiaries decreased in 2009, representing the first decrease in 11 years. 7 The study showed that the volume of advanced imaging services billed in 2009 decreased by 0.1% compared with 2008, whereas overall imaging services declined by 7.1% for the same year-to-year comparison.
Because of rising concerns of safety, cost, and potential overuse with CT imaging for patients with paranasal sinus disease, the need for consensus-based guidance has become more evident. Currently, there is a lack of literature that provides guidance on appropriate indications for CT imaging in this population.
To help organize and disseminate information on appropriate use of CT for paranasal sinus disease, this consensus panel was convened by the American Academy of Otolaryngology–Head and Neck Surgery (AAO-HNS) to create a clinical consensus statement. This document reflects information synthesized from an organized group of expert opinions in a written document with the purpose of reviewing the literature, synthesizing information, and attempting to clarify areas of controversy or ambiguity. The findings of this consensus panel are stated as opinions or suggestions and not as guidelines.
Methods
The development of this consensus statement consisted of panel recruitment, determination of clinical/evidence gaps through a literature review, survey development and administration, revision of ambiguous survey questions, resurvey (if warranted), data aggregation, and analysis.
Panel Recruitment and Literature Review
The 12 panel members represented the multidisciplinary fields of radiology, pediatric otolaryngology, otolaryngology–head and neck surgery, otolaryngic allergy, facial plastics and reconstructive surgery, rhinology, skull base surgery, and periodontology. The panel chair (G.S.) led the survey and manuscript development along with designated panel members and a staff liaison.
Clinical gaps in the literature were sought through existing guidelines or evidence reviews such as the AAO-HNS Adult Sinusitis Guideline 8 and American College of Radiology (ACR) Appropriateness Criteria. 9 The Appropriateness Criteria are evidence-based guidelines that assist referring physicians and other providers in making the most appropriate imaging or treatment decision for a specific clinical condition. By employing these guidelines, providers enhance quality of care and contribute to the most efficacious use of radiology. The guidelines were developed by experts with knowledge in diagnostic imaging, interventional radiology, radiation oncology, and other relevant specialties. Recommendations are based on the available medical literature to the extent possible supplemented by expert opinion. The expert panel for the ACR Appropriateness Criteria guidelines for sinonasal disease imaging included neuroradiologists, neurologists, and otolaryngologist–head and neck surgeons. The AAO-HNS Adult Sinusitis Guideline and ACR Appropriateness Criteria were used as resource material for this consensus statement; however, there was no official participation of the ACR in the preparation of this document.
A supplemental systematic search that included systematic reviews (including meta-analyses) or clinical practice guidelines in English from PubMed and The Cochrane Library from 2007 to 2011 using the search string “Tomography, X-Ray Computed[mh] AND paranasal sinus disease[mh]” was also included. The gaps in literature were used as a framework for the qualitative and Delphi surveys.
The Delphi Method: Survey Development and Administration
The Delphi method, 10 a technique designed to refine expert opinion through survey, was used to obtain consensus. The method used multiple confidential survey iterations to seek equal input from each panel member and attempted to reduce undue influence from a minority of participants. This rigorous and standardized approach minimizes bias and facilitates expert consensus.
Web-based software (Survey Monkey, Menlo Park, California) was used to survey the panel. The survey period was broken down into 4 iterations: 1 qualitative survey with free text boxes for responses and 3 subsequent Delphi rounds. All answers were de-identified and remained confidential; however, e-mail addresses were collected to ensure proper follow-up, if needed. The qualitative survey included 8 questions on the indications, contraindications, advantages, and disadvantages of CT scans of the sinus and the role a CT scan played at various points of care. The purpose of the qualitative survey was to narrow the scope and provide a framework for subsequent Delphi rounds.
The 3 Delphi round surveys were broken down into 4 clinical areas: (1) pediatric sinusitis, (2) medical management, (3) surgical planning, and (4) complications of sinusitis or sinonasal tumors. Prior to dissemination to the panel, the survey was reviewed by the panel chair (G.S.) and consultant (J.S.R.) for content and clarity. Questions in the survey were answered using a 5-point Likert scale where 1 = strongly disagree, 2 = disagree, 3 = neither agree nor disagree, 4 = agree, and 5 = strongly agree. One round occurred when the survey was distributed; responses were aggregated, distributed back to the panel, discussed via teleconference, and revised, if warranted. The purpose of the teleconference was to provide an opportunity to clarify any ambiguity, propose revisions, or drop any statements recommended by the panel.
Analyses and Interpretation
Likert questions were reported using the median, mode, range, and percentage of agreement (and strong agreement in cases >75%). Consensus was defined as follows:
1: Agree AND strongly agree OR disagree AND strongly disagree and no more than 1 outlier in the opposite direction
2: Agree AND strongly agree OR disagree AND strongly disagree and less than 3 choices selected as neither agree nor disagree
3: No more than 1 panel member skipping the question.
The final statements that reached consensus were aggregated and analyzed.
Results
Overall, of 48 initial statements, 33 reached consensus and 15 were dropped because of redundancy or because the statements did not reach consensus by the panel. Statements that were dropped are shown in Table 1 .
Summary of Dropped Statements (n = 15)
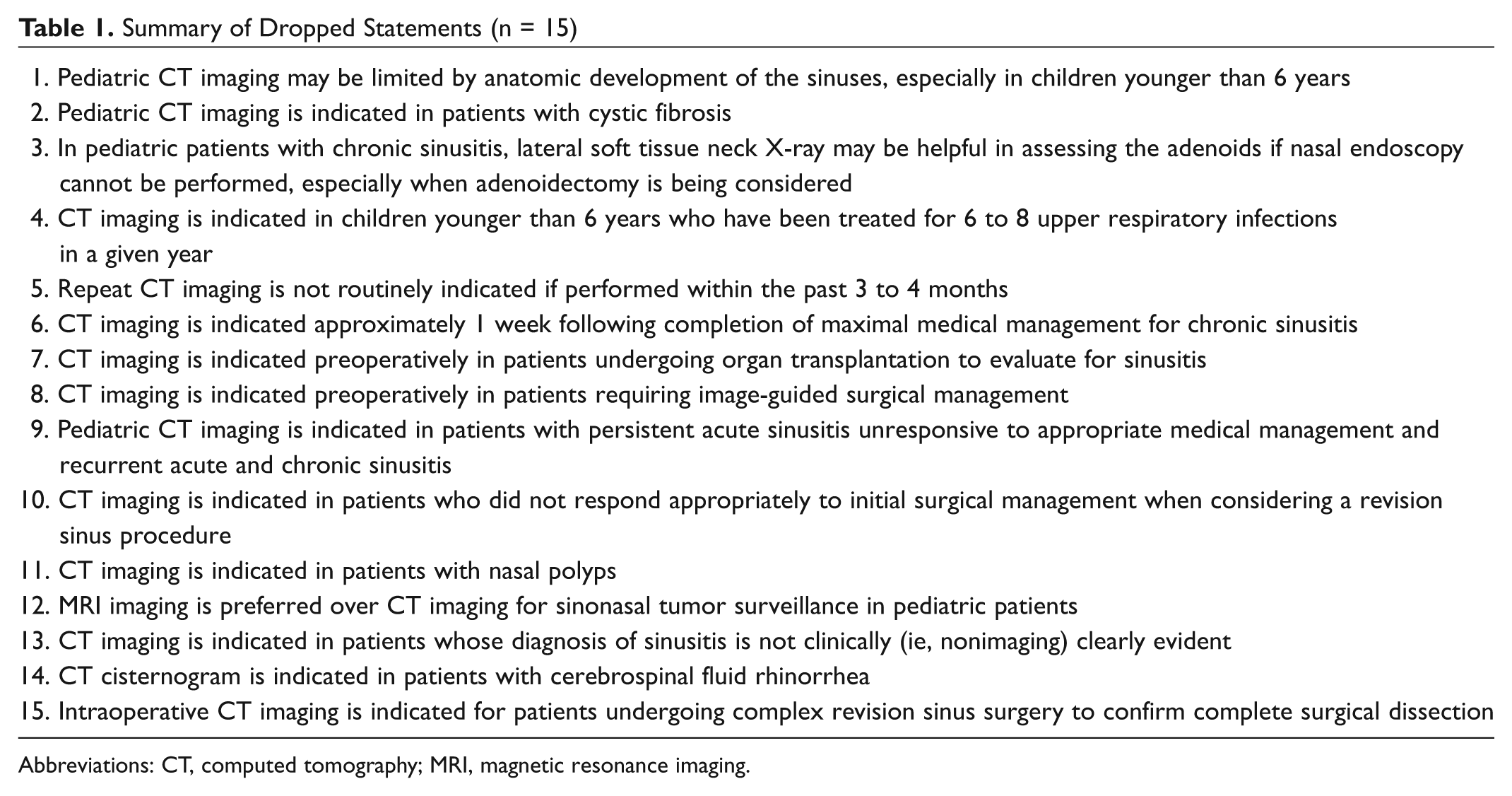
Abbreviations: CT, computed tomography; MRI, magnetic resonance imaging.
Pediatric Sinusitis
For pediatric sinusitis, 7 statements reached consensus ( Table 2 ). Of these, 4 had at least 75% of the panel strongly agree to the statement (statements 1, 4, 6, and 7). The panel agreed that when medical management with or without adenoidectomy has failed to control the symptoms of sinusitis in the pediatric population, CT imaging is indicated (statement 1). In the immunocompromised child with concern for invasive fungal sinusitis, magnetic resonance imaging (MRI) is indicated along with CT imaging (statement 2). There was unanimous agreement that pediatric CT imaging may be limited by radiation safety concerns and possible requirement for sedation, especially in children younger than 6 years (statement 3). There was strong agreement that pediatric CT imaging is indicated at any age for suspected tumor, complications from sinusitis, and prior to sinus surgery (statement 4). For children younger than 3 years, CT imaging is indicated in those with chronic sinusitis who have failed appropriate medical management (statement 5); however, CT imaging is not indicated for acute uncomplicated sinusitis unless they have had prior appropriate medical therapy (statement 6). The panel unanimously agreed that CT imaging for pediatric patients is not indicated for routine uncomplicated upper respiratory infections (such as colds) for a duration of less than 10 days (statement 7).
Pediatric Sinusitis Statements Reaching Consensus (n = 7)
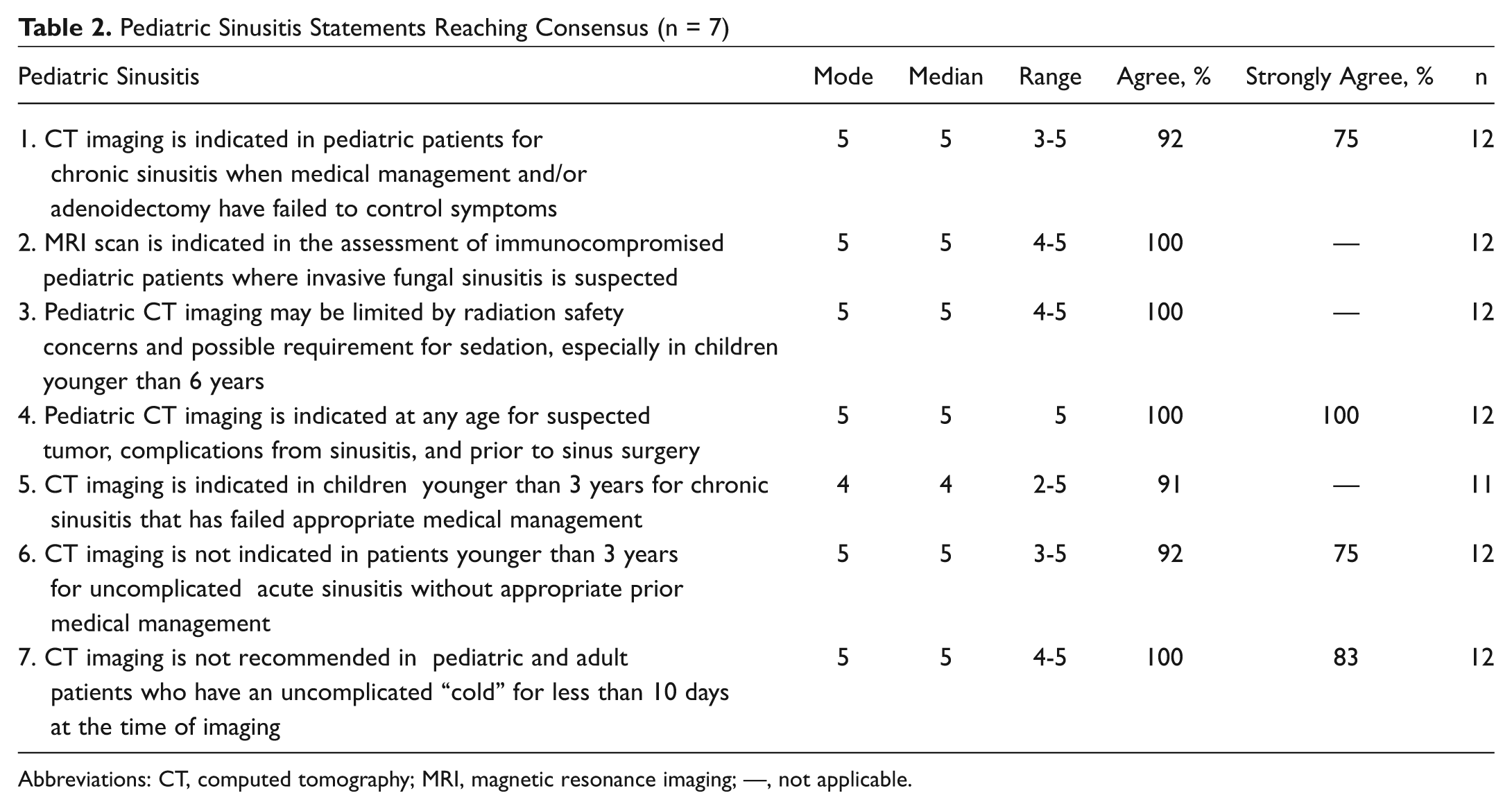
Abbreviations: CT, computed tomography; MRI, magnetic resonance imaging; —, not applicable.
Medical Management
For medical management, 11 statements reached consensus by the panel ( Table 3 ). Of these, 4 statements had at least 75% of the panel strongly agree (statements 3, 5, 8, and 10). The panel reached consensus that CT imaging is indicated in patients not responding appropriately to medical management (statement 1). The panel unanimously agreed that CT imaging is indicated in patients who have been treated repeatedly with antibiotics and other medications for presumed sinusitis, with persistent complaints posttreatment, but no clinical evidence of sinusitis, to confirm that the problem is indeed not due to sinonasal pathology and thereby avoid continued inappropriate antibiotic administration (statement 2). Computed tomography imaging is not indicated for clinically diagnosed uncomplicated acute sinusitis (statement 3); however, it is indicated for recurrent acute and chronic sinusitis (statement 4) and patients with cerebrospinal fluid (CSF) rhinorrhea (suspected or confirmed, spontaneous or iatrogenic). The panel reached consensus that CT imaging in the asymptomatic patient, in conjunction with physical and endoscopic examination, is appropriate in certain circumstances such as tumor surveillance and to monitor areas not well visualized clinically (statement 6). A CT image is indicated for facial pain following dental procedures or for complicated dental infections, or when odontogenic sinusitis is suspected but unproven following dental evaluation (statement 7).
Medical Management Statements Reaching Consensus (n = 11)
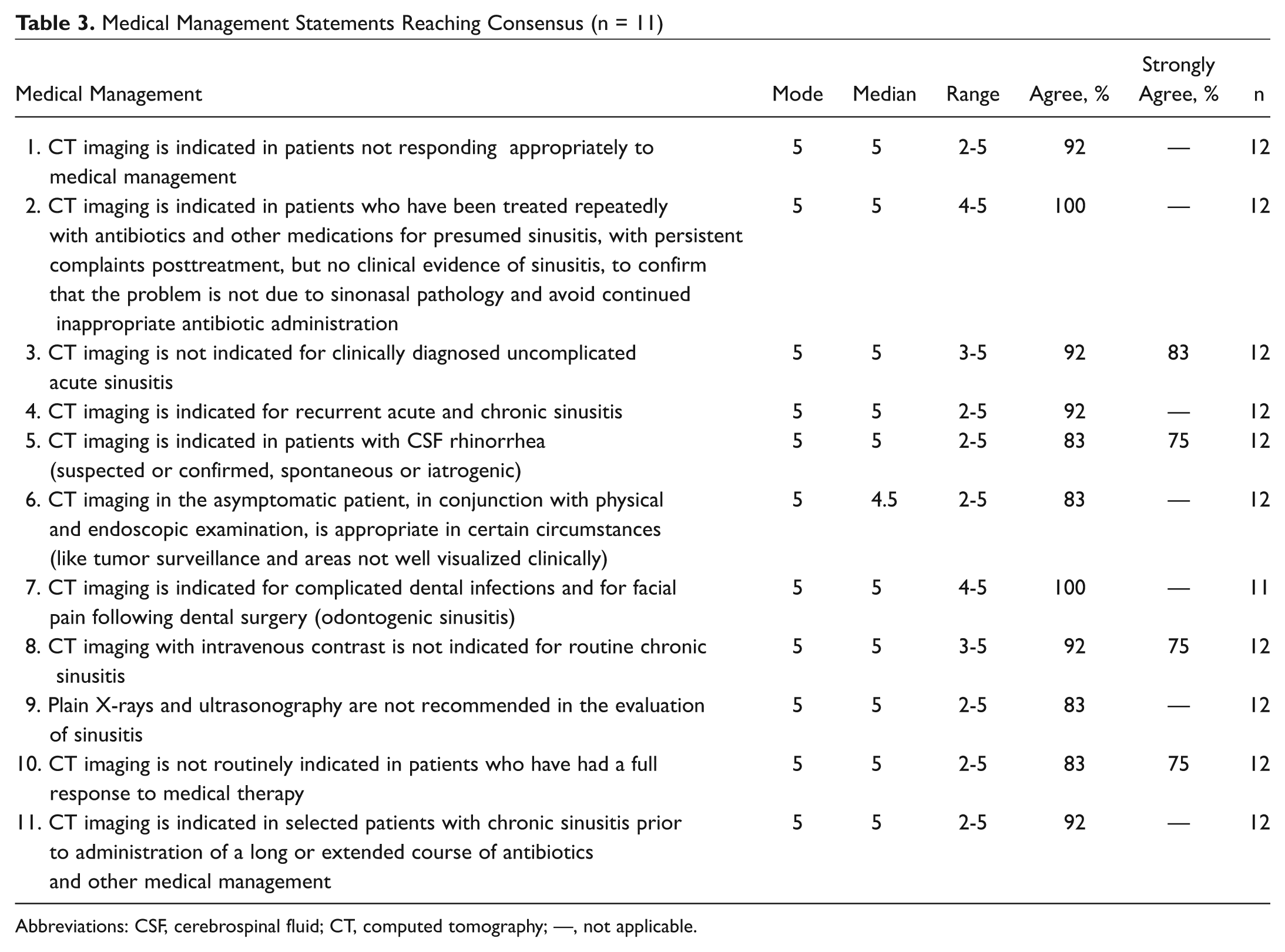
Abbreviations: CSF, cerebrospinal fluid; CT, computed tomography; —, not applicable.
Surgical Planning
For surgical planning, 5 statements reached consensus by the panel ( Table 4 ). Of these, 2 statements had at least 75% of the panel strongly agree (statements 1 and 4). The panel unanimously agreed that CT imaging is indicated prior to sinus surgery (statement 1) and, in the case of malignant disease, may be combined with positron emission tomography (PET) scanning for tumor surveillance and preoperative surgical planning (statement 3). In addition, the panel unanimously agreed that CT imaging is indicated for patients undergoing sinus surgery requiring intraoperative navigation for image-guided surgery (statement 4). The panel reached consensus that CT imaging may be indicated prior to dental implant, “sinus lift,” or other dental surgery involving the teeth of the maxilla. The panel agreed that CBCT imaging for sinonasal disease delivers lower radiation doses than conventional CT imaging (statement 5).
Surgical Planning Statements That Reached Consensus (n = 5)
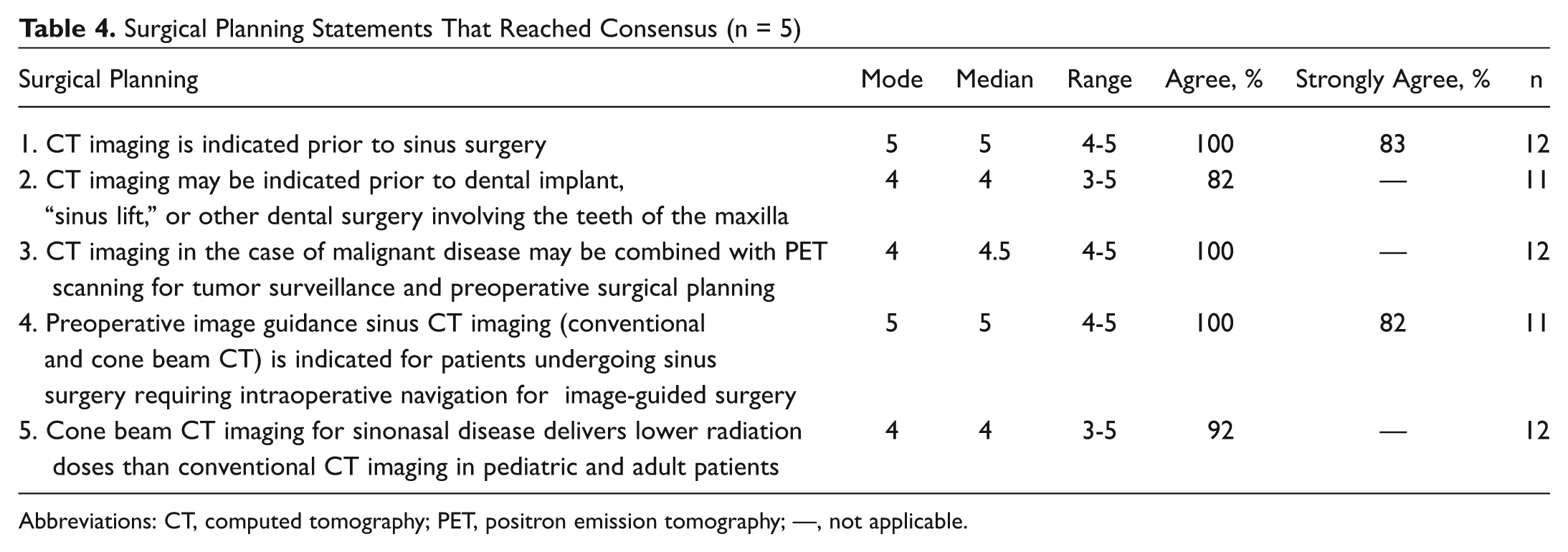
Abbreviations: CT, computed tomography; PET, positron emission tomography; —, not applicable.
Complication of Sinusitis or Sinonasal Tumor
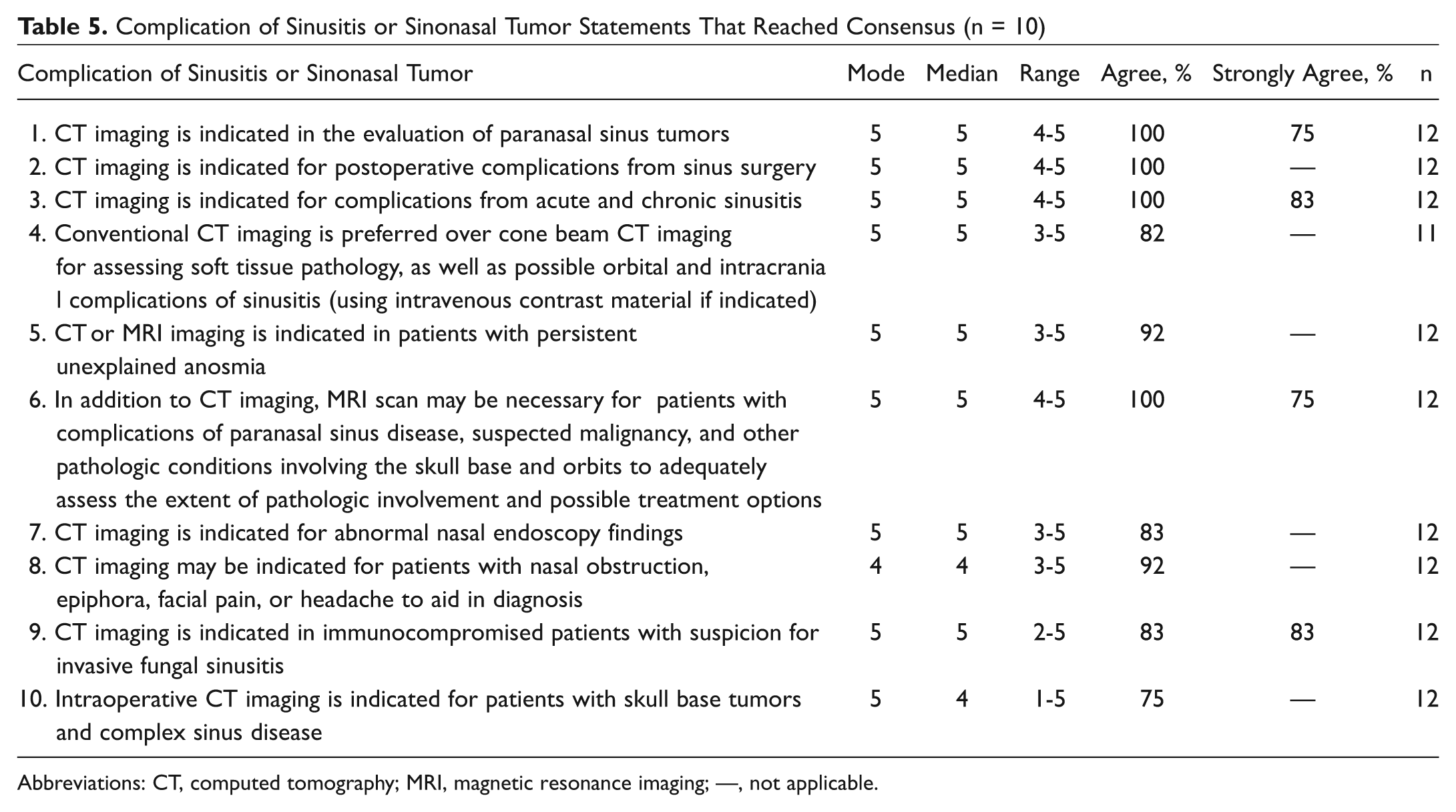
For complications of sinusitis or sinonasal tumors, 10 statements reached consensus by the panel ( Table 5 ). Of these, 4 statements had at least 75% of the panel strongly agree (statements 1, 3, 6, and 9). The panel agreed that CT imaging is indicated in the evaluation of paranasal sinus tumors (statement 1), for postoperative complications from sinus surgery (statement 2), and for complications from acute and chronic sinusitis (statement 3). The panel agreed that conventional CT imaging is preferred over CBCT imaging for assessing soft tissue pathology, as well as possible orbital and intracranial complications of sinusitis using intravenous contrast material if indicated (statement 4). Computed tomography or magnetic resonance imaging is indicated in patients with persistent unexplained anosmia (statement 6). In addition to CT imaging, MRI scan may be necessary for patients with complications of paranasal sinus disease, suspected malignancy, and other pathologic conditions involving the skull base and orbits to adequately assess the extent of pathologic involvement and to determine possible treatment options (statement 7). Computed tomography imaging may be indicated for patients with nasal obstruction, epiphora, facial pain, or headache to aid in diagnosis (statement 8). For immunocompromised patients with suspicion for invasive fungal sinusitis, CT imaging is indicated (statement 9). However, MRI of the brain may also be necessary in this group of patients. Intraoperative CT imaging is indicated for patients with skull base tumors and complex sinus disease (statement 10).
Complication of Sinusitis or Sinonasal Tumor Statements That Reached Consensus (n = 10)
Abbreviations: CT, computed tomography; MRI, magnetic resonance imaging; —, not applicable.
Discussion
Pediatrics
Radiation exposure, especially in the pediatric population, is a growing concern in diagnostic medicine. The increased availability of CT scanners has led to growth in the number of these studies being ordered. The pediatric statements that reached consensus generally emphasized the need to minimize CT scans when possible. Consistent with the ACR Appropriateness Criteria, imaging studies were not indicated for uncomplicated acute sinusitis in pediatric patients. However, the panel clarified further that CT imaging was not indicated without appropriate prior medical management in patients younger than 3 years, especially since anatomic development of the paranasal sinuses is limited and most cases are related to chronic adenoiditis in this age group. The panel agreed that imaging should not be performed for acute upper respiratory symptoms that have not been treated medically, particularly if symptoms have been present for less than 10 days. In the majority of patients with a common cold, acute changes will be noted on CT imaging, including mucosal abnormalities in the sinuses and changes in the osteomeatal region and nasal passages, often with fluid noted as well, and these findings can persist up to 6 weeks after symptoms have resolved. 11 Furthermore, imaging can be avoided in the pediatric population (in particular, patients younger than 3 years) if medical management has failed and diagnosis warrants an adenoidectomy alone. Computed tomography imaging was indicated for persistent symptoms in pediatric patients with chronic sinusitis after appropriate medical management and/or failure to improve following adenoidectomy. This recommendation mirrors the ACR Appropriateness Criteria, which also indicated that CT of the paranasal sinuses is the imaging modality of choice in patients with persistent sinusitis.
Complications of Sinusitis and Sinonasal Tumors
When evaluating the nasal and sinus cavity, information gathered from physical examination may be limited by what can be seen directly and endoscopically. Imaging may be used to provide more detailed information beyond the endoscopic visualization. This is important for the evaluation and management of tumor and infection that has extended outside the confines of the nasal and sinus cavities. However, CT imaging may not be enough to provide precise information, especially for tumor invasion into adjacent soft tissue structures and/or the skull base. Therefore, the use of MRI in addition to CT imaging is helpful in defining the true extent of a tumor. During the tumor resection, both the preoperative CT and MRI images may be fused together to create hybrid images that contain bony and soft tissue information to assist the surgeon in the complete oncologic resection of the tumor. An intraoperative CT image may also be used to confirm adequacy of resection of the tumor in real time; however, this is limited to bony tumors since intraoperative CT images are not optimal for soft tissue evaluation. Currently, intraoperative CT imaging is being used for complex revision sinus surgery and bony tumor and skull base resections as well. Postoperative CT images may also confirm a postoperative complication after endoscopic sinus surgery.
Medical Management
The consensus statement is primarily focused on indications for sinus CT imaging. Discussion regarding medical therapy and details of medical management are addressed in other guidelines. 12 There is strong evidence, for example, that nasal steroid sprays and saline lavages are helpful for chronic rhinosinusitis. 8
The presence of sinus abnormalities on CT does not necessarily indicate an infectious cause, but a sinus CT that is completely normal provides confirmation that initiation or continuation of antibiotics for sinusitis is inappropriate. Therefore, there was consensus that sinus CT is indicated in select patients (eg, gastrointestinal pathology, antibiotic intolerance, anticoagulation therapy) before prolonged courses of antibiotics are administered and in patients unresponsive to medical therapy.
The data regarding antibiotic therapy in acute rhinosinusitis are mixed. Most acute rhinosinusitis cases spontaneously resolve and therefore do not warrant CT imaging. Although a sinus CT image is recommended for patients with recurrent acute sinusitis, it is difficult to distinguish a viral cold from bacterial acute sinusitis in adults solely based on symptoms. In addition, 80% of patients with a cold will demonstrate sinus CT abnormalities that resolve or dramatically improve spontaneously within 2 weeks. 11 Therefore, it is reasonable to time the sinus CT for the patient with recurrent acute sinusitis to a period free of cold symptoms, in order to accurately evaluate irreversible mucosal and bony abnormalities and obstruction to sinus outflow tracts that will be amenable to possible surgical intervention. Nevertheless, CT imaging is valuable in patients with recurrent acute sinusitis symptoms where clinical evidence of a common cold or infectious rhinosinusitis is unclear. In addition, if the CT image is normal, the symptoms are not from sinusitis and will not be amenable to sinus surgery. For patients with persistent or recurrent facial pain or headache who are often misdiagnosed and treated for sinusitis but frequently have migraines, there may be value in objectively demonstrating to these patients the absence of sinus pathology on CT.
Patients frequently present with facial pain, and it is often difficult to distinguish possible odontogenic sinusitis from other causes of sinusitis. Although almost half of patients may complain of a foul odor, less than a third may complain of upper dental pain. Dental radiographs may miss up to 30% of these cases. Careful evaluation of the sinus CT for periapical lucenies will reveal dental causes often missed by Panorex or other dental films. 13
A trial of medical therapy is almost always recommended before sinus surgery is considered in the patient with uncomplicated sinusitis. A sinus CT image is not required before initiation of medical therapy in healthy patients with uncomplicated sinusitis since the end point in the management of acute sinusitis is resolution of the patient’s symptoms. If symptoms resolve with medical therapy, there is no indication for CT imaging, since this will not change patient management. Accordingly, consensus was obtained that CT imaging is not routinely indicated in patients who have had a full response to medical therapy (statement 1). In patients who fail to respond to medical therapy, a noncontrast sinus CT image is appropriate. The panel also reached consensus that plain X-rays and ultrasonography are not recommended for the evaluation of sinusitis (statement 9). In acute uncomplicated rhinosinusitis, a sinus CT image is not indicated (statement 3).
The panel agreed that suspected CSF rhinorrhea should prompt a sinus CT image, without a trial of medical therapy (statement 5). Cerebrospinal fluid rhinorrhea is suspected in patients with unilateral clear nasal drainage, or in the immediate postoperative period (iatrogenic) or trauma setting, and might also be suspected in a patient with headache beyond that expected following sinus surgery, or with altered mental status with or without clear nasal drainage.
In asymptomatic patients with special situations, sinus CT surveillance in conjunction with endoscopic and physical examination is appropriate, in the absence of medical therapy. Such situations include sinus tumor surveillance and sinus abnormalities that cannot be followed by nasal endoscopy, such as lateral frontal sinus or supraorbital ethmoid opacifications or mucoceles.
Surgical Planning and Dental Lift
Cone beam CT is widely used in otolaryngology, dental surgery, and oromaxillofacial surgery, and the clinician should always be mindful of the potential for overusing this technology. Cone beam CT has excellent spatial resolution and is well suited to paranasal sinus, temporal bone, and skull base imaging for assessment of bone windows, but it is not useful in patients in whom soft tissue resolution is necessary. Conventional CT and MRI scanning remain the best diagnostic modalities for soft tissue evaluation and are often used together in the assessment of skull base pathology, particularly if concern exists about possible intracranial involvement (eg, brain abscess) and for complications of sinusitis (eg, subperiosteal abscess) or complications related to sinus surgery. Cone beam CT can be helpful for intraoperative use for patients with complex skull base and craniofacial lesions. In a recent study, use of intraoperative CT scanning resulted in additional intervention being performed in 18% of cases, demonstrating an important adjunctive role that may improve clinical outcomes. 14
Point-of-service CT imaging, with CBCT devices or conventional CT, provides rapid, high-quality, and convenient imaging for patients. Prospective investigation has shown reduction in antibiotic overtreatment (60%-80%) and has also been shown to improve patient compliance with therapy.15,16 The panel agreed that the treating clinician may determine the type of CT imaging to be performed. The quality of the images obtained with both CBCT and conventional CT is appropriate for use in diagnosis and treatment, both in the clinical setting and also in the operating room when performing sinonasal and skull base surgeries, with or without intraoperative navigation.
Dental patients being considered for implant surgery and “sinus lift” are frequently referred for preoperative assessment of the maxilla and adjacent maxillary sinus. These patients typically require clinical evaluation and sinus CT imaging to assess possible maxillary sinus pathology and to evaluate the recipient maxillary bone to facilitate dental surgical treatment planning and to avoid complications following surgery to optimize clinical outcomes. Sinus CT imaging may also be necessary in the event of postoperative complications from dental surgery. Sinus CT imaging is also frequently used postsurgery to assess the outcome of sinus augmentation procedures prior to implant placement.
Conclusion
This consensus statement is aimed to help guide clinicians in the appropriate use of CT imaging for pediatric and adult patients with paranasal sinus and skull base disease and to promote the delivery of integrated, patient-centered care that will improve patient safety and outcomes.
Paranasal sinus CT imaging is a fundamental component of caring for patients with sinonasal and skull base pathology to confirm the diagnosis and eliminate the need for unnecessary medication and/or surgery. Using dose reduction protocols and adhering to the principle of “as low as reasonably achievable” is an important contemporary concept in CT imaging for children and adults, and in particular, pediatric dosing protocols are being refined to minimize radiation exposure in this vulnerable patient population. For children, careful consideration should be given when performing CT imaging but is needed in the setting of treatment failures and complications, either of the pathological process itself or as a result of iatrogenic (surgical) complications. For adults, imaging is necessary in surgical planning, for treatment of medical and surgical complications and all aspects of the complete management of patients with sinonasal and skull base pathology.
Disclaimer
Consensus statements are based on the opinions of carefully chosen expert panels and provided for informational and educational purposes only. The purpose of the expert panel is to synthesize information, along with possible conflicting interpretations of the data, into clear and accurate answers to the question of interest. Consensus statements may reflect uncertainties, gaps in knowledge, opinions, or minority viewpoints. Consensus statements do not purport to be a legal standard of care and are not clinical practice guidelines. The responsible physician, in light of all the circumstances presented by the individual patient, must determine the appropriate treatment, diagnosis, and management. Consideration of consensus statements will not ensure successful patient outcomes in every situation. The AAO-HNS emphasizes that these consensus statements should not be deemed to include all proper diagnosis/management/treatment decisions or methods of care, or to exclude other treatment decisions or methods of care reasonably directed to obtaining the same results.
Author Contributions
Disclosures
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.