
Abstract
Objective
The aim of this study is to evaluate the sensitivity parameters of the percentage of time the pH is <4 and >7, as well as the total number of laryngopharyngeal reflux episodes in 24 hours, in patients with suspected laryngopharyngeal reflux disease.
Study Design
Retrospective controlled study.
Setting
University hospital.
Subjects and Methods
The study was conducted on 46 patients with laryngopharyngeal reflux disease and 58 healthy controls. Patients and controls underwent 24 hours of dual-probe pH monitoring of the distal and cervical esophagus. Patients completed a Reflux Symptom Index questionnaire and underwent esophageal manometry. Data concerning the percentage of time the pH was <4 and >7 and the number of reflux episodes registered at the cervical esophagus were collected and evaluated.
Results
The percentage of time the pH is <4 and the number of laryngopharyngeal reflux episodes seem to be a reliable diagnostic laryngopharyngeal reflux criterion reaching satisfactory sensitivity (81% and 83%, respectively). Although the pH >7 parameter appeared statistically different between the 2 groups (P < .001), the sensitivity of the test appeared to be poor (55%).
Conclusion
Our study demonstrates the importance of the absolute number of laryngopharyngeal reflux episodes in 24 hours in the diagnosis of patients with suspected laryngopharyngeal reflux, proposing it as a new diagnostic criterion.
Laryngeal symptoms have been considered a manifestation of gastroesophageal reflux disease for a long time, and it is currently estimated that 4% to 10% of patients evaluated by otolaryngologists may have reflux-associated symptoms such as throat dryness, hoarseness, dysphonia, foreign body sensation, and other conditions not justified by other diseases. 1 However, only in recent years have the accompanying laryngopharyngeal symptoms related to acid reflux been investigated by otolaryngologists. As a result, a new syndrome called laryngopharyngeal reflux disease (LPR) has been identified. 2 Diagnosis based solely on clinical history and physical examination of the patient appears to be insufficient. In fact, LPR symptoms and physical findings can be present in up to 80% of the general population. 3 Furthermore, the use of scoring systems, such as the Reflux Symptom Index (RSI) or empirical trials with proton pump inhibitors, has been proposed. However, each of these diagnostic trials has revealed very little that is specific for this condition.1,4,5
Cervical esophageal pH monitoring is considered the best method for LPR diagnosis, although experts acknowledge the need to improve diagnostic accuracy and introduce new parameters. The pH <4 threshold used in proximal esophageal pH monitoring is currently considered the best index for LPR diagnosis.
Recently, Ayazi et al 1 proposed that the loss of alkalinization in the cervical esophagus may be responsible for the repeated pepsin activity in the larynx and pharynx. In fact, pepsin activity occurs at a pH of 6.5. 6 For this reason, the authors conducted a study proposing the percentage of time that cervical esophageal levels had a pH >7 as a new LPR diagnostic criterion. This, in combination with the percentage of time the pH is <4, achieved a 90% diagnostic sensitivity. 1 According to other studies, a modest and short acid exposure of the cervical esophagus exceeding the cricopharyngeal sphincter is sufficient to trigger LPR symptoms, since the epithelium of the upper airway is more susceptible to damage by stomach acid than the esophageal epithelium.7,8 This phenomenon has been considered by some authors, who defined even a single laryngopharyngeal reflux event as “abnormal” without really proposing or analyzing a numerical diagnostic cutoff.9,10 In summary, the impact of the total number of reflux episodes has not yet been quantified or analyzed in a controlled study with symptomatic LPR patients. The aim of this study is to evaluate the sensitivity parameters of pH <4 and pH> 7 times, as well as the total number of laryngopharyngeal reflux episodes (LPREs) in 24 hours. To this purpose, we compared a group of LPR patients and a healthy control group, both of which underwent a 24-hour dual-probe pH-metry.
Materials and Methods
Patients
We enrolled 2 groups of consecutive patients according to a planned recruitment between February 2009 and December 2011. The first group consisted of healthy subjects, in order to define the parameters of “normality” using the percentile method (95th percentile and 5th percentile). The second group consisted of subjects with LPR symptoms. Thirty-two patients refused pH-metry (29 potential controls and 3 LPR patients). Two patients (potential controls) were considered ineligible due to incomplete data. The pH-metric tracks were analyzed retrospectively. The study was approved by the Institutional Review Board and the Ethics Committee of the “Sapienza” University of Rome.
Control Group
We analyzed the pH-metric tracks of 46 controls selected from a group of 90 healthy volunteers who underwent dual-probe pH monitoring with no gastroesophageal reflux disease (GERD) or LPR symptoms. All underwent complete otolaryngological evaluation, a videoesophagram, esophageal manometry, and dual-probe pH testing to ensure that they had normal physiology and anatomy. Subjects with an abnormal composite pH score in the distal esophagus and hiatal hernia were excluded. These patients were defined as “normal,” although, when considering the selection criteria, few subjects could have been asymptomatic LPR patients. Tracing was analyzed with the aim of defining normal values for total percentage times that the cervical esophagus was exposed to pH <7 and pH <4 and the number of LPR events.
LPR Patient Group
We identified a group of 58 patients (1) for whom reflux was most likely the cause of symptoms, such as throat dryness, hoarseness, dysphonia, foreign body sensation, and so on, and (2) who responded to an empiric trial of reflux medications with complete relief of their LPR symptoms. Consequently, the response to medication was used as the diagnostic criterion for LPR. Using this selection criterion, we excluded LPR patients who did not respond to medical treatment from our evaluation, thus introducing a bias to this investigation. In our opinion, this was necessary since too many false positives otherwise would have been inevitably introduced.
Patients filled out an RSI questionnaire, and all scored above 13. We considered an RSI score greater than 13 to be abnormal, as reported in the literature. 11 All patients underwent esophageal manometry and dual-probe pH monitoring of the distal and cervical esophagus while being off acid suppression medication. We excluded the presence of all other pathologic conditions that could justify their symptoms, such as hiatal hernia and chronic laryngeal pathologies, in all patients.
Ambulatory pH Monitoring
No medication affecting gastrointestinal function was allowed during the monitored period. Patients and controls were instructed to follow a normal diet, remain in an upright or sitting position until going to bed at night, avoid eating or drinking between meals, and perform normal activities at home or at work.
Ambulatory 24-hour dual-probe pH monitoring was carried out using a Digitrapper pH 400 (Alpine BioMed, Fountain Valley, California). This pH-monitoring device consisted of a proximal and a distal probe, with a distance of 10 cm, 15 cm, or 18 cm between the probes.
The appropriate catheter was selected for each subject based on esophageal length (measured by manometry) so that when the distal pH sensor was positioned 5 cm above the upper border of the lower esophageal sphincter, the proximal sensor was placed in the cervical esophagus but below the lower border of the upper esophageal sphincter at a 1- to 3-cm distance for each patient.
The recorders were calibrated in pH 7 and 1 reference buffer solutions. Patients and controls switched the buttons in the data logger to record whether they were supine or upright and whether they were eating or not.
Analysis of pH Tracings
The probe was removed the following day. Information from the data logger was transferred to a computer for analysis using Gastro Trac software (Alpine BioMed). Through 24-hour dual-probe pH monitoring, we considered the total fraction of the time pH was <4 for the proximal and distal probe, the total fraction of the time pH was >7 for the proximal probe, and the total LPREs for the proximal probe. DeMeester scoring from the proximal probe was considered to define GERD diagnosis. 12 A laryngopharyngeal reflux episode was defined as a decrease in the pH level to lower than 4, measured at the proximal probe immediately following distal esophageal acid exposure without eating or swallowing.
Data and Statistical Analysis
The upper limit of normal for the percentage of time the pH was <4 in the cervical esophagus was calculated using the 95th percentile value in the subject group. This value was applied to the LPR group to determine the sensitivity of the pH <4 threshold in LPR diagnosis.
We then calculated the percentage of time the pH was >7 in the 58 asymptomatic subjects to define the lower limit of normal for exposure to pH >7 using the 5th percentile value. The sensitivity of the percentage of time the pH was >7 as a diagnostic criterion for LPR was compared with pH <4 exposure in the LPR group.
The normal upper limit of normal for the absolute number of LPREs was calculated by counting the LPREs and using the 95th percentile value in the subject group.
The Mann-Whitney U test was used for comparison of continuous variables between the groups. Values were reported as median and interquartile range (IQR). A P value of less than .05 was considered statistically significant. Statistical analysis was performed using SPSS version 15.0 for Windows (SPSS, Inc, an IBM Company, Chicago, Illinois).
Results
The controls consisted of 46 volunteers (25 men and 21 women) with a median age of 39 (26-42) years. The LPR patient group consisted of 58 patients (28 men and 30 women) with a median age of 51 (45-61) years. Of these 58 patients, 46 had typical GERD symptoms in addition to their LPR symptoms, and 12 patients had only LPR symptoms. Among the latter, GERD was suspected based on the results of the DeMeester score in 2 patients. 12
In the asymptomatic subjects, the median percent time of cervical esophagus exposure to pH <4 was 0.10% (IQR, 0.0%-0.20%) ( Figure 1 ). The upper limit of normality (95th percentile value) for exposure to pH <4 was 0.52% ( Table 1 ). The median percentage of time the cervical esophagus was exposed to a pH >7 was 70.3% (IQR, 61.1%-82.1%) ( Figure 2 ), and the lower limit of normality (5th percentile value) for pH >7 exposure was 54.3% ( Figure 2 ). The median LPREs was 1 (IQR, 0-3) ( Table 1 ), and the upper limit of normality for LPREs was 4.2 (95th percentile; Figure 3 ). For this reason, we considered >4 LPREs to be pathologic.
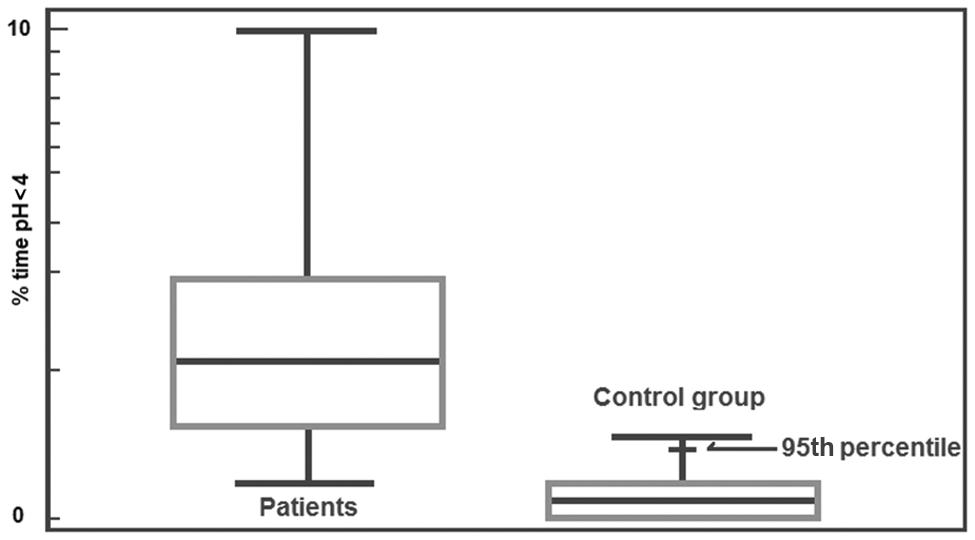
Cervical esophageal exposure to pH >4 in patients (n = 58) and the control group (n = 46).
Comparison between Controls and Patients with Laryngopharyngeal Reflux Using the Mann-Whitney U Test

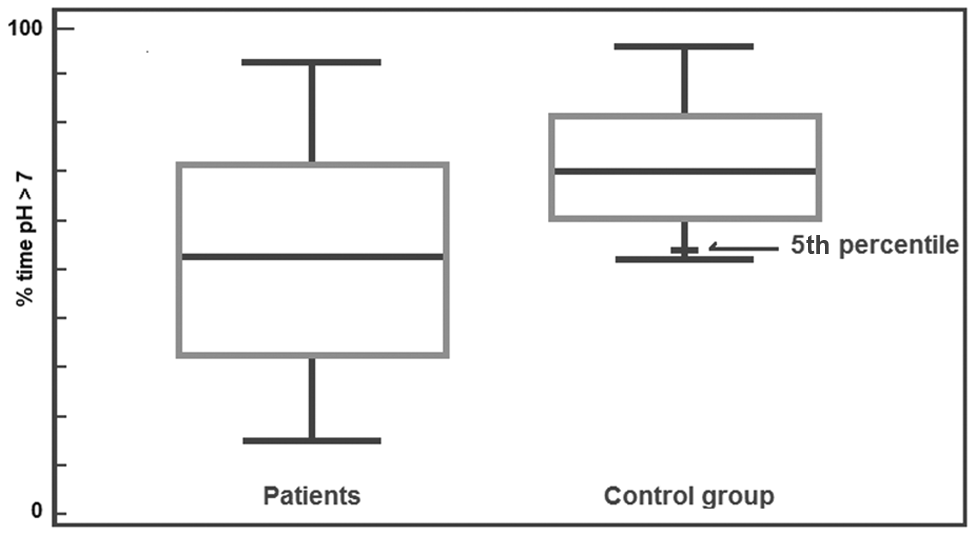
Cervical esophageal exposure to pH <7 in patients (n = 58) and the control group (n = 46).
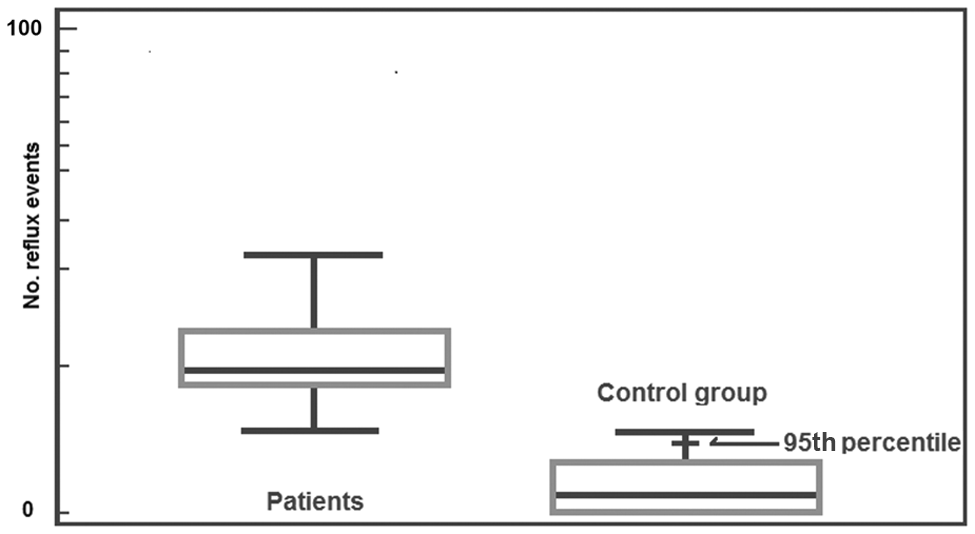
Laryngopharyngeal reflux events in patients (n = 58) and the control group (n = 46).
Patients with LPR symptoms had significantly greater reflux in the cervical esophagus, expressed as increased exposure to pH <4 (P < .001); had increased LPREs (P < .001); and failed to maintain a neutral pH in the cervical esophagus, as expressed by a lower exposure to pH >7 (P < .001), compared with asymptomatic subjects ( Table 1 ).
On the basis of conventional analysis of their pH tracings, 47 of 58 patients with LPR were considered abnormal using the percentage of time pH was <4, yielding a sensitivity of 81%. On the basis of their inability to maintain cervical esophageal pH >7, 32 of 58 patients were defined as abnormal, yielding a sensitivity of 55%. Using the absolute number of LPREs, 48 of 58 patients were defined as abnormal, yielding a sensitivity of 83% ( Table 2 ).
Patient Positivity to the Tests According to the Percentile Method
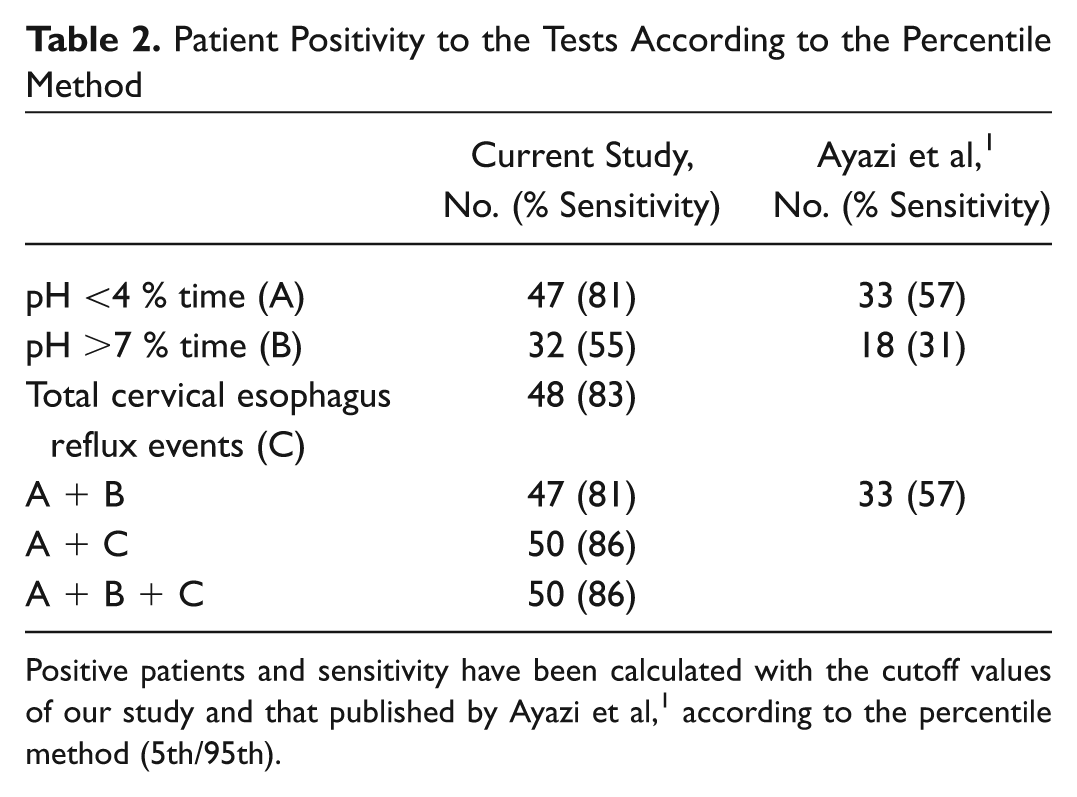
Positive patients and sensitivity have been calculated with the cutoff values of our study and that published by Ayazi et al, 1 according to the percentile method (5th/95th).
In 47 of 58 patients, the percentage of time the pH was <4 or >7 was abnormal, yielding an 81% sensitivity for identifying reflux as the cause of laryngopharyngeal symptoms. We did not observe increased sensitivity when combining the 2 parameters.
In 50 of 58 patients, the percentage of time the pH was <4 or the number of LPREs was abnormal, yielding an improved sensitivity for identifying reflux as the cause of laryngopharyngeal symptoms of 86%.
In using the normality parameters recently proposed by Ayazi et al, 1 we found a decrease in sensitivity in the ability to identify symptomatic individuals in terms of the percentage of time the pH was <4 and >7, which stood at 57% and 31%, respectively. When we considered the 2 parameters together, we did not observe an increased sensitivity ( Table 2 ).
Discussion
The prevalence of LPR was estimated to be approximately 80% in patients with voice hoarseness and around 50% in patients with laryngeal symptoms.13-17 However, although many physicians believe the condition is still underdiagnosed, many also suspect overdiagnosis and misdiagnosis in many patients. Diagnosis and management of LPR remain controversial for at least 2 reasons:
Absence of convincing evidence regarding techniques for establishing a definitive diagnosis and causation
Studies have reported conflicting conclusions
Medical history–based and physical examination–based LPR diagnosis is unlikely since common signs and symptoms occur in many other medical conditions (Reinke’s edema, globus pharyngeus, laryngeal hyperirritability, laryngospasm, chronic posterior and diffuse laryngitis, diffuse laryngitis, laryngeal granuloma) and in up to 80% of the general population.2,18,19
The difficulty in establishing LPR diagnostic criteria also lies in the absence of clarity in the relationship between GERD and LPR. Conventionally, LPR was considered an extraesophageal component of GERD and then was taken to exclude LPR in the absence of GERD. However, published studies show that reflux may be responsible for mainly laryngeal or mainly gastroesophageal symptoms.16,20
In a study conducted by Ossakow et al 20 on 2 groups of patients (36 gastrointestinal and 63 otolaryngologic patients), it emerged that none of the gastroenterologic patients had hoarseness, but all the otolaryngologic patients did. Only 6% of the otolaryngologic patients had heartburn, whereas it was reported in 89% of the gastroenterologic patients.
These conclusions were supported by Wiener et al, 16 stressing that gastric acid can reflux through the esophagus to the larynx without causing esophageal injury in transit.
These findings, albeit with lower rates, were also supported by our study. Of 58 patients, only 12 had exclusively laryngeal symptoms (21%).
In our opinion, GERD and LPR share the same pathophysiology, but the laryngopharynx and esophagus do not have the same defense mechanisms against the acid. For this reason, one episode of reflux, especially if short-lived, may be responsible for pharyngolaryngeal symptoms but not esophageal ones. However, this phenomenon has not yet been analyzed in a controlled study with symptomatic subjects since the parameters actually studied (percentage of the time the pH is <4 or >7) take into account only the percentage of time of acid exposure and not the acute damage caused by the number of reflux episodes even during the 24 hours.
With this background, the present study is affected by a nonnegligible bias in patient selection. In fact, since the pH study could not be used as an inclusion criterion, patients and controls were enrolled according to symptoms, RSI, manometry, and response to antireflux therapy. These parameters, even when combined, do not represent highly sensitive diagnostic criteria. Consequently, although we performed an accurate patient selection, patients and controls still may not represent absolutely true “normal” and true LPR patients. Among patients, in fact, we did not include LPR patients who did not respond to therapy. Among controls, a few asymptomatic LPR patients most likely were included. However, this selection bias is a usual confounder in LPR studies.
The percentage of time the pH is <4 for the proximal electrode in a dual-probe catheter analysis is actually considered the diagnostic gold standard for LPR. 1 In our study, the application of this parameter yielded a high sensitivity (81%).
It was recently proposed by Ayazi et al 1 that the loss of alkalinization in the cervical esophagus may be responsible for the repeated activity of pepsin in the laryngopharynx compartment. Its activity has been shown to reach up to a pH 6.5 level. For this reason, the authors proposed the percentage of time the pH is >7 as a new criterion for the diagnosis of LPR on a sample. This finding, in combination with pH <4, yielded a 90% sensitivity compared with 69% reached as pH <4 alone.
However, in our study, we considered the percentage of time the pH is >7 by calculating the normal range in a group of our healthy patients. The difference between the patient group and the control group was statistically significant (P < .0001). Thirty-two of 58 patients who were unable to maintain cervical esophageal pH >7 were defined as abnormal, yielding a sensitivity of 55%, whereas Ayazi et al 1 reported an 84% sensitivity. Furthermore, by applying the cutoff values proposed by Ayazi et al 1 to our group, the sensitivity drops to 33% ( Table 2 ).
In 47 of 58 patients, the percentage of time the pH was <4 or >7 was abnormal, yielding a nonincremented sensitivity (81%) compared with the single parameters. In light of our results, the percentage of time the pH was >7, although statistically significantly different between the 2 groups, did not imply any advantage.
Using the percentage of time the pH was >7 was justified by the preserved activity of pepsin up to pH 6.5 and its failure to achieve degradation up to pH 8. However, pepsin activity at pH 6 is about 10 times lower than that found at pH 2 and about 5 times lower than that found at pH 4. 17 There are also no data concerning the efficacy of the laryngeal mucosal defense mechanisms between pH 5 and 7. For these reasons, we believe there are not enough data to argue that the failure to maintain a pH >7 could justify laryngeal mucosal damage. In contrast, studies on laryngeal tissue grown in vitro have shown that cell damage starts from an exposure less than or equal to pH 5 and that the damage is enhanced by the presence of pepsin. 21 At these pH values, the cellular response to an inflammatory stimulus increases depending on (1) how low the pH is and (2) how long the tissue is exposed. However, the most significant changes at transcript levels were measured within 60 seconds of exposure, suggesting that a longer exposure time does not necessarily translate into greater or more extensive damage.
In light of these considerations, we chose to analyze the absolute LPRE number during 24 hours.
Using the absolute number of LPR events, 48 of 58 patients were defined as abnormal, yielding a sensitivity of 83% ( Table 2 ). In 50 of 58 patients, the percentage of time the pH was <4 or the LPRE was abnormal, yielding an improved sensitivity of 86% for identifying reflux as the cause of laryngopharyngeal symptoms.
Conclusion
The study confirmed that the percentage of time the pH is <4 is a reliable diagnostic LPR criterion in LPR diagnosis, reaching a satisfactory sensitivity in symptomatic LPR patients. The pH >7 parameter appeared statistically different between the 2 groups, but the sensitivity of the test appeared to be poor.
The absolute number of LPREs in 24 hours was statistically different between the 2 groups and reached a good sensitivity. Although the sample taken for analysis does not allow us to reach definitive conclusions, our study highlights the importance of the absolute number of LPREs in 24 hours in the diagnosis of patients with suspected LPR.
Further larger studies with selection criteria based on the gold-standard diagnostic tests are needed to validate these results and to propose LPRE as a valid diagnostic criterion, particularly when combined with the percentage of the time the pH is <4.
In our opinion, and also as reported by Ayazi et al, 1 these studies highlight that cervical esophageal pH monitoring is the most objective method for diagnosing LPR, but its accuracy must be improved by also proposing and introducing new diagnostic quantitative and qualitative parameters.
Author Contributions
Disclosures
Footnotes
Acknowledgements
We are grateful to Maria Grazia Saladino for her valuable contribution in the editing of the manuscript. Armando De Virgilio (corresponding author) had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
No sponsorships or competing interests have been disclosed for this article.