
Abstract
Objective
Use of neomycin eardrops in nonintact tympanic membranes (NITMs) due to tympanic membrane (TM) perforation or tympanostomy tubes (TTs) is controversial because of the potential for ototoxicity. We sought to compare the risk of sensorineural hearing loss (SNHL) in patients with NITMs who received neomycin with those who received fluoroquinolone eardrops.
Study Design
Retrospective cohort study.
Setting
Administrative claims data analysis, including diagnoses and procedure detail for physician office and hospital visits and pharmacy dispensing events in children eligible for Medicaid fee-for-service benefits in 29 states between 1999 and 2006.
Subjects and Methods
Eligible patients (age <18 years) had to have received a study eardrop within 12 months after first diagnosis of NITM. The follow-up period started from the first eardrop dispensing.
Main Outcome Measures
We compared the 12-month risk of SNHL using Cox proportional hazards regression models adjusted for SNHL risk factors.
Results
We found 982 SNHL cases in 134,598 children treated with neomycin or fluoroquinolone eardrops. The adjusted hazard ratio (HR) for 1, 2, and 3 or more prescriptions of neomycin was 0.90 (95% confidence interval [CI], 0.76-1.07), 1.45 (1.05-2.01), and 1.30 (0.71-2.36), respectively, when adjusted for SNHL risk factors, the interval between initial diagnosis of NITM and eardrop initiation, and total number of eardrop prescriptions. The results remained unchanged for several sensitivity analyses.
Conclusion
Short-term use of neomycin eardrops in patients with NITMs is not associated with an increased risk of SNHL; however, repeated doses (ie, ≥2 prescriptions) showed a significant association with an increased risk of SNHL.
Nonintact tympanic membranes (NITMs) due to otitis media or tympanostomy tube (TT) placement are common in children.1,2 Otitis media is a leading cause for health care visits, totaling 709 million cases annually worldwide. 3 Chronic suppurative otitis media with tympanic membrane perforation (CSOM) occurs at an annual rate of 0.48% (31 million cases). 3 More than 1 million TTs are placed in the United States each year, with approximately 7% of all children receiving tubes by age 3 years. 4 Most children with TTs develop otorrhea, which is typically treated with antibiotic eardrops. 5 Ototopical formulations are chosen because of higher bacteriological response rates and a reduced risk for adverse effects and antibiotic resistance compared with systemic antibiotic administration.6,7
Eardrops instilled into the ear canal may traverse the NITM, penetrating the middle ear, and thus raising the potential for ototoxicity.8-10 There has been convincing evidence in animal experiments that topical application of aminoglycosides can cause ototoxicity. 11 In humans, aminoglycoside eardrops are instilled through TTs for chemical ablation of vestibular function in Ménière’s disease. 12 Accordingly, the expert consensus panel of the American Academy of Otolaryngology–Head and Neck Surgery recommends against the use of topical aminoglycoside eardrops with an NITM. 8 Instead, fluoroquinolones are promoted over aminoglycosides in such cases because of the lack of ototoxicity.8,13 However, clinicians may prescribe topical aminoglycoside eardrops when there is a previous treatment failure with fluoroquinolone drops, if culture results suggest quinolone drops would not be appropriate, or if drug formulary plans do not provide suitable alternatives. 8 Furthermore, although neomycin eardrops have been available in routine clinical practice for decades, case reports of ototoxicity due to neomycin eardrops have been rare.14,15 Thus, opinions about risks and benefits of neomycin eardrops differ, perhaps also driven by typically higher cost of the alternative, quinolones. 16
A review published by the British Association of Otolaryngologists emphasized the lack of well-designed human studies concerning ototoxicity from eardrops, 17 and indeed, no controlled study has evaluated neomycin eardrop risk in children with NITMs. The objective of this study was to assess the comparative risk of neomycin vs fluoroquinolone eardrops when used by patients with evidence of a recent NITM.
Methods
Data Source and Cohort Assembly
The study cohort was assembled from 29 US states’ Medicaid Extract Files (MAX), maintained by the Centers for Medicare & Medicaid Services (CMS), and included all children eligible for Medicaid fee-for-service benefits between 1999 and 2006. MAX provides monthly detail on Medicaid eligibility, sociodemographic information, and diagnoses and procedures associated with inpatient and outpatient service claims, as well as dispensed prescriptions by pharmacies. MAX has been used successfully for pharmacoepidemiologic research, including a variety of pediatric safety studies.18,19 Patients, ages 0 to 18 years, were included in the study after their first diagnosis of NITM, defined as TT placement (Current Procedural Terminology [CPT] code 69433 or 69436), first diagnosis of CSOM (International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM] codes 382.1, 382.2, and 382.3), or perforation of the tympanic membrane (ICD-9-CM codes 384.2x) identified from either inpatient or outpatient service claims. We required patients to have continuous Medicaid enrollment for at least 6 months before their first diagnosis of NITM. Furthermore, eligible subjects had to have received neomycin or fluoroquinolone eardrops within 12 months after the tympanic membrane perforation and had to have continuous Medicaid eligibility for another 12 months following first eardrop administration. The date of the first study drug dispensing was defined as the index date. We followed patients from the index date until the first occurrence of sensorineural hearing loss (SNHL) or the end of study (12 months after the index date).
Patients were excluded if they had inpatient or outpatient claims with diagnoses of conductive hearing loss (ICD-9-CM codes 389.0x), SNHL (ICD-9-CM codes 389.1x), mixed hearing loss (ICD-9-CM codes 389.2x), or unspecified hearing loss (ICD-9-CM codes 389.7, 389.8, and 389.9) during the 6-month period before the index date. In addition, we excluded patients with significant risk factors for SNHL during the 6 months before the index date or during follow-up, including evidence of status post–organ transplant, malignant neoplasm, syphilis, toxoplasmosis, rubella, cytomegalovirus infection, albinism, neurological conditions (congenital anomalies of the nervous system, hereditary and degenerative disease of the central nervous system, injury to nerves and spinal cord), severe head injury, head or neck radiation, retinitis pigmentosa, heavy metal poisoning, burns, decompression sickness, bacterial meningitis, viral encephalitis, or exposure to systemic aminoglycosides, interferon, cisplatin, cyclosporine, vinblastine, vincristine, or phosphodiesterase inhibitors (see the Appendix, available at otojournal.org).
Study End Point
Occurrence of SNHL was defined as a medical encounter with a diagnosis code for SNHL (ICD-9-CM codes 389.1x [excluding 389.14] and 389.2x) that occurred within 60 days after or up to 7 days before audiometric testing (CPT codes 92553, 92557, 92585, 92586, 92588, 92579, and 92582).
Drug Exposure
In this comparative safety study, fluoroquinolone eardrops were chosen as the reference for all analyses because they are equally effective as aminoglycoside drops and have not been found to have ototoxic effects.8,20 For each day of follow-up, we attributed subject time to either neomycin or quinolone use based on the first pharmacy eardrop claim that established the study index date. If a patient who was originally started on quinolones was switched to neomycin, follow-up time after the switch was assigned to neomycin. In contrast, a patient originally started on neomycin was not reassigned even if switched to quinolones, because neomycin effects might be diagnosed delayed and would be erroneously attributed to quinolones and because quinolones are not expected to contribute to SNHL. Neomycin use was further categorized into 1, 2, or 3 or more filled prescriptions (updated for each day of study follow-up) to capture potential cumulative effects. Because repeated use of eardrops might signalize more severe otologic problems, which may contribute to SNHL, we adjusted for the total number of filled study eardrop prescriptions (regardless of drug class) updated for each day of follow-up.
Covariates
Covariates, measured during the 6-month period preceding the index date, included patient demographics (age, sex, race) and comorbidities (immunodeficiency conditions, fetal alcohol syndrome, craniofacial conditions, hyperbilirubinemia, hypothyroidism, sickle cell disease, mastoiditis, vestibular disorders, history of heart disease, kidney disease, diabetes mellitus, and cleft palate or cleft lip) (Appendix). We also adjusted for calendar year to take into account the trend of decreasing neomycin use. 21 We further adjusted for the time between initial diagnosis of NITMs and index dispensing of a study eardrop, as well as underlying cause of NITM (TT vs perforation).
Statistical Analysis
We estimated multivariate-adjusted hazards ratios (HRs) and 95% confidence intervals (CIs) using time-dependent Cox proportional hazards regression. We included all baseline risk factors or potential confounders for SNHL in the Cox model as indicated previously. For sensitivity analysis, we restricted our analysis to children with NITMs due to TT placement for more exact timing of tympanic membrane perforation. Analyses were conducted using SAS version 9.2 (SAS Institute, Cary, North Carolina). All tests were 2-sided, with a P value less than .05 suggesting statistical significance. The study protocol was approved by the CMS and University of Florida Institutional Review and Privacy Boards.
Results
Of the 155,238 children who had claims suggesting an NITM and who subsequently received neomycin or quinolone eardrops between 1999 and 2006, 20,181 patients were excluded due to comorbidities or use of medications that have been associated with SNHL. The final study cohort included 134,598 patients; 27,144 were new users of neomycin, and 107,454 initiated fluoroquinolone eardrops. A total of 18,619 (13.8%) of these patients received both neomycin and fluoroquinolone eardrops during the follow-up period. Of 27,144 neomycin initiators, 8859 (33%) switched to the quinolone eardrop; among 107,454 quinolone initiators, 9742 (9%) had neomycin dispensed during the follow-up.
Table 1 presents baseline patients characteristics. Compared with fluoroquinolone users, neomycin users were older, less likely to have had TT insertion, and started antimicrobial treatment slightly later. Two-thirds of neomycin dispensing occurred in 1999-2002, whereas the majority of fluoroquinolone eardrops were dispensed in 2003-2006.
Characteristics of Study Participants by Index Prescription
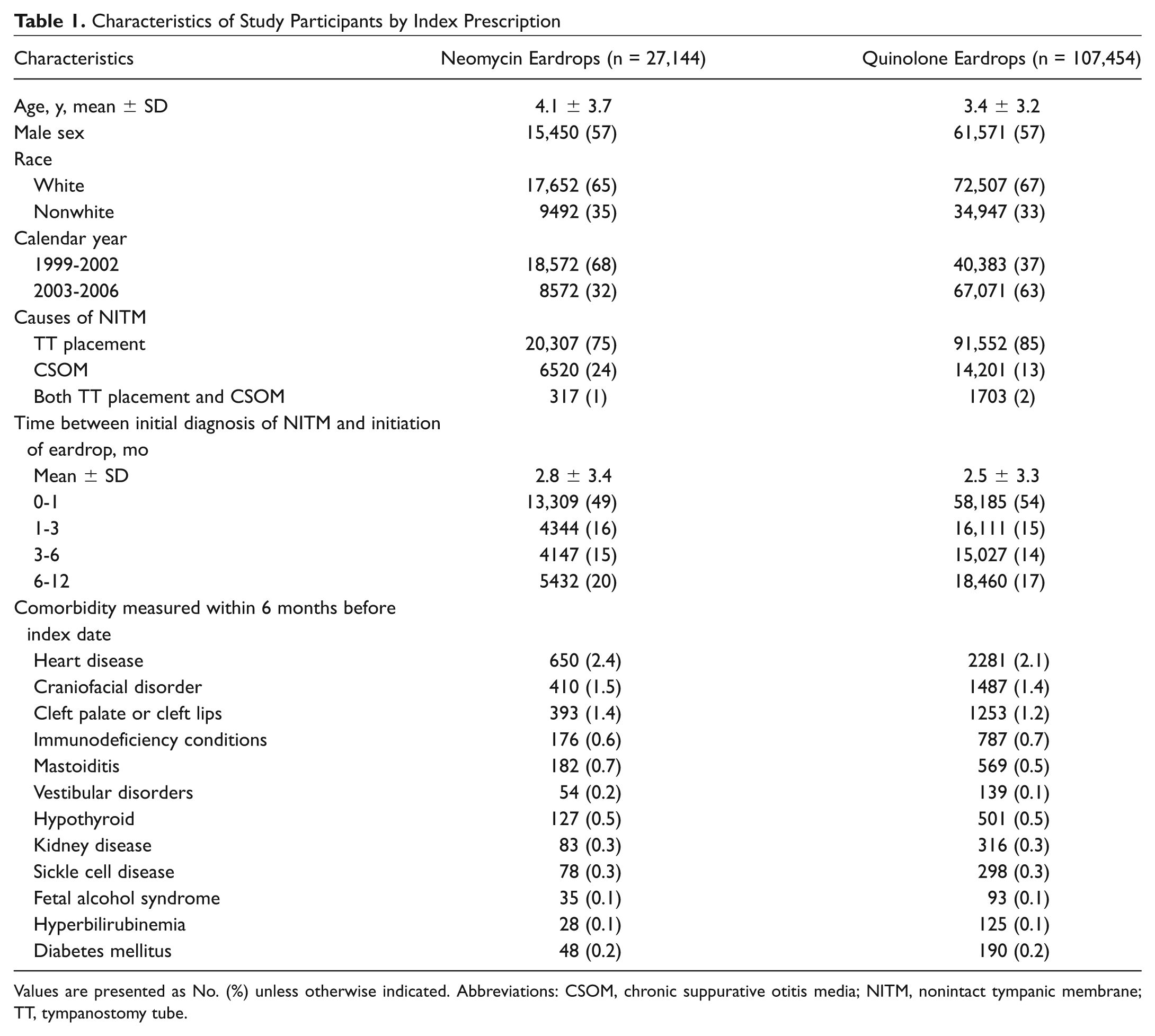
Values are presented as No. (%) unless otherwise indicated. Abbreviations: CSOM, chronic suppurative otitis media; NITM, nonintact tympanic membrane; TT, tympanostomy tube.
We identified a total of 982 incident SNHL cases, resulting in an overall annual incidence of 7.3 per 1000 children who received study eardrops ( Table 2 ). Compared with the time patients were only exposed to quinolone eardrops, there was no suggestion of an increased risk of SNHL during the time patients had filled 1 prescription of neomycin eardrops (adjusted HR = 0.90; 95% CI, 0.76-1.07). However, the multivariate-adjusted HR was statistically significant (HR = 1.45; 95% CI, 1.05-2.01) when time after the second neomycin prescription fill was considered. The trend continued when time during more than 2 prescriptions was analyzed (HR = 1.30; 95% CI, 0.71-2.36), but confidence intervals were wide due to the small number of cases (n = 12). Note that the number of filled quinolone prescriptions was balanced in this analysis of cumulative neomycin use because of the adjustment for the total number of eardrop prescriptions.
Associations between SNHL, Antibiotic Eardrop Use, and Other Baseline Covariates among Patients with NITM (n = 982)
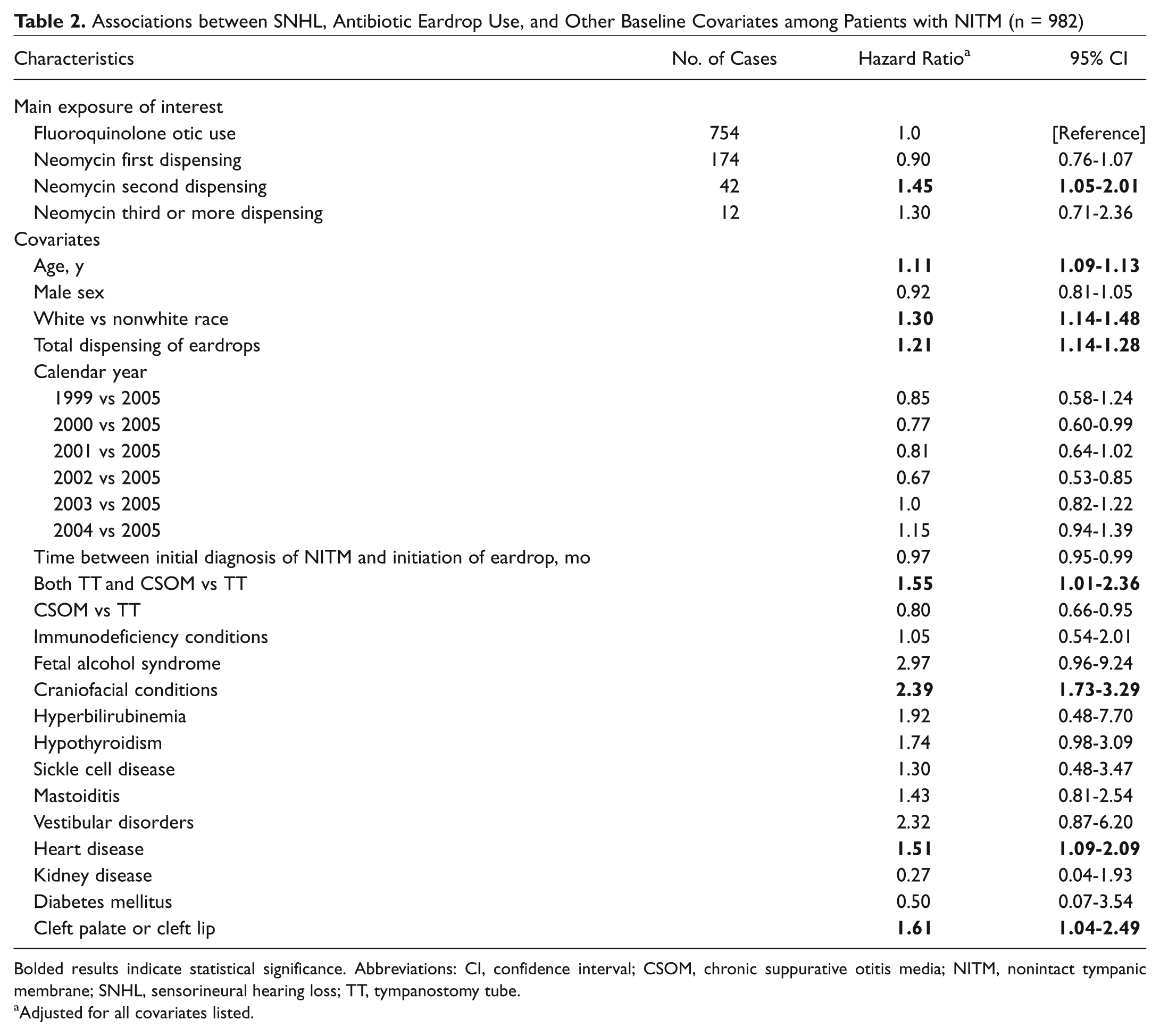
Bolded results indicate statistical significance. Abbreviations: CI, confidence interval; CSOM, chronic suppurative otitis media; NITM, nonintact tympanic membrane; SNHL, sensorineural hearing loss; TT, tympanostomy tube.
Adjusted for all covariates listed.
Several risk factors for SNHL were prominent in this cohort, including fetal alcohol syndrome (HR = 2.97; 95% CI, 0.96-9.24), craniofacial conditions (HR = 2.39; 95% CI, 1.73-3.29), and cleft palate or cleft lip (HR = 1.61; 95% CI, 1.04-2.49). In general, the associations for other predefined risk factors were in the correct direction that would be expected ( Table 2 ). Sensitivity analyses revealed similar results, but confidence intervals became wider due to the reduced number of cases. Restriction to patients with TT placement resulted in 785 incident cases of SNHL. The adjusted HR was 0.90 (95% CI, 0.73-1.10), comparing times during first neomycin use to quinolone use, and 1.50 (95% CI, 1.07-2.10) for times after 2 or more prescriptions for neomycin were filled ( Table 3 ).
Associations between SNHL and Antibiotic Eardrop Use among Patients Who Had TT Placement (n = 785)
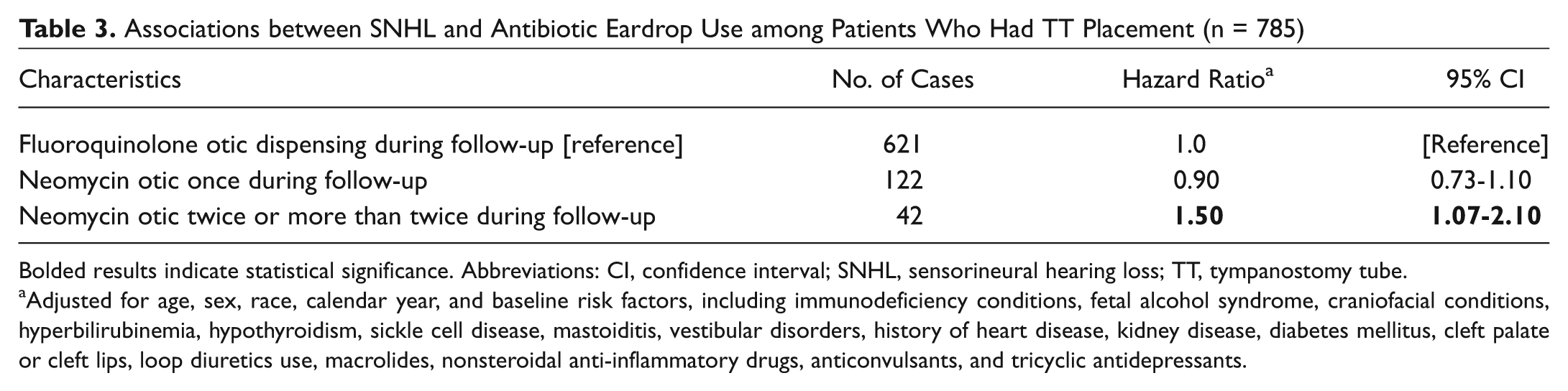
Bolded results indicate statistical significance. Abbreviations: CI, confidence interval; SNHL, sensorineural hearing loss; TT, tympanostomy tube.
Adjusted for age, sex, race, calendar year, and baseline risk factors, including immunodeficiency conditions, fetal alcohol syndrome, craniofacial conditions, hyperbilirubinemia, hypothyroidism, sickle cell disease, mastoiditis, vestibular disorders, history of heart disease, kidney disease, diabetes mellitus, cleft palate or cleft lips, loop diuretics use, macrolides, nonsteroidal anti-inflammatory drugs, anticonvulsants, and tricyclic antidepressants.
Discussion
There is strong evidence from animal studies that all topical aminoglycoside eardrops are ototoxic in the presence of NITMs. 11 In humans, the most compelling evidence for the ototoxic potential of aminoglycoside eardrops is the relatively consistent loss of vestibular and cochlear function that is observed in patients with Ménière’s disease treated with gentamicin solution through a TT. 12 Ototoxicity is usually seen within 2 weeks of therapy. 12 Inner ear function is commonly compromised in patients with Ménière’s disease, limiting generalizability to the population typically exposed to aminoglycoside eardrops.
Aminoglycoside eardrops have been used extensively to treat otitis media with TT and CSOM, 21 but reports of hearing loss associated with aminoglycoside eardrops and NITMs are relatively sporadic. 10 Some case series with relatively small numbers of patients did not find SNHL with single dose, 22 5 days, 16 or 14 days 23 of neomycin eardrop administration following TT placement. Miro 24 reported 1 case of SNHL in 113 adolescents and adults treated after neomycin eardrops for CSOM. None of the studies on neomycin risk in TT or CSOM involved repeated dosing, long-term follow-up, or sufficient power to detect differences in relatively uncommon adverse events, such as SNHL.
In this large cohort of children with NITMs, we did not see a significant association between short-term use of topical neomycin eardrops (ie, 1 dispensing within 12 months after initial diagnosis of NITM) and an increased risk of SNHL compared with fluoroquinolone eardrops; however, we found evidence of an increased risk of SNHL in ears with NITMs receiving repeated doses of neomycin eardrops. Our findings suggest that neomycin penetration through the NITM and into the inner ear is usually limited, and larger doses or longer administration windows may be needed to produce harm. The fact that sustained use was associated with an increased risk for SNHL does suggest, however, that penetration can occur and result in significant damage.
To place our findings in perspective, when applying the 45% increase in hazard to the baseline rate of hearing loss in quinolone users (7.4 per 1000 patient-years), approximately 3.3 new cases of SNHL would be expected per 1000 children with 2 or more neomycin eardrop prescriptions. The clinical implications of these findings are consistent with established recommendations for the treatment of otitis media with NITM. 8 When possible, fluoroquinolone eardrops should be used preferentially over neomycin eardrops. If neomycin eardrops are to be used, patients should be monitored for ototoxicity, especially if a repeated course is to be prescribed. As overuse of ototopical agents by patients is common, 25 patients and families must be appropriately counseled about the risks of treatment and overtreatment.
It is important to note that our study cannot exclude the risk for SNHL associated with single use of neomycin. First, because of preexisting ear problems and young age, hearing problems, especially mild SNHL, may not be recognized until after our 12-month follow-up period. Second, reliance on pharmacy dispensing data does not guarantee administration or capture eardrops that were provided to the patient during the clinic visit or after surgery. These misclassifications of exposure may have compromised correct assignment of patients to exposure groups and biased our results toward the null hypothesis (no effect or HR = 1). Third, although our 12-month follow-up time period is expected to comprise the time period where TTs remain patent 26 and perforations have not healed, 27 some tympanic membranes might have been intact by the time of neomycin administration and thus not susceptible to toxic effects. We attempted a sensitivity analysis stratified by initiation of study eardrops relative to diagnosis of NITM, but our sample size became too small for meaningful inferences. Fourth, we did not evaluate the validity of ICD-9-CM and CPT codes for identification of SNHL but assumed that the diagnosis coupled with the respective audiology exam would establish satisfactory validity. However, reliance on this algorithm may have missed cases, again resulting in misclassification and bias toward the null hypothesis.
Methodological issues that may have biased our study toward a neomycin effect should be considered as well. First, initiation of neomycin may be associated with more severe ear disease and thus increased risk of SNHL. We adjusted our analysis for a variety of risk factors, but residual confounding may exist. Similarly, switching to neomycin may reflect higher disease severity, but restriction of our analysis to nonswitchers resulted in similar HR point estimates even though confidence intervals became wide. The fact that neomycin use decreased over the study period suggests that physician choice was primarily driven by increasing adoption of fluoroquinolones rather than underlying disease severity. Furthermore, utilization of an active control group minimizes the chance for confounding as both aminoglycosides and quinolones have demonstrated efficacy in the treatment of otitis media, and thus, disease severity is expected to be similar. We further reduced the likelihood of confounding inherent in differential patient progress during the follow-up period by adjusting for total number of eardrops received, a proxy for progression of the underlying ear disease.
Finally, we cannot exclude the chance for diagnostic bias, as physicians might be more likely to suspect SNHL in patients with recent exposure to neomycin eardrops and thereby order diagnostic workups more frequently. However, we compared the rate of hearing tests and found approximately 5% of subjects in either exposure group had CPT codes for hearing tests, suggesting the likelihood of diagnostic bias is minimal.
Additional study strengths are inherent in its size and source population. This is the first large controlled population-based study to evaluate the comparative safety of 2 commonly prescribed eardrops in patients with NITMs. Its sample size enabled us to evaluate risk for a rare but serious adverse drug effect, examine dose-response relationships, and adjust for a large number of SNHL risk factors. Enrollment of children in Medicaid allowed us furthermore to focus on a more vulnerable population representing more than a quarter of all children in the 29 study states.
Conclusion
Repeated exposure of ears with NITMs to neomycin eardrops is associated with an increase in SNHL compared with fluoroquinolone eardrops. Clinicians who are treating patients with NITMs should try to avoid the use of potentially ototoxic eardrops.
Author Contributions
Disclosures
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.