
Abstract
Objective
Adenotonsillectomy (TA), performed for obstructive sleep apnea (OSA) or recurrent tonsillitis (RT), has been associated with weight gain after surgery. The objective of this study was to look at a large population of children undergoing TA and the demographic factors that contribute to postoperative weight gain.
Study Design
Case series with retrospective chart review.
Setting
Tertiary, urban academic care center.
Subjects and Methods
Children undergoing TA at an academic center between 2008 and 2011 were included in this study. Demographic data (age, gender, race), OSA disease severity, preoperative and 3- to 6-month postoperative normalized body mass index (BMI; z-scores), and changes in z-scores were compared.
Results
Complete weight data after TA were available for 115 children, 85 of whom underwent surgery for OSA. Mean age (7.2 ± 4.3 vs 7.3 ± 4.4 years, P = .955) and gender distribution (38% female vs 50% male; P = .323) were similar for the OSA and RT groups. However, children with OSA were more likely to be black (60% vs 33%) than RT patients (P = .026). Overall, the preoperative BMI z-score increased from 0.98 ± 1.50 to 1.21 ± 1.25 (P = .0009) with no difference by surgical indication (P = .58). Multiple linear regression analysis demonstrated that only age was significantly, and negatively, associated with changes in BMI z-scores (P = .015).
Conclusions
Similar to previous studies, children had weight gain after TA. In this analysis, younger age (≤6 years) was a significant predictor of postoperative weight gain. Future research should prospectively evaluate the association between weight gain and demographic factors in children undergoing TA, with special attention to the relationship with age.
Both recurrent tonsillitis (RT) and obstructive sleep apnea (OSA) are associated with hypertrophy of tonsillar and adenoid tissue and are common otolaryngologic problems encountered by general and pediatric otolaryngologists. OSA is the most severe type of sleep-disordered breathing (SDB). 1 OSA is thought to exist in approximately 1% to 4% of children in the United States.2-5 More importantly, if untreated, OSA is known to have significant long-term consequences, including behavioral disorders, pulmonary and cardiovascular complications, and decreased quality of life.6-8 RT can be caused by a host of pathogens, most commonly group A streptococcus. Although RT can affect a person at any age, recurrent and chronic tonsillitis are more common in children than adults. A common treatment for both RT and SDB is an adenotonsillectomy (TA). TA is now the second most common ambulatory procedure performed in children in the United States, with approximately 530,000 performed in children younger than 15 years in 2006. 9
Decreased dietary intake and failure to thrive (FTT) have been documented in patients with both recurrent acute tonsillitis10,11 as well as SDB.12,13 FTT in this patient population has been attributed to an array of problems, some of which include dysphagia with decreased caloric intake, increased nighttime work of breathing with resulting heightened energy consumption, and fluctuations in nightly growth hormone secretion.14-16 TA has even been recommended for children with a single diagnosis of FTT. 17
Although TA has been used for many years, increasing evidence suggests that it may be responsible for changes in weight following surgery above and beyond what would be expected with resolution of RT or SDB. Significant weight increases in children following TA have been reported in multiple studies.18-23 This finding is, however, complicated by the fact that obesity in children has dramatically increased over the past several decades, with as many as 17% of children today categorized as obese. 24 Some studies would suggest that weight gain could simply occur with resolution of FTT.20,25 However, much controversy still exists concerning weight gain following TA, including whether or not it is a result of the surgery itself, improvement in the underlying pathology, or changes in inflammatory biomarkers. The purpose of this study was to evaluate the association of demographic factors with weight gain following TA in children.
Materials and Methods
Inclusion Criteria
Children who underwent TA for RT or OSA at an urban academic tertiary care center between 2008 and 2011 were identified retrospectively. Children between the ages of 12 months and 18 years who underwent polysomnography (PSG) for OSA diagnosis before surgery were included ( Figure 1 ). An array of data from the charts were analyzed, including demographic data, primary complaint, OSA disease severity, results from PSG, and preoperative and 3- to 6-month postoperative normalized body mass indexes (BMIs), as defined by z-score. Children were categorized as having RT if they presented with a primary complaint of recurrent acute tonsillitis and had no associated clinical signs or symptoms of OSA or SDB or also had an initial PSG showing an apnea-hypopnea index (AHI) <1.5. Children were categorized as having OSA if they had a preoperative polysomnogram that showed a respiratory disturbance index ≥1.5. Because this was a retrospective chart review, an expedited institutional review board approval was obtained, and all identifying data were protected throughout the data extraction process. The expedited review was conducted by the Johns Hopkins Medicine Institutional Review Board. All patients in this study received a TA by one of the pediatric otolaryngologists at the Johns Hopkins School of Medicine. Children who were younger than 12 months old, had significant comorbidities/syndromes, or did not have complete weight data from the electronic medical records were excluded from this study.
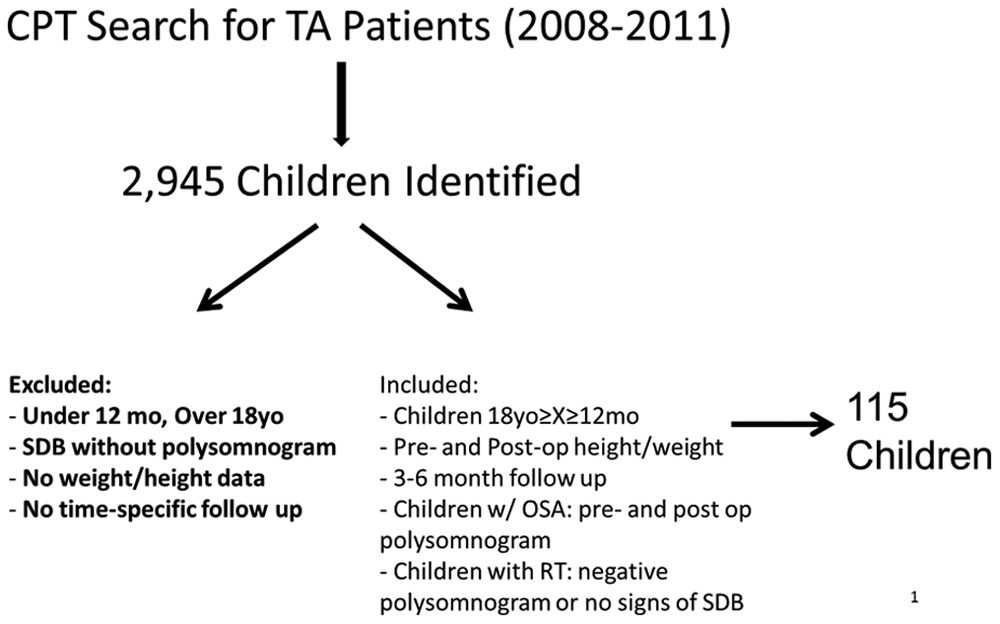
Algorithm for patient inclusion.
PSG Data
The electronic medical record was used to extract data from overnight 16-channel PSG. Most of these studies were performed at the Johns Hopkins Sleep Laboratory using Somnologica or REMLogic (Embla, Broomfield, Colorado). For monitoring throughout the PSG, recorded signals included electrocardiogram, left and right electro-oculograms, electroencephalograms (with leads C3-A2, C4-A1, and O1-A2), tibial electromyogram, submental electromyelogram, and oxyhemoglobin saturation (Masimo, Irvine, California). All participants had respiratory effort assessed with both abdominal and thoracic inductive plethysmography (Embla), as well as assessment of an end tidal CO2 (Novametrix, Murrysville, Pennsylvania). Body position was observed with the use of an infrared video camera, and airflow was monitored with a differential pressure transducer (Pro-Tech, Mukilteo, Washington) connected to a nasal cannula (Salter Labs, Arvin, California). If snoring was encountered during the sleep study, it was graded subjectively using a clinical scale of 1 (least) to 4 (greatest) by the sleep technologist, using guidelines routinely implemented at this institution. All results were interpreted by board-certified pediatric sleep medicine physicians.
Z-Score and Weight Measurements
Patient data extracted during the chart review process included race, sex, 1-month preoperative and 3- to 6-month postoperative height and weight. Height and weight were directly measured in the outpatient pediatric clinics at Johns Hopkins Hospital. BMI is an index of relative body fat calculated using height and weight; however, the definitions for obesity vary by age and sex in children. For this reason, the pediatric BMI values were normalized using a z-score, which uses height, weight, age, and sex to measure obesity. A z-score calculator was used from the Centers for Disease Control and Prevention website. 26 For this study, a z-score greater than 2.0 was considered overweight and greater than 3.0 morbidly obese, per the World Health Organization guidelines. 27
Statistics
Standard statistical analysis, including descriptive statistics and the Mann-Whitney U test, were used to evaluate differences in demographic data between the patients in the different indication groups. The Student t test was used to compare differences in BMI z-score by age. Multivariate linear regression modeling was also performed with Stata 12 (Stata Corporation, College Station, Texas) and GraphPad Prism 5.0 (GraphPad Software, San Diego, California) to show the relationship between age, race, sex, and surgical indication with postoperative weight changes. The t test was used to compare postoperative weight changes by age category (≤6 years or >6 years). Six was selected for the cutoff as the peak age for tonsil removal in children is between 2 and 6 years of age, and previous studies of much larger and less selected patient cohorts undergoing TA found the mean age to be 5.6 years. 28 P values of <.05 were used to determine significance throughout the analysis.
Results
One hundred fifteen patients who underwent TA for RT or OSA were included for analysis; 85 were diagnosed with OSA and 30 with RT. Of the total group, 42 (41%) were female, while 15 (50%) were female in the RT group and 57 (38%) were female in the OSA population (P = .323; Table 1 ). The age of the overall cohort ranged from 1.4 to 16.8 years, with a mean of 7.2 ± 4.3 years, while the mean ages for the RT and OSA populations were 7.3 ± 4.4 years and 7.2 ± 4.3 years, respectively. The OSA cohort included more black children (60% vs 33%) than the RT cohort (P = .026).
Demographic Data and Physical Examination Characteristics for Patients Diagnosed with Either Recurrent Tonsillitis or OSA Who Obtained a TA with Preoperative and 3- to 6-Month Postoperative Weight Measurements
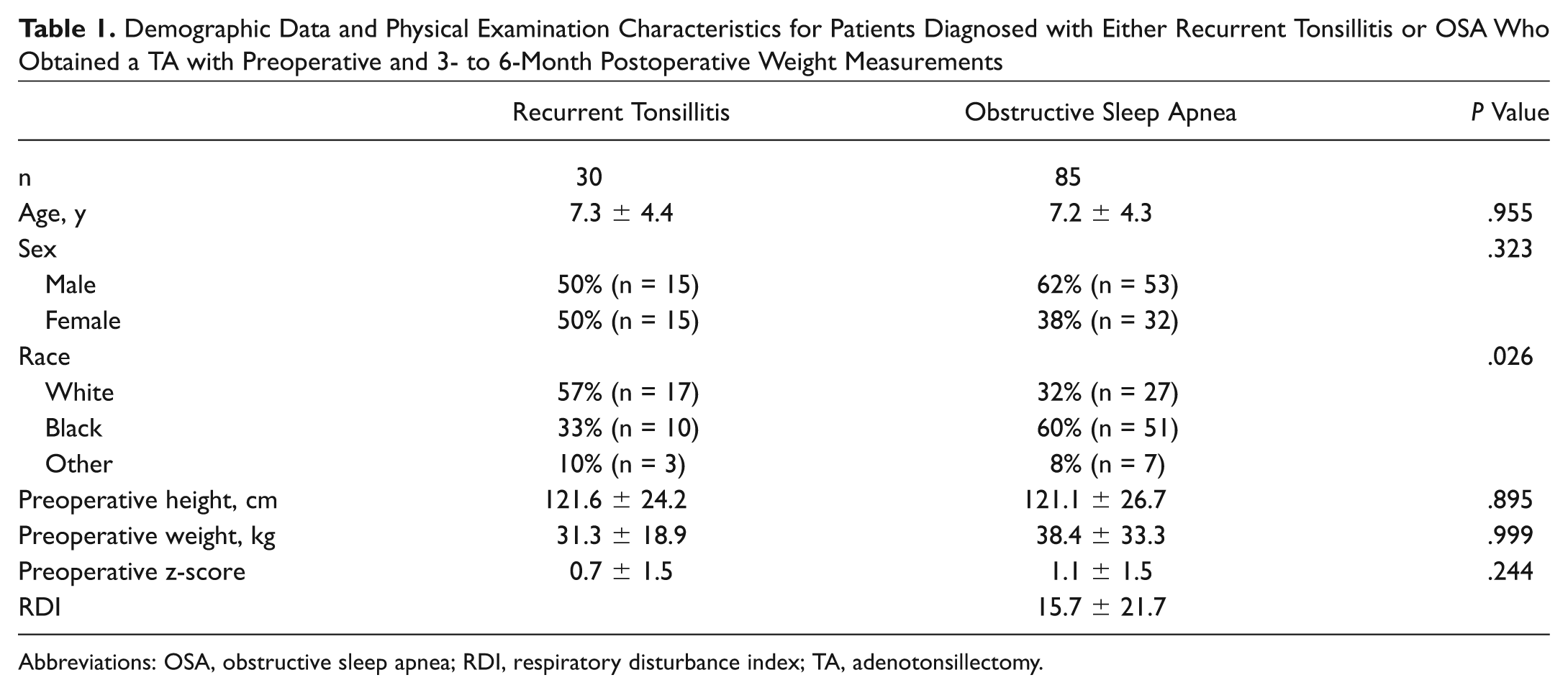
Abbreviations: OSA, obstructive sleep apnea; RDI, respiratory disturbance index; TA, adenotonsillectomy.
The preoperative height for the RT and OSA groups were 121.6 ± 24.2 cm and 121.1 ± 26.7 cm, respectively, with no significant difference, as seen in Table 1 . The preoperative weight for the RT and OSA groups were 31.3 ± 18.9 kg and 38.4 ± 33.3 kg, respectively. The preoperative z-scores for the RT and the OSA groups were 0.70 ± 1.47 and 1.07 ± 1.51, respectively, and these increased to 0.87 ± 1.16 and 1.33 ± 1.27, respectively ( Figure 2 ). Overall, the z-score for the total patient population significantly increased from 0.98 ± 1.50 (~85%) before surgery to 1.21 ± 1.25 (~87%) after TA (P = .0009), with no significant difference by surgical indication (P = .58).
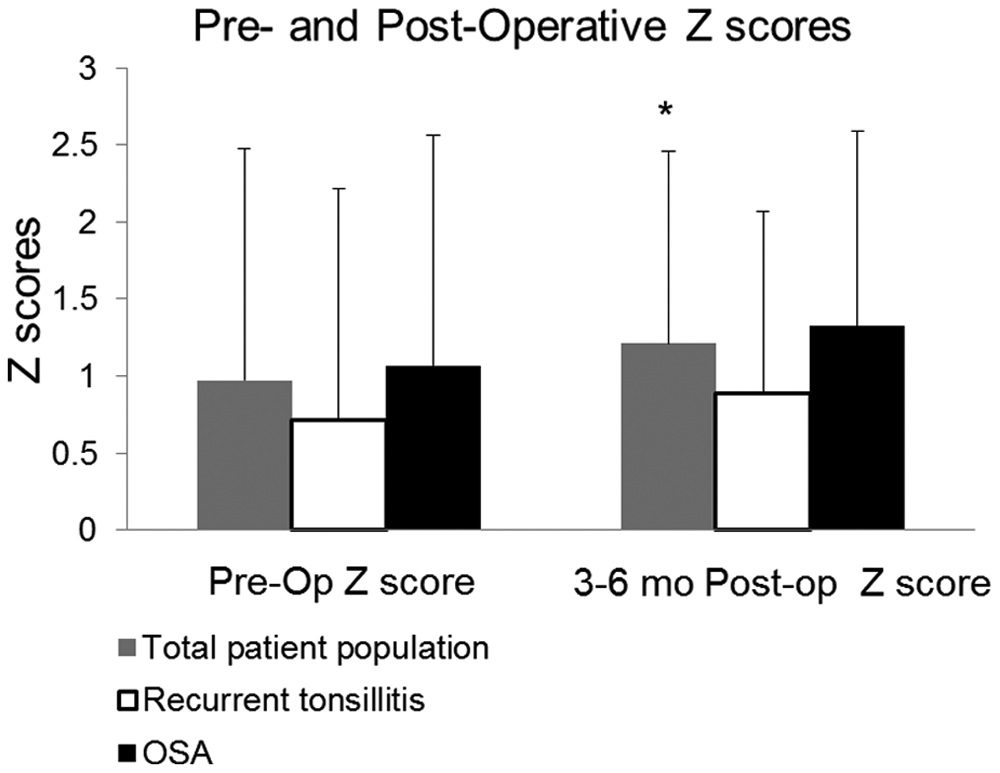
Preoperative and 3- to 6-month postoperative z-scores for the overall, tonsillitis, and obstructive sleep apnea populations. There was no significant difference between groups, although there was a trend toward increased z-scores after adenotonsillectomy.
Multivariate linear regression modeling found that the significant change in z-score after surgery was not significantly modified by surgical indication, race, or sex, as seen in Table 2 ; age, however, was a significant factor when viewed as a continuous variable. Further analysis with a Student t test demonstrated that children 6 years of age and younger had a significant increase in their BMI z-score while those children older than 6 years were found to have no significant change in weight after surgery ( Table 3 ). Those children 6 years old and younger had a mean preoperative z-score of 0.55 ± 1.5 (~67th percentile) and a mean postoperative z-score of 0.98 ± 1.3 (~84th percentile), while those children older than 6 years old had a mean preoperative z-score of 1.37 ± 1.4 (~92nd percentile with a mean postoperative z-score of 1.43 ± 1.2 (~92nd percentile; Table 4 ). In the multiple linear regression analysis, only age was significantly, and negatively, associated with changes in BMI z-scores (P = .015).
Multiple Linear Regression Analysis of Demographic Factors Related to Change in Standardized Body Mass Index after Adenotonsillectomy
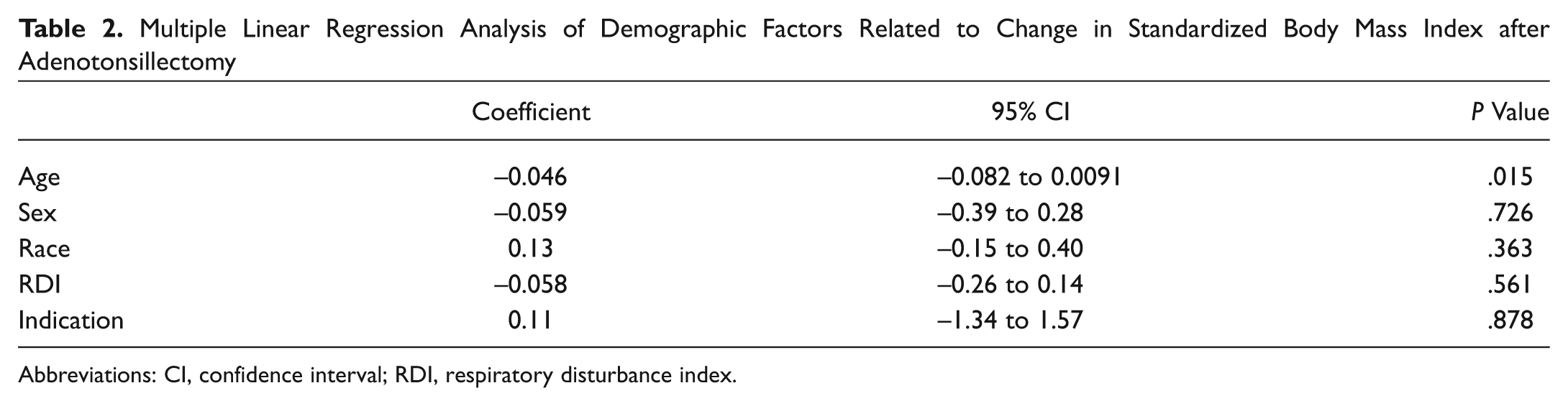
Abbreviations: CI, confidence interval; RDI, respiratory disturbance index.
Statistical Comparison between Groups by Surgical Indication, Age, Race, and Sex
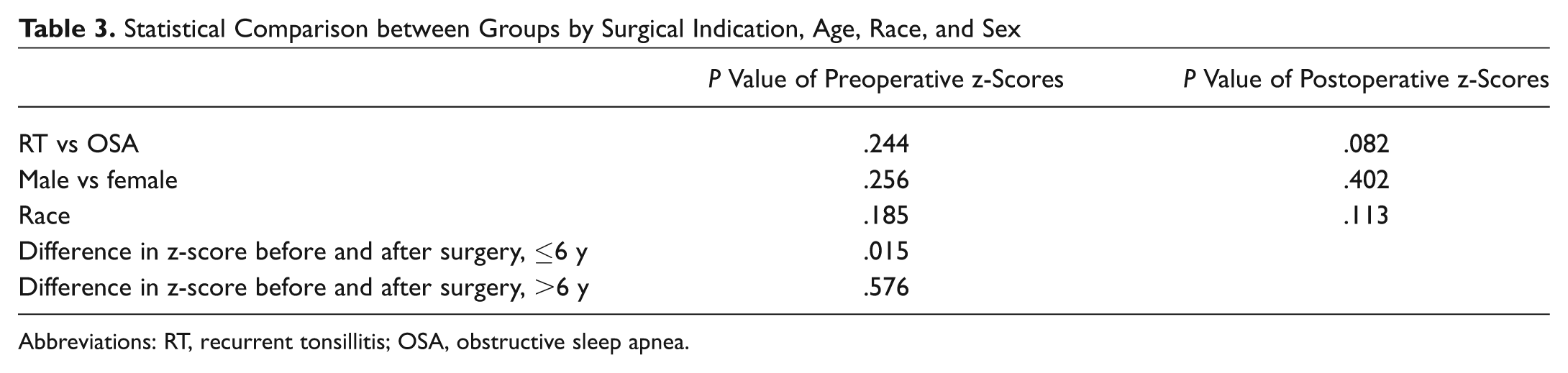
Abbreviations: RT, recurrent tonsillitis; OSA, obstructive sleep apnea.
Difference in z-Score before and after Adenotonsillectomy in Children Categorized by BMI Status prior to Surgery
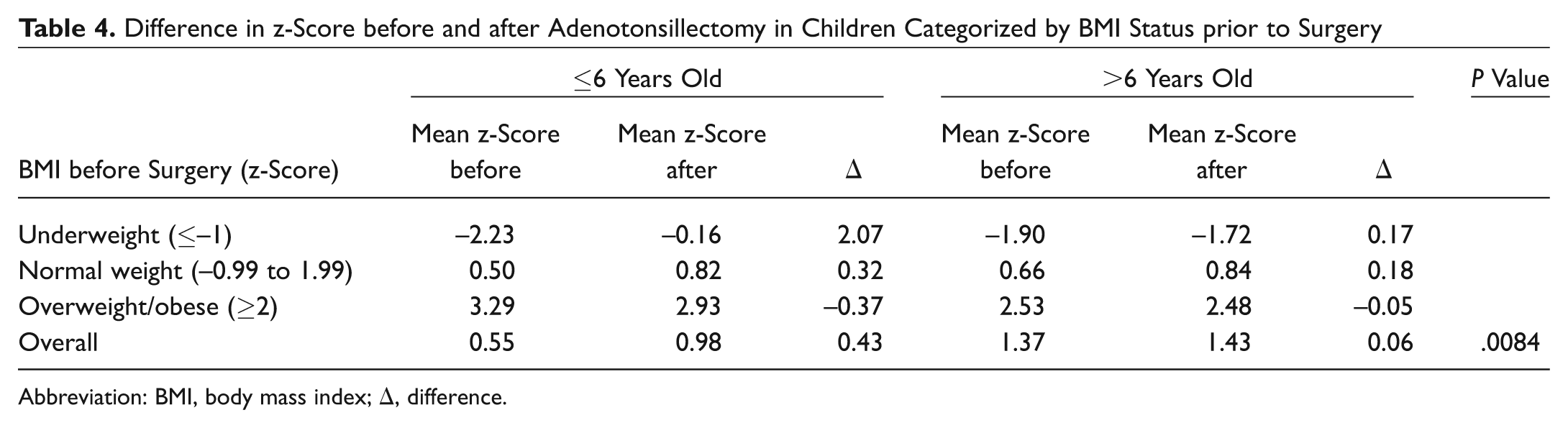
Abbreviation: BMI, body mass index; Δ, difference.
Discussion
This study suggests that weight gain after TA in children is variable and dependent on age. In this study, a nonsnoring patient population diagnosed with recurrent tonsillitis is directly compared with a population with OSA diagnosed by PSG. While indication for surgery was not a significant factor in weight gain, age was significant, with children 6 years old and younger more likely to gain weight after surgery than those older than 6 years.
Previous studies have investigated the role of TA in weight gain in children with both OSA and RT. A study of 55 patients with RT found that TA resulted in significant increases in standard mean normal weight; however, the authors did not analyze by age or compare to other patients with SDB. 19 Kiris et al 22 found that z-scores significantly increased after surgery in children who had OSA or RT; however, PSG was not performed to confirm the presence or absence of OSA. A different meta-analysis found that standardized weight significantly increased in children after TA, regardless of indication. 17 This analysis did not use PSG to confirm OSA. 17 A separate meta-analysis found that both normal and overweight children who underwent TA for various indications gained more than expected weight, but the methods to measure weight and weight gain were variable. Finally, a large study of the Dutch birth cohort found that TA between the ages of 0 and 7 years resulted in overweight or obesity by age 8. 29 All of these studies mentioned that weight gain was a direct result of TA, regardless of surgical indication or age group; however, the lack of definitive diagnosis of OSA by PSG made interpretation of the results less clear.
Several publications attempted to compare children based on clinical indication for TA or suggested that the weight gain was a recovery from failure to thrive seen with adenotonsillar hypertrophy. For example, in a study of 41 children, 75% were found to gain weight significantly when age-corrected weight was measured. 25 Nieminen et al 20 concluded that children with obstructive sleep apnea syndrome (OSAS) had significant increases in BMI compared with patients who underwent TA for primary snoring. 20 Although the authors used PSG to diagnose patients with OSAS, only 19 children with OSAS underwent TA, and none of the children with RT had surgery, limiting the comparison control group. 20
Within the literature, many methods have been used to calculate weight changes in children. Weight percentile and z-scores have been commonly used for standardized anthropometric measurements; however, other methods have included standardized weight, BMI, and even fat-free mass. This variability in how weight is measured in children was exemplified in the meta-analysis by Jeyakumar et al, 18 in which the groups had to be divided based on BMI, standardized weight scores, or corrected weight due to the variability of the previous publications. Z-score, when compared with other forms used for calculating weight, is calculated based on weight distribution of the reference population. 30 It is also a standardized quantity, so it can be extrapolated across age and sex. 30 Finally, it can be used to examine the extremes of growth status. 30 For these reasons, z-score was used to standardize all weight measurements in this article. Based on the data from this study, the mean for children younger than 6 years was within the normal range, with a large percentage of these children actually considered underweight. However, the mean z-score for children older than 6 years in this study was, on average, considered overweight.
The current study demonstrates that weight gain in children who underwent TA is variable depending on age. Unlike many other studies, these data suggest that young children, many of whom were normal weight or underweight prior to the TA, have significant weight gain after the procedure. Those children who are overweight before the TA remain, on average, overweight after the procedure.
This study does have limitations. Because this is a retrospective review, it is possible that data were miscollected or misinterpreted during the collection process. With this study, there is a significant risk of examination bias based on whether or not physical examination data were originally reported and included in the electronic medical records, which determined the inclusion/exclusion of the original patient population. Initially, 2945 children who had undergone TA from 2008 to 2011 were identified. However, after excluding those patients who did not have recorded height and weight, preoperative and postoperative PSGs, or follow-up within the specified time frame, only 115 patients (3.9%) met criteria for the control or TA group in this study. Given the large number of excluded patients, a selection bias may exist. Although all patients with OSA were categorized by PSG, the patients with RT did not all undergo sleep studies. Some patients who presented with symptoms of RT as well as snoring were included in the control population if the initial PSG showed an AHI <1.5. However, the RT patients who did not obtain an initial PSG were screened for signs of SDB including snoring and were negative by history. Moreover, a large population of children with OSA was identified in this study; however, only 30 children were identified who met the inclusion criteria for recurrent tonsillitis without any snoring or history of SDB. Finally, because of the retrospective nature of this evaluation, we were not able to follow the BMI trajectory of children who did not undergo further otolaryngology evaluation as a control group. However, future studies in large hospital systems with fully integrated electronic medical records will facilitate this evaluation.
Conclusions
Much controversy exists concerning the effect that TA plays on weight in children. Prior research suggests that the surgical procedure itself may be responsible for postoperative weight gain in children. Moreover, some prior research suggests that the weight gain is primarily seen in those patients obtaining TA for OSA and not in those patients who undergo TA for infectious indications. In the current analysis, TA specifically resulted in weight gain in younger children (≤6 years) who are more likely to be normal weight or underweight preoperatively. Children older than 6 years who were, on average, overweight, in fact remain overweight without any significant increase in BMI score. Prospective, long-term studies are needed to further elucidate the relationship between child age, TA, and weight gain.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.
Presented as an oral presentation at the 2012 American Academy of Otolaryngology—Head and Neck Surgery Foundation Annual Meeting; September 12, 2012; Washington, DC.