
Abstract
Objective
Describe single-stage removal of head and neck venous malformations using percutaneous embolization with n–butyl cyanoacrylate (n-BCA) glue prior to surgical resection.
Study Design
Case series with chart review.
Setting
Tertiary-care pediatric hospital.
Subjects and Results
A total of 169 venous malformations were identified between 2000 and 2012, and 102 (60.1%) were in the head and neck. Thirty-five of 102 (34.3%) were observed, 56 of 102 (54.9%) had invasive therapy, and 11 of 102 (10.8%) underwent n-BCA embolization and surgery (“GES procedure”). The median age of the glue embolization and surgery cohort was 14 years (range, 6-19), and 7 of 11 (63.6%) were female. Treated venous malformations involved the oral cavity/tongue (4/11; 36.4%) and parotid/face (7/11; 63.6%). During facial lesion excision, intraoperative facial nerve monitoring was used. All surgical sites (11/11) were closed primarily. No patient in this cohort had any posttreatment nerve deficits, dysarthria, and dysphagia or lesion persistence.
Conclusions
Localized venous malformations can be treated with preoperative percutaneous embolization with n-BCA glue followed by surgical excision. This technique, with selective motor nerve monitoring, appears safe and allows for complete venous malformation removal with limited nerve dissection, to allow maximal tissue and functional preservation.
Keywords
Venous malformations (VMs) are common vascular anomalies with a population incidence of 1% to 4%. 1 They comprise ectatic, slow-flow, venous channels that are usually present at birth and grow commensurately with the patient 2 and commonly occur in the head and neck region with a predilection for the oral cavity, airway, and muscle groups. 3 Critical structures, skin mucosa, and nerves are frequently next to head and neck VMs, complicating treatment, particularly with surgical resection since VM bleeding during treatment makes visualization difficult and injury easy. Sometimes this close relationship of VMs to neurovascular structures makes invasive therapy contraindicated if risks associated with VM resection outweigh possible improvements in appearance or function.
A variety of treatment options for VM treatment have been described, including conservative measures, irradiation, electrocoagulation, cryotherapy, 4 sclerotherapy, laser photocoagulation, and surgical resection. 3 Conservative management of VMs is generally reserved for small, isolated, asymptomatic lesions. Larger symptomatic lesions often need treatment. Irradiation and electrocoagulation have been described in the past but are not currently used. Laser therapy, using Nd:YAG, CO2, and KTP, has been important in the management of VMs involving skin and mucosa.5-7 Superficial components of intraoral or airway VMs can be treated with serial laser therapy using a flexible fiber-optic delivery system. 8 Laser therapy is used serially as the deeper portions of the VM are not eradicated with these devices. Interstitial Nd:YAG laser therapy has been reported in deep VM treatment, but there is a paucity of data on their safety since laser tissue destruction is unpredictable. In particular, neural or skin injury from deep tissue laser injury is a major consideration, especially in the head and neck.9,10 Percutaneous sclerotherapy, usually multiple stage, of head and neck VMs leads to sclerosant-induced VM inflammation and thrombosis.11-13 Inflammation-induced complications, including skin and mucosal injury, airway compromise, infection, nerve, injury, and cardiovascular collapse, can limit sclerotherapy use.14,15
Current VM management is aimed at reducing cosmetic deformity, dysfunction, and pain, while minimizing treatment complications. 16 Surgical excision, with or without adjunctive laser treatment or sclerotherapy, continues to be a good treatment option in VM management. 14 Large, diffuse VMs pose a challenge as intraoperative bleeding makes preservation of critical structures difficult, even with multimodal therapy. 14 Preoperative sclerotherapy of facial VMs is associated with less operative time per lesion volume and less operative blood loss. 17 Additional strategies, including the use of recombinant factor VIIa to reduce intraoperative bleeding, have been described as safe and effective. 18 Even with optimal therapy, especially in head and neck VMs, leaving behind residual VM is inevitable. Moreover, after therapy, revascularization for wound healing can potentially result in new VM tissue that may be harder to eradicate than the initial VM. n–Butyl cyanoacrylate (n-BCA) (Codman & Shurtleff and Johnson & Johnson, Raynham, Massachusetts) has been used extensively because of its chemical properties, and the tissue reaction is mild in comparison to other cyanoacrylate derivatives. 19 This glue is approved by the US Food and Drug Administration for high-flow cerebral arterial malformations and has been used extensively to treat intracranial and extracranial arteriovenous malformations. When used, n-BCA is dispersed under direct fluoroscopic guidance into the venous channels in contact with the vessel wall, and the acute inflammatory reaction that develops soon after percutaneous embolization leads to a demarcation line between the VM and healthy tissue. This facilitates the complete removal of VM with minimal morbidity and recurrence.
Head and neck VMs have a wide variation in size and extent and can persist with any treatment. Some VMs are localized to a given anatomic region, such as the skin and buccal region ( Figure 1 ). These we have called “localized” or unifocal, sporadic head and neck VMs, analogous to stage 1 and 2 lesions described by Goyal et al 20 in 2002. All invasive VM treatments have potential for vital structure injury and cosmetic disfigurement, particularly with diffuse VMs, where complete eradication is impossible due to unacceptable morbidity. Localized VMs also pose treatment challenges as they can be directly adjacent to easily injured vital structures, which limits treatment extent and efficacy. Staged glue embolization followed by partial and complete resection has been described. 21 Because of the treatment challenges and risks associated with staged VM treatment, we describe an innovative technique for single-stage removal of localized head and neck VMs using percutaneous embolization with n-BCA glue prior to surgical resection (“GES procedure”).
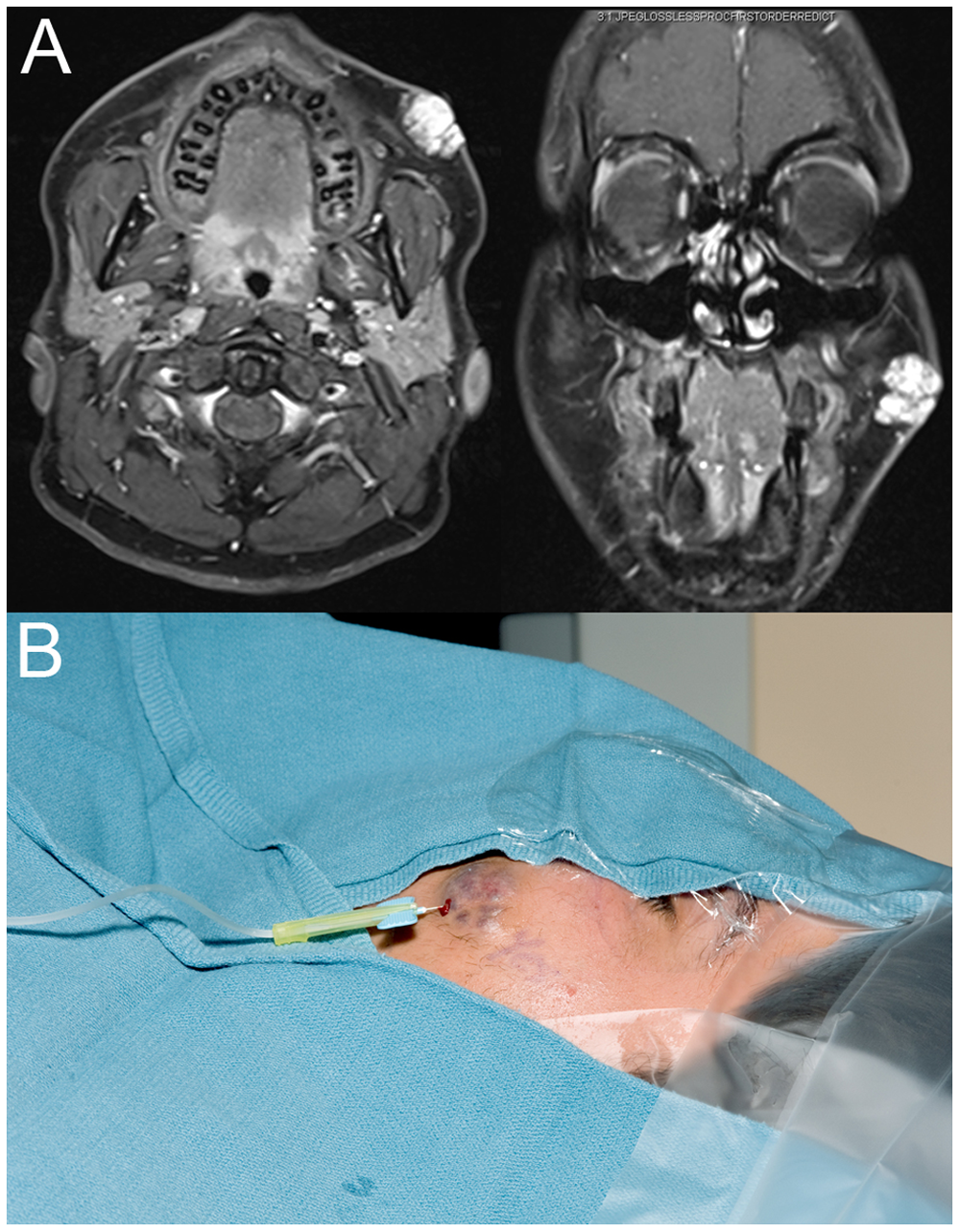
(A) Axial and coronal magnetic resonance images of localized venous malformation of the cheek. (B) Embolization with n–butyl cyanoacrylate glue in the interventional radiology suite.
Materials and Methods
Seattle Children’s Hospital (SCH) institutional review board approval was obtained prior to study initiation. The VM study cohort was retrospectively identified in the vascular anomaly quality improvement database between 2000 and January 2012. Only head and neck VMs based on clinical exam and imaging studies were included. Data collected included patient demographics, VM location, treatment type (definitive, staged/partial), total number and type of interventions, and treatment outcome. The VM patients excluded were those with non–head and neck VMs and slow-flow vascular lesions with an unclear diagnosis ( Figure 2 ). The study cohort was divided into observed patients and those actively treated. The treatment group was divided into treatment with or without preoperative n-BCA glue embolization. A secondary analysis was done on VMs that underwent treatment without preoperative n-BCA glue embolization and to determine if n-BCA glue embolization could have been applied to a larger population of patients. This was done after 2 VM patients previously treated by conventional methods were successfully treated with preoperative n-BCA glue embolization. Potential candidacy for VM treatment with the GES procedure was made through analysis of VM location (lip, tongue, face, parotid) in relation to important motor nerves at risk for injury, presence in a morbid site for sclerotherapy, resection or secondary reconstruction, and VMs with intracranial/extracranial vascular connections.
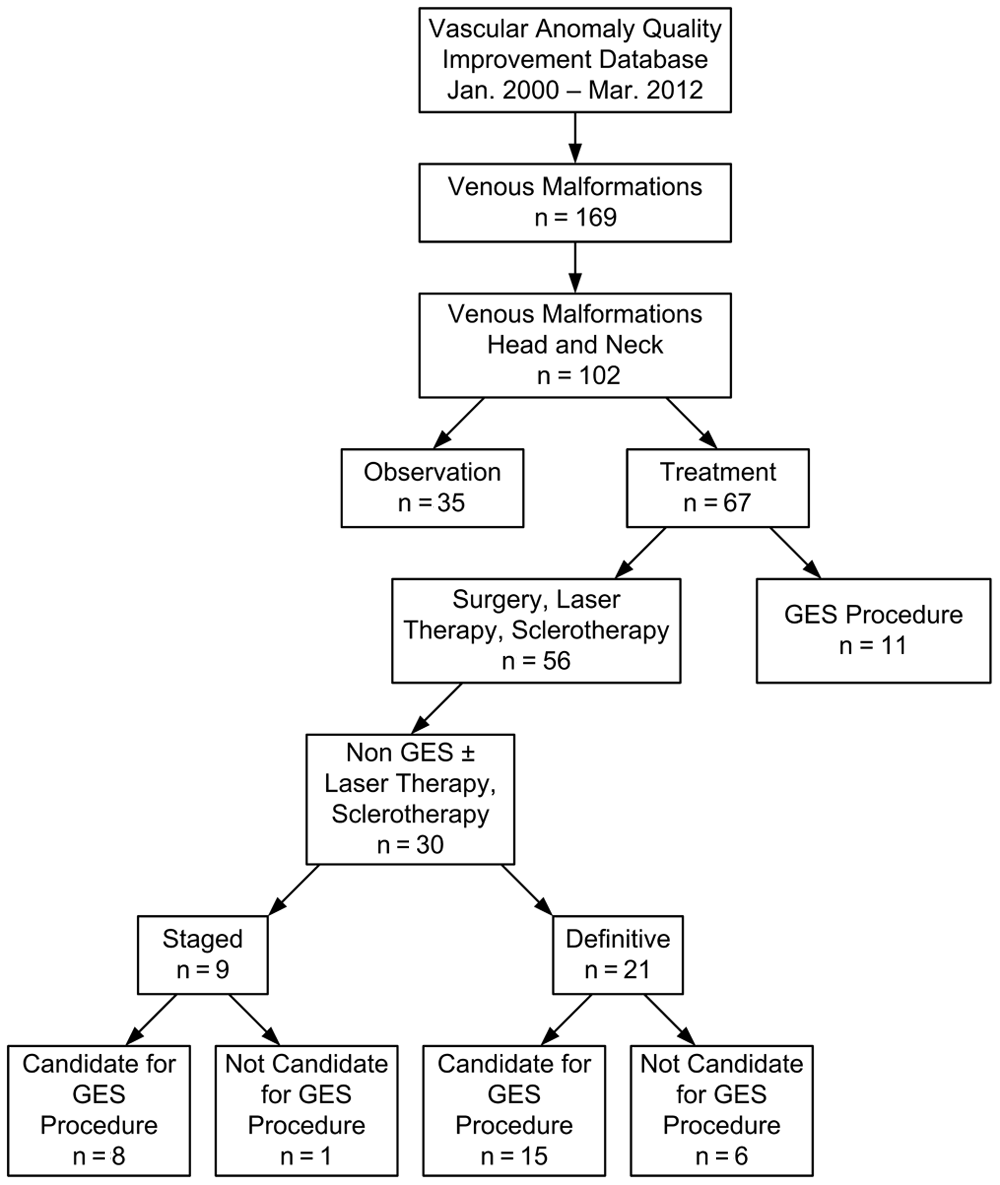
Study design and results from vascular anomaly improvement database from January 2000 to March 2012. This flow diagram illustrates the patient cohorts used in this study. The boxes after “Non-GES ± Laser or Sclerotherapy” outline pre–GES-treated patients and their potential candidacy for the GES procedure. GES, glue embolization and surgery.
Preoperative Embolization with n-BCA Liquid Embolic Glue
Patients underwent n-BCA liquid glue (Codman & Shurtleff and Johnson & Johnson) embolization, by SCH interventional radiologists (B.V.G. and N.J.V.), prior to surgical resection. Preliminary sonographic images of each corresponding VM were obtained and stored for archival purposes. With real-time sonographic guidance, 21- to 25-gauge needles were used to percutaneously puncture and access the VM to the point in which blood was identified. This was followed by a venographic contrast injection (Optiray 320; Mallinckrodt, Hazelwood, Missouri) to delineate the flow pattern and margins of the VM. The n-BCA glue was prepared using an ethiodized oil (included in the package) to form the liquid embolic mixture. The ethiodized oil served as a radio-opaque contrast agent to permit visualization of the liquid embolic mixture as it is injected under fluoroscopy. Subsequently, the n-BCA liquid glue embolic mixture was introduced into the VM under real-time fluoroscopic visualization. A previously described, the blank roadmap masking technique was used to monitor embolic material distribution and flow.21,22 Upon the complete filling of the VM with the liquid embolic mixture, the embolization was ceased. The needle was then removed and hemostasis achieved with manual compression ( Figure 1 ). Following n-BCA glue embolization, the patients were immediately transferred to the operating suite for subsequent surgical excision of the VM.
Results
We identified 169 VM patients, and 102 (60.1%) met inclusion criteria ( Figure 2 ). These patients’ demographic data are presented ( Table 1A ). The VMs in this cohort occurred in the following areas: lips (25; 25%), tongue/mouth (16; 16%), nose (2; 2%), ear (1; 1%), face/parotid (36; 36%), and neck/larynx (21; 21%). Demographic, VM specific, and VM treatment data for VM patients undergoing treatment are presented ( Table 1B ). Indications for treatment included cosmetic deformity, pain, and high hemorrhage risk ( Figure 3 ). A summary of active treatments given is shown ( Table 1B ). Note that the n-BCA glue embolization-surgery group (GES) underwent definitive procedures and the non-GES group had staged procedures. The GES group had primary closure of surgical sites and no neuromotor or neurosensory deficits, dysphagia, or dysarthria or VM recurrence ( Figures 4 and 5 ). The VMs treated with GES in the facial/parotid region all had facial nerve mapping and monitoring, which enabled identification of the facial nerve branches at the VM site without complete facial nerve dissection. 23 Patients in the GES group underwent half the number of procedures as the non-GES group ( Table 1B ). Mean follow-up time was approximately 10.4 months (range, 1-68 months).
Demographic and Treatment Data for Study Cohort
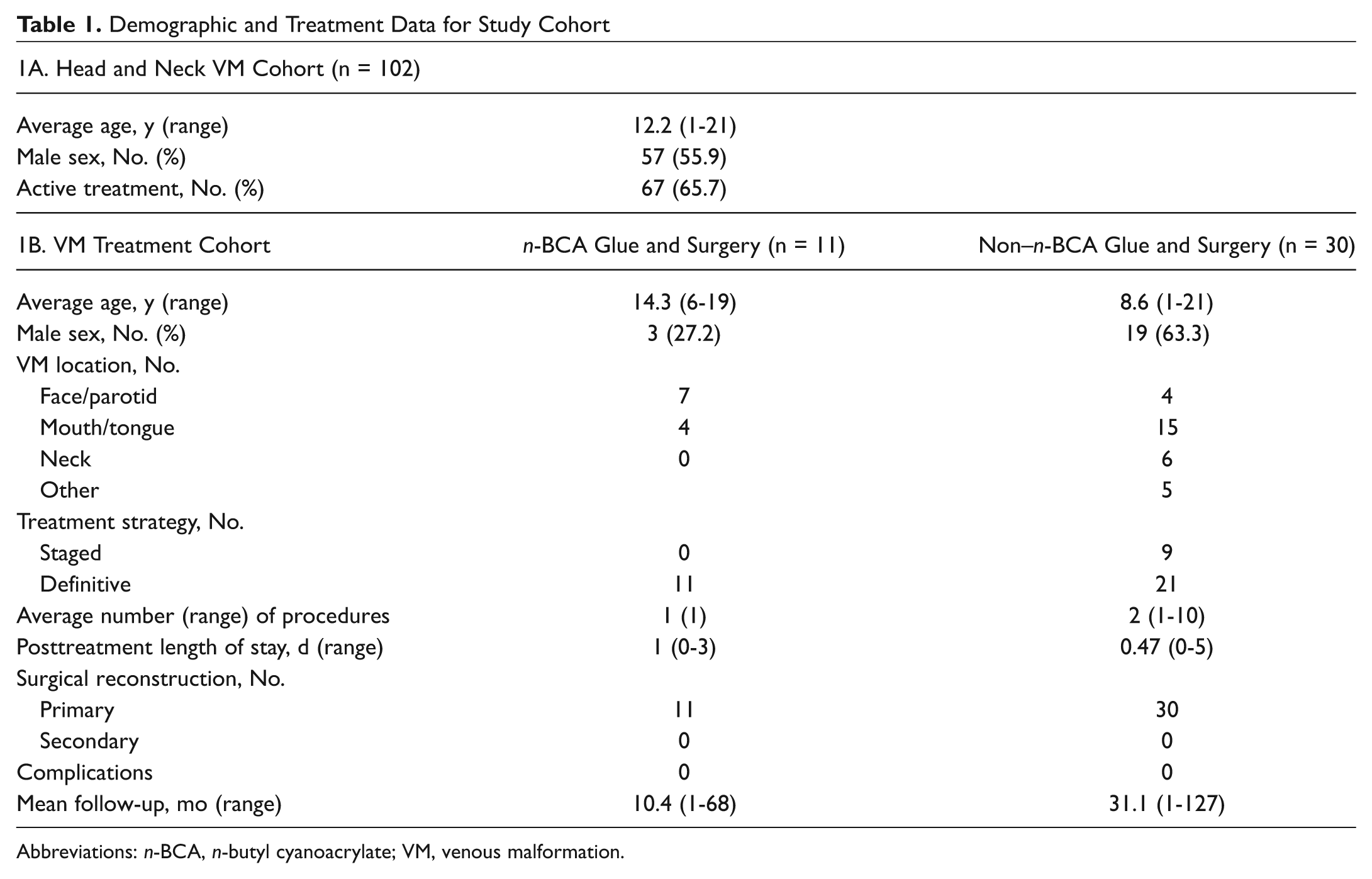
Abbreviations: n-BCA, n-butyl cyanoacrylate; VM, venous malformation.
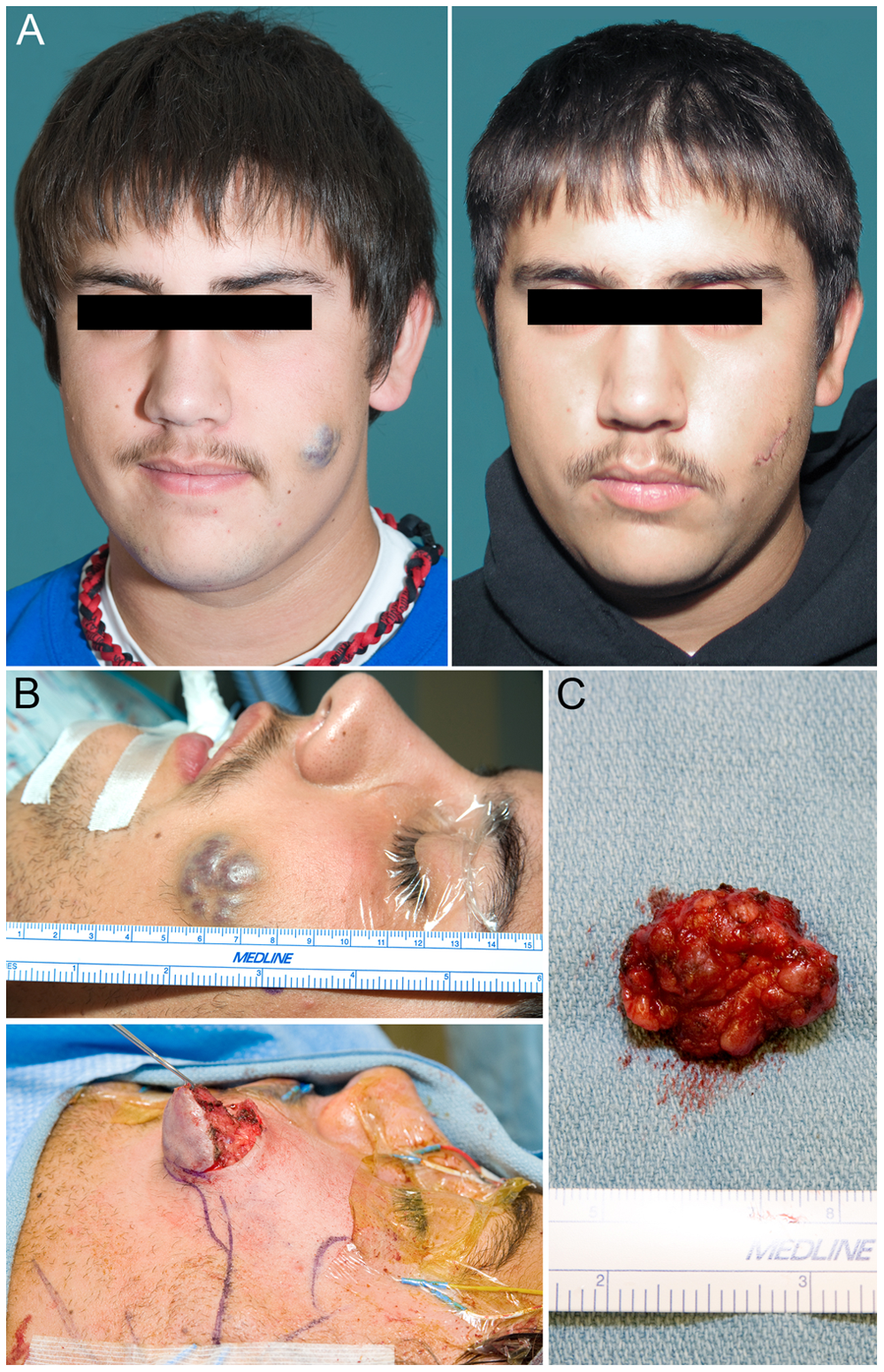
Venous malformation of the left cheek removed for recurrent pain and risk of bleeding with contact sports: (A) pre- and postoperative appearance, with normal facial nerve function after localized dissection; (B) intraoperative view with surgery through a small incision, along with facial nerve mapping and monitoring; and (C) the excised lesion without significant blood loss.
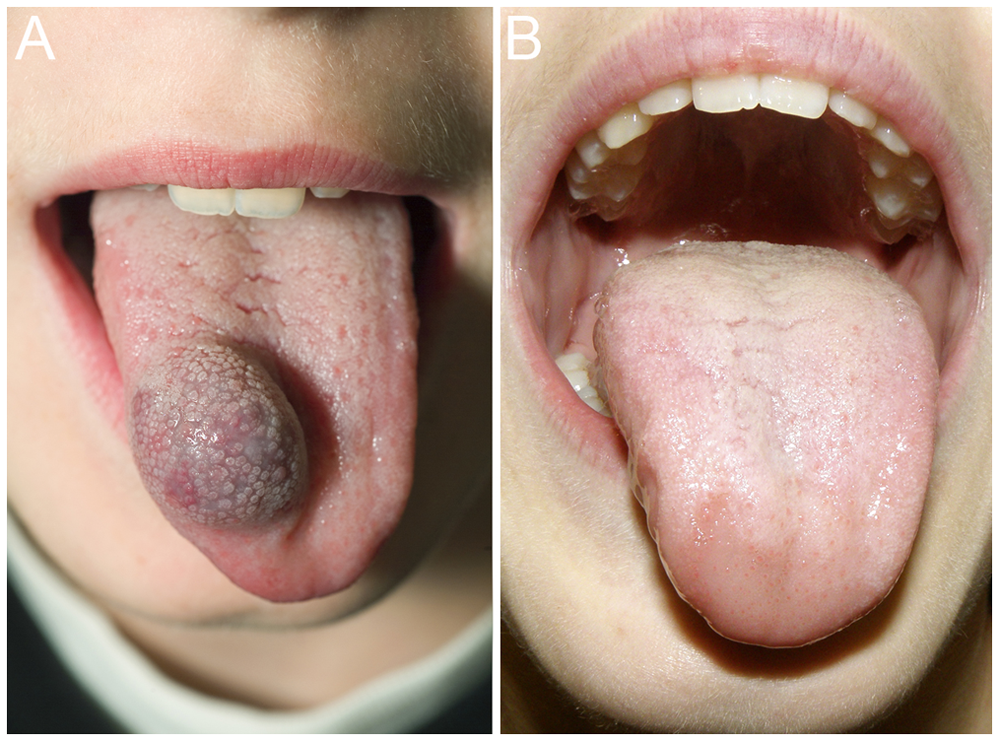
Venous malformation of the tongue with treatment indicated for high hemorrhage risk. Glue embolization and surgery procedure performed with lesion removal and primary closure. (A) Preoperative appearance and (B) postoperative appearance.

Right buccal venous malformation causing pain with chewing and risk of hemorrhage. Glue embolization and surgery procedure performed with lesion removal and primary closure. (A) Preoperative appearance, (B) postoperative appearance, and (C) intraoperative appearance with glue displacing lesion blood, lesion resection with creation of local myomucosal flaps.
Within the non-GES cohort, some VMs would have been treatable with GES, based on VM location. The VMs that were considered localized or unifocal sporadic in the head and neck were deemed potential candidates for GES. Of the 56 patients in the non-GES group, 30 (53.6%) had localized VM treated with surgical therapy alone or in conjunction with laser therapy or sclerotherapy ( Figure 2 , bottom half of diagram). The remaining 26 patients had nonsurgical invasive therapy and were not included in this reviewed cohort. Of the 30 patients, 9 underwent staged VM treatments, whereas 21 patients had attempted single-stage definitive treatment. In hindsight, 8 of 9 of the VMs treated in a staged manner would have been GES procedure candidates, whereas 15 of 21 definitive patients would have been candidates. The VM location in these 21 patients was parotid/face (4), mouth/tongue (14), neck (3), and lip (2). Of the 7 noncandidate patients, the VMs were clotted and inflamed at presentation (1), in the uvula/palate (1), primarily in the dermal layer of the chin skin (1), too large for single-stage embolization (2), or near vital structures, such as the eye (2).
Discussion
Localized VM, in children, can be treated with preoperative percutaneous embolization with n-BCA glue followed by surgical excision in a single-stage “GES procedure.” This technique appears safe and allows for complete venous malformation removal with maximal tissue and functional preservation.
Management of head and neck VM is challenging since the risk of procedural complications, posttreatment morbidity, and variable treatment response are always present. Strategies have been retrospectively described that reduce potential injury of critical head and neck structures during treatment, decrease intraoperative bleeding, improve surgical efficiency, and reduce posttreatment cosmetic deficits.14,16-18 These techniques and other serial treatments, although effective on smaller stage VMs, are controversial because they are costly and actually may introduce more treatment risk, such as significant radiation exposure.20,24 Our report also describes a new single-stage technique for VM treatment that is aimed at reduction of treatment risk while effectively eradicating localized, sporadic VM. This technique differs from described staged use of n-BCA glue embolization and surgery, reducing the chances of extralesional tissue loss or necrosis, seen in other reports. 21 This initial experience using preoperative percutaneous glue embolization followed in sequence by surgical excision of localized VM was not associated with any complications; allowed simultaneous active motor nerve monitoring, nerve dissection, and primary reconstruction; and was effective in complete VM removal, without demonstrable postoperative morbidity.
From our data, this technique is accomplished under a single anesthesia and safe for localized VM. Intraoperative blood loss was subjectively improved with minimal need for intraoperative hemostasis. Reduction in bleeding enabled excellent visualization and dissection and preservation of important structures, such as nerves and arteries. Preoperative glue embolization evacuates intralesional blood while preserving overlying tissue, allowing surgical excision through small incisions and facilitating local flap creation for primary reconstruction and closure ( Figures 3 - 5 ). To be able to perform primary reconstruction in this setting is an exciting possibility that in our experience significantly reduces postprocedure morbidity (ie, swelling, pain, mucosal loss, etc.) often seen with other treatment modalities. Review of VMs treated without glue embolization showed that the majority would have been candidates for preoperative glue embolization followed by surgical excision ( Figure 2 ). The patients who would not have been candidates for this technique had VMs that were deemed too large for single-stage therapy and were extensively entwined with critical structures, such as the eye or in areas (chin, uvula/palate) where preoperative glue embolization may not have offered any additional advantage. When glue-embolized VMs are in the parotid or near a motor nerve, surgical management with active facial nerve monitoring/mapping is essential, as this enables clear identification and preservation of individual nerve branches without the need for complete nerve dissection in localized VM. Preoperative VM glue embolization followed by surgical excision enables complete lesion removal with preservation of surrounding vital structures, but one must keep in mind there is a tissue deficit that results from this excision, and this defect must be appropriately reconstructed.
Overall, preoperative glue embolization followed by immediate surgical excision represents an innovative technique to manage localized head and neck VMs. This technique requires collaboration between interventional radiologists and surgeons, in addition to careful preoperative planning and intraoperative monitoring. Preoperative glue embolization allows the procedure to occur in sequence, ending in same-day surgical resection. This approach could potentially minimize radiation exposure to patients as compared with patients who have undergone multiple sclerotherapy sessions. 24 In addition, complete lesion removal could minimize the risk of cutaneous scarring from laser and/or injection sclerotherapy.
One of the limitations of this study is that the GES group had fewer patients than the non-GES group. This was due to the relative novelty of this technique. As a result, long-term follow-up was not possible in all patients. It would be interesting to obtain an even larger cohort to evaluate the impact of GES on operative time, intraoperative blood loss, and health care costs. Of particular interest would be a randomized controlled study comparing outcomes using this innovative technique with more traditional methods. Future studies will also determine if this technique is adaptable to larger lesions, allowing resection in a staged manner, to allow development of guidelines for patient and lesion selection.
Conclusion
Surgery has been used effectively to eradicate or minimize VMs, but the risk of bleeding, residual cosmetic and functional deficits, and recurrence presents a management challenge. Our results demonstrate that preoperative percutaneous embolization of localized VM with n-BCA glue followed by surgical resection, the “GES procedure,” is safe and allows for complete VM removal. Furthermore, this innovative technique to treat VMs has the potential to reduce the number of operative interventions, while minimizing radiation exposure required as well as reducing the costs and morbidity with treating such lesions. The GES procedure has become our preferred method of treating localized VMs.
Author Contributions
Disclosures
Footnotes
Acknowledgements
We thank Eden Palmer for generation and editing of clinical photos and manuscript figures.
No sponsorships or competing interests have been disclosed for this article.
This article was presented at the 19th International Workshop on Vascular Anomalies; June 16-19, 2012; Malmö, Sweden.