
Abstract
Objectives
Oral tongue cancer may have a distinct epidemiological profile from other mucosal neoplasms of the oral cavity. We sought to further define the demographic characteristics associated with oral tongue cancer to determine if unique characteristics exist compared with other oral cavity cancers.
Study Design
Cross-sectional analysis using cross-tabulations and multivariate regression modeling.
Setting
The Maryland Health Service Cost Review Commission database.
Subjects and Methods
Discharge data from a state database were queried to perform a cross-sectional analysis of oral cancer cases treated surgically from 1990 to 2009.
Results
A total of 1688 oral cancer cases comprised the study population, with 719 (42.6%) of cases involving the oral tongue. Tongue cancer comprised 31.6% of oral cancers in black patients and 44.1% of oral cancer in white patients (P = .011). Racial disparities in oral tongue cancer were identified for age at diagnosis, with significantly fewer black patients younger than 40 years (3.8%) compared with whites (11.3%; P = .006). After controlling for all other variables, oral tongue cancer patients were significantly less likely to be older than 40 years (odds ratio [OR], 0.40; P < .001), black (OR, 0.53; P = .001), have Medicare payor status (OR, 0.55; P = .002), and advanced comorbidity (OR, 0.22; P < .001), in contrast to other oral cancer subsites.
Conclusion
The racial and socioeconomic qualities of oral tongue cancer patients differ significantly from other oral cancers. This younger, healthier subgroup of oral cancer patients demonstrates a distinct population at risk for cancer of the oral tongue.
The epidemiological heterogeneity of head and neck cancer is becoming increasingly recognized as having clinical relevance. Although the incidence of head and neck cancer has historically been observed to increase with increasing age, recently younger populations have been identified who appear to have an increased incidence of disease. The first consists of high-risk human papillomavirus (HPV)–associated oropharyngeal cancer patients who do not present with the conventional risk factors of tobacco and alcohol exposure; are primarily white, male, and younger than 50 years; and appear to have an improved prognosis when compared with HPV-negative oropharyngeal cancers.1,2 A second emerging group is a subset of oral tongue cancer patients who also demonstrate an increasing incidence rate unrelated to HPV infection.3,4 Demographically, these patients are young, white females younger than 50 years. Although both HPV-associated oropharyngeal cancer and oral tongue cancer patients tend to be younger than the traditional head and neck patient, they appear to differ in both etiology and prognosis. In contrast to HPV-associated oropharyngeal cancer patients, oral tongue cancer has no association with high-risk HPV infection, and younger oral tongue cancer patients do not appear to have a survival advantage compared with oral tongue cancer patients older than 50 years.3-6 Using a statewide database, we sought to further define the demographic characteristics associated with oral tongue cancer to determine if unique characteristics exist compared with other oral cavity cancers.
Methods
A cross-sectional analysis of patients with a diagnosis of oral cancer was performed using hospital discharge data from nonfederal acute care hospitals in Maryland collected by the Maryland Health Service Cost Review Commission (HSCRC). The HSCRC database provides information regarding the index hospital admission (surgery) and is limited to 30 days of follow-up. Adult patients (≥18 years of age) who underwent an ablative procedure for a malignant oral cavity neoplasm in Maryland between January 1, 1990, and July 1, 2009, comprised the study population. The International Classification of Diseases, 9th Revision (ICD-9) codes for malignant neoplasm of the lip (141.0, 140.1, 140.3,140.4, 140.6, 140.8, 140.9), oral tongue (141.1, 141.2, 141.3, 141.4, 141.9), gum (143.0, 143.1, 143.8, 143.9), floor of mouth (144.0, 144.1, 144.8, 144.9), and other unspecified parts of mouth (145.0, 145.1, 145.2, 145.5, 145.6, 154.8, 154.9, and 170.1) were used for sorting. All cell types were included. Surgical procedures included in this analysis were limited to ablative procedures: destruction of tongue lesion (25.1), partial glossectomy (25.2), complete glossectomy (25.3) or radical glossectomy (25.4), or partial or total mandibulectomy (76.31, 76.41, 76.42), with or without neck dissection (40.40, 40.41, 40.42, 40.3).
Secondary independent variables included were age, sex, race, All Patient Refined Diagnosis Related Groups (APR-DRG) case complexity score (1-4), APR-DRG mortality risk score (1-4), length of stay, intensive care unit (ICU) days, other specialty unit care days, payor source (commercial, health maintenance organization [HMO], Medicare, Medicaid, or self-pay), procedure, nature of admission (emergent/urgent or other), readmission, inpatient death, and hospital type (university, community teaching, or community). The APR-DRG case complexity score reflects the clinical severity of illness related to the extent of physiologic decompensation or loss of organ function experienced by the patient for either the primary diagnosis or comorbidities, whereas the APR-DRG mortality risk score reflects the likelihood of dying. Both scoring systems incorporate the impact and interaction of multiple secondary diagnoses. A community teaching hospital was defined as a nonuniversity hospital with a residency program in otolaryngology–head and neck surgery or oral surgery. Procedures were categorized by severity as minor (excision/destruction of lesion and partial glossectomy, with or without neck dissection) and major (complete or radical glossectomy or mandibulectomy, with or without neck dissection). American Joint Commission on Cancer (AJCC) tumor stage, tumor grade, histological subtype, and outcome beyond 30 days were not available from the HSCRC database.
Data were analyzed using Stata 12 (StataCorp, College Station, Texas). Associations between variables were analyzed using χ2 tests and multivariate logistic regression. Age categories were created based on the results of loess smoothed regression analysis. Collinearity was checked by performing a multiple regression analysis and calculating the variance inflation factors (VIF) and removing variables with a VIF greater than 10.0, which suggests collinearity. Variables that were hypothesized to have predictive value as well as those that were significant in bivariate analysis were entered into the regression models. Multiple logistic regression was used to identify variables that were significantly associated with primary site and race using a stepwise backward selection approach. Odds ratios (ORs) are expressed relative to a reference baseline category. This protocol was reviewed and approved by the Johns Hopkins Medical Institutions Institutional Review Board.
Results
A total 1688 cases met study criteria ( Table 1 ). The mean age was 61.2 years (range, 20-101 years). The majority of patients were male (59.7%) and white (79.9%). The oral tongue was the most common subsite for oral cancer (42.6%), followed by the floor of mouth (27.7%), other unspecified subsite (18.1%), gum (9.2%), and lip (2.4%). Patients with oral tongue cancer were significantly younger than patients with cancer of other oral subsites. Specifically, there was a higher incidence of oral tongue cancer in patients younger than 40 years compared with other oral cavity subsites. Oral tongue cancer patients had lower APR-DRG case complexity scores and lower APR-DRG mortality risk scores and were more likely to have commercial insurance and more likely to receive treatment at a community hospital.
Demographic Characteristics of Oral Cancer Patients
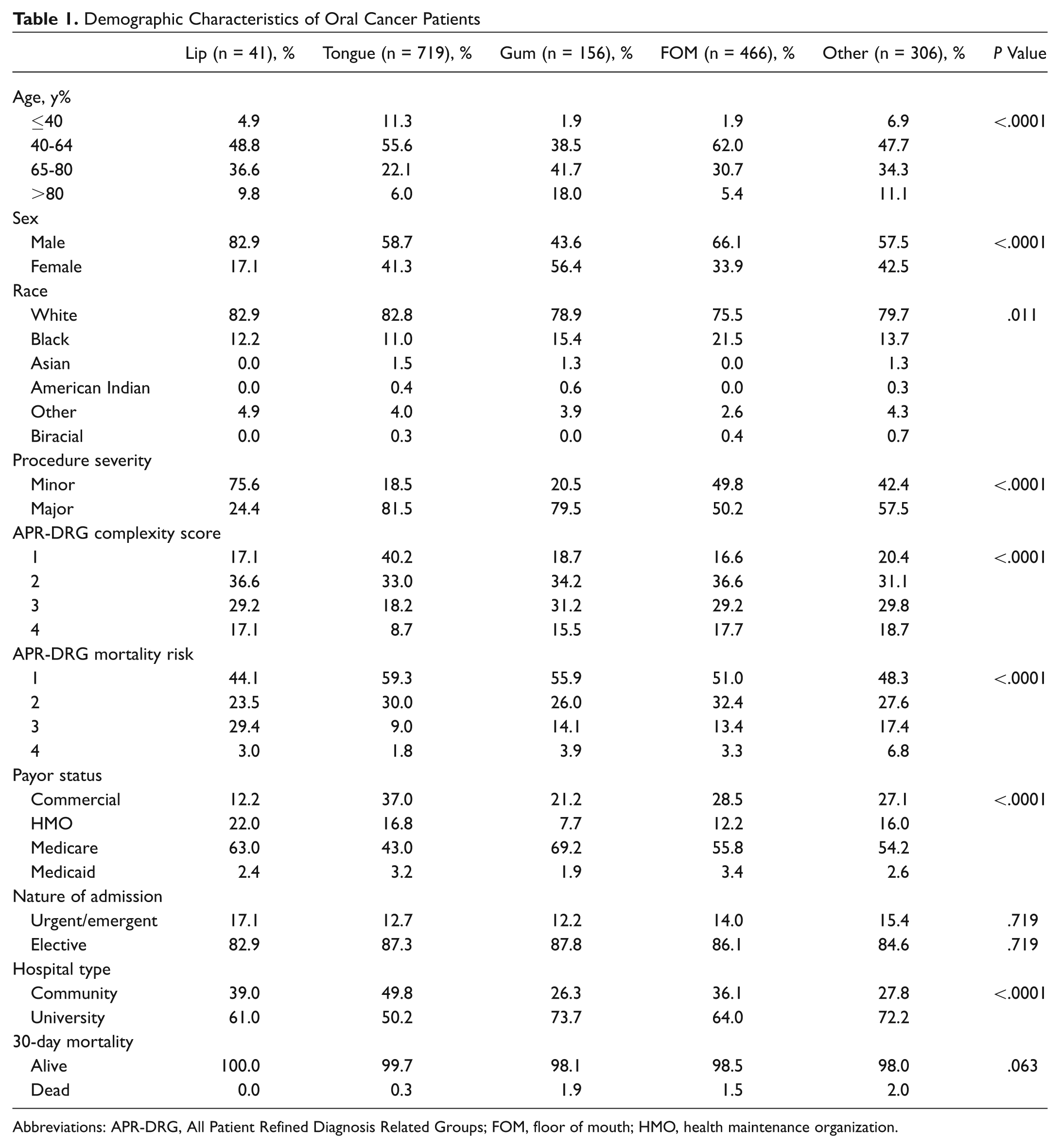
Abbreviations: APR-DRG, All Patient Refined Diagnosis Related Groups; FOM, floor of mouth; HMO, health maintenance organization.
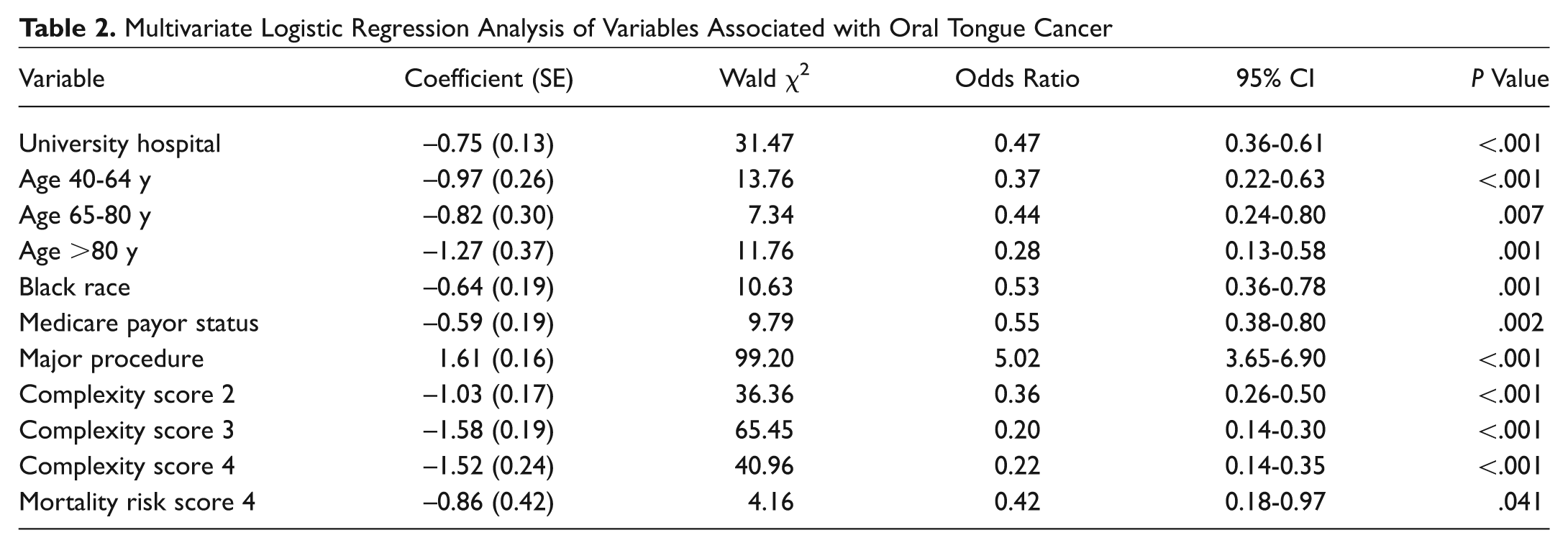
Multivariate regression analysis of variables associated with a diagnosis of oral tongue cancer is shown in Table 2 . Compared with other oral cavity sites, patients with oral tongue cancer were less likely to be black, more likely to be younger than 40 years, and less likely to have Medicare insurance, have advanced comorbidity, and receive care at a university hospital but were significantly more likely to require major surgical procedures.
Multivariate Logistic Regression Analysis of Variables Associated with Oral Tongue Cancer
Discussion
This analysis describes distinct epidemiologic characteristics of oral tongue cancer patients compared with other oral cavity cancer subsites. We found that patients with oral tongue cancer were more likely to be younger than 40 years, were less likely to be black, had lower case complexity scores, but were more likely to require major surgical procedures for treatment. These data reinforce the evidence from prior studies that patients with oral tongue cancer have distinct epidemiologic differences compared with patients with cancer of other oral cavity subsites.
Although a reduction in tobacco usage is likely a driving force behind declining oral cancer cases overall,1,7 several epidemiologic studies have recognized a rising incidence of cancers arising from the oral tongue subsite. Shiboski et al 4 examined trends in 2262 patients with squamous cell carcinoma of the oral cavity and 1251 cases of the pharynx from the Surveillance, Epidemiology and End Results database (SEER). Subsite analysis demonstrated a steady increase in oral tongue, tonsil, and tongue base squamous cell cancers, specifically in a younger white subpopulation aged 20 to 44 years. Patel et al 3 similarly performed trend analyses in the SEER database and demonstrated a rising incidence of oral tongue squamous cell carcinoma in young patients aged 18 to 44 years, with a greater increase in annual incidence for white women than for white men. We now recognize infection with high-risk HPV strains as a major etiologic factor for tonsillar and base-of-tongue cancers 2 ; however, high rates of HPV infection have never been demonstrated in the oral cavity and are an unlikely explanation for the increased incidence in oral tongue cancer in younger patients.1,6,8 In this study, we found that oral tongue cancer patients were younger than other patients with tumors of other oral cancer sites and were less likely to be black: the large majority of nonblack patients were white in this study. The HSCRC database does not provide information on tobacco or alcohol use, so we cannot evaluate the role of substance abuse in explaining this trend, but it is unlikely that this trend is related to an increase in tobacco or alcohol use.
Several studies have focused specifically on the characteristics of head and neck cancer in patients who are nonsmokers and nondrinkers and have identified an increase in oral tongue cancers in this low-risk subgroup.9-11 Wiseman et al 12 studied a small cohort of 40 patients who had never smoked and never drank alcohol: a small proportion of 1648 head and neck cancer patients studied. They found that 78% of the primary tumors in never-smokers were located in the oral cavity, predominantly involving the oral tongue. In a larger series of 125 cases of head and neck cancer in patients who did not smoke or use alcohol, de Boer et al 13 also found that 73% of cancers arose from the oral cavity, with the remainder of primary tumors arising in the oropharynx. Harris et al 11 evaluated a cohort of never-smokers and never-drinkers younger than 40 years and found that compared with patients with a history of tobacco and alcohol use in the same age range, young never-smokers and never-drinkers were more likely to have oral tongue cancer.
Despite a decreased incidence of traditional risk factors (tobacco and alcohol abuse) reported in the literature, and in our study a decreased incidence of comorbidity, no survival benefit has been clearly demonstrated to date for younger oral tongue cancer patients when compared with other oral cavity subsites or older patients with oral tongue cancer.3,14-21 Historically, young patients with oral tongue cancer were believed to have a poorer prognosis, 22 although more recent studies have demonstrated that with equivalent treatment, outcomes for young patients are equivalent to those of older patients with oral tongue cancer.17,18 We found that oral tongue cancer patients were less likely to have advanced comorbidity and more likely to have commercial insurance, suggesting a younger, healthier population with greater access to health care services, but more commonly underwent major surgical procedures. These findings suggest several possibilities: that better preoperative health status allowed for more extensive surgical procedures in this subset; that treatment is more aggressive in younger, healthier patients; or that young patients with oral tongue cancer presented with more advanced disease, which may reflect a lack of clinical awareness of cancer risk in younger patients and a need for greater educational efforts, diagnostic delay in younger patients, or more aggressive tumor biology in this subpopulation. The HSCRC database does not contain tumor staging information, and so the effect of stage cannot be determined; however, multivariate analysis controlling for the effects of age, comorbidity, and insurance status still showed a significant increased likelihood of major surgical procedures for oral tongue cancer patients, suggesting either that stage is more advanced in this population or that treatment is more aggressive for reasons that are not captured in administrative data.
There are several limitations to the use of hospital discharge data that may influence our findings. Although case complexity and mortality risk scores were used for risk adjustment, the ability to adequately control for case mix is limited when discharge diagnoses from administrative databases are used, which is the case in almost all studies investigating volume and outcome associations to date, including the present study. The Maryland HSCRC database provides no follow-up data beyond the index admission, is limited to a 30-day postoperative window, and contains no information on stage of disease, grade, subtype, long-term outcomes, or survival. The HSCRC database does not contain information regarding risk factors such as tobacco or alcohol use and the use of previous surgical procedures or chemotherapy, and the effect of treatment on survival cannot be estimated. Because the HSCRC is an inpatient database, patients who undergo diagnostic procedures only will not be captured, nor will patients who are treated nonoperatively. Postoperative complications may not be apparent at the time of discharge, and as a result, the incidence of complications may be underreported. Finally, surgery performed on an outpatient basis is not captured in this inpatient database limited to hospital admissions.
Despite these limitations, these data demonstrate some distinct epidemiologic features of oral tongue cancer that suggest several hypotheses: that oral cancer in younger patients may present differently, be treated differently, or may represent a distinct biologic entity. Patients with oral tongue cancer are more likely to be younger than 40 years, less likely to be black, less likely to have advanced comorbidity, more likely to have commercial insurance, and more likely to undergo more extensive surgical procedures compared with patients with cancer involving other oral cavity subsites. These data suggest a need for further investigation to identify the reasons for the disparities seen in oral tongue cancer patients compared with other oral cavity cancer sites to determine whether diagnostic, treatment, or biological differences underlie these observed epidemiologic differences.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.