
Abstract
Objective
To describe the epidemiology and determine the clinicopathologic predictors of recurrence and survival in patients with head and neck mucoepidermoid carcinoma (MEC).
Study Design
Case series with chart review.
Setting
Tertiary care hospital.
Subjects and Methods
The medical records of 101 patients who underwent surgical treatment at the University of Michigan for head and neck MEC between 1985 and 2010 were reviewed. Main outcome measures were disease-free survival (DFS), disease-specific survival (DSS), and overall survival. Clinicopathologic parameters evaluated were age, sex, subsite, histological grade, adjuvant therapy, T stage, nodal status with/without extracapsular spread, and margin status.
Results
Of the 101 patients, 38 parotid, 33 palate, 17 oral, 8 submandibular/sublingual, 4 orbital, and 1 parapharyngeal carcinomas were identified. All patients underwent surgical resection, 23 had postoperative radiation, and 2 had postoperative chemoradiation. The 5-year OS and DSS was 79% and 95% with a median follow-up of 72 and 45 months, respectively. Five-year DFS was 76%. On univariate analysis, histological grade was a statistically significant predictor of disease-free survival (P = .001) and overall survival (P = .04). Positive nodal status was a significant predictor of DSS (P = .004). There was no statistically significant difference in DFS, DSS, or OS based on sex, age, anatomic subsite, T stage, adjuvant therapy, and margin status.
Conclusion
Advanced histological grade and positive nodal status are the strongest independent predictors of prognosis in head and neck MEC patients. Further studies into the molecular biology of MEC that may account for such clinicopathological features are currently underway.
Introduction
Mucoepidermoid carcinoma (MEC) is the most common malignancy of the salivary glands, representing 30% to 40% of all major salivary gland malignancies 1 and up to 50% of parotid gland malignancies. 2 MEC is comprised of 3 different histological cell types in varying proportions: mucous cells, undifferentiated small cells (intermediate cells), and epidermoid (squamoid) cells. Low-grade tumors typically are cystic and have more mucous cells, while high-grade lesions tend to be solid and have a more epidermoid cell component ( Figure 1 ). 3

Histological classification of mucoepidermoid carcinoma (MEC) within our cohort. Low-grade (Panel A) typically consists mainly of mucin-secreting cells. Intermediate-grade (Panel B) is comprised of both mucin and epithelial cells. High-grade (Panel C) has mainly an epithelial cell component.
The clinicopathologic behavior of MEC is highly variable, ranging from slow-growing indolent tumors to locally aggressive and highly metastatic carcinomas. In an attempt to gain better insight into its highly variable behavior, a variety of prognostic factors have been studied to predict aggressive tumor behavior. Histologic grading of MEC has been shown to correlate strongly with clinical behavior, although reproducibility and consistency associated with the various grading systems continues to be problematic.4-6 Other clinicopathologic parameters such as age, sex, tumor site, stage, TNM status, extracapsular spread (ECS), adjuvant therapy, and margin status have been shown to have predictive value in survival, although it has been suggested that the most prognostically relevant of these are histological tumor grade and clinical stage.7 -11
The objectives of this study were to describe the epidemiology of head and neck MEC treated at a single tertiary hospital as well as to determine the clinicopathologic predictors of recurrence and survival in this patient population.
Materials and Methods
Study Population
Using the University of Michigan Department of Pathology laboratory information system, 153 patients were identified as having MEC between 1985 and 2010. Of the 153 patients originally identified, 113 met the following inclusion criteria: a primary MEC involving the head and neck that was treated (either by surgery alone, surgery and radiation [RT], or surgery, radiation, and chemotherapy [CRT]) at the University of Michigan. Slides from all cases were reviewed by a head and neck pathologist (JBM) to confirm the diagnoses. Twelve cases that were originally diagnosed as MEC (7 high-grade, 3 intermediate-grade, 1 low-grade, and 1 unknown) were reclassified as salivary duct carcinomas. These cases were eliminated from our analysis to give us a total of 101 patients analyzed. Using retrospective chart review, data collected included age, gender, ethnicity, tumor site, histological grade, stage, treatment type, T stage, nodal status with/without extracapsular spread, primary tumor margins, current disease status, and median follow-up. Archived pathology slides were available for all 113 patients. Indications for adjuvant RT generally included positive margins, positive nodal metastasis, ECS, perineural invasion (PNI), and advanced T stage (T3, T4).7,12,13
Approval was obtained by the Institutional Review Boards of the University of Michigan Medical School prior to conducting this study (IRB No. HUM00051553).
Tumor Staging and Histological Classification
Patients were staged using clinical and radiographic findings according to the American Joint Committee on Cancer (AJCC) classification system for salivary gland carcinomas. 14 Tumors were upstaged to a T4 based on any cranial nerve or bone involvement. Initial T stage was not available for those patients presenting with recurrent or residual tumors (n = 13), as well as for 4 patients presenting to University of Michigan for initial tumor evaluation.
Histological grading was performed by a head and neck pathologist (who was blinded to the clinical outcome) using the Armed Forces Institute of Pathology (AFIP) grading system. This system evaluates the following histologic parameters with weighted point scales in parentheses: intracystic component <20% (+2), neural invasion (+2), necrosis (+3), ≥4 mitoses/10 hpf (+3), and anaplasia (+4). Scores are added resulting in a range from 0 to 14. A score of 0 to 4 represents a low-grade tumor; 5-6 intermediate-grade; 7+ high-grade. 15
Statistical Analysis
The outcomes of interest were disease-free survival (DFS), overall survival (OS), and disease-specific survival (DSS). The start point for survival estimates was defined as the date of diagnosis. A DFS event was defined as a pathologically confirmed recurrence; an OS event was defined as death from any cause; a DSS event was defined as a death from cancer; deaths from other causes were censored at the date of death. DFS, OS, and DSS curves were estimated by the Kaplan-Meier method. Univariate and multivariate Cox regression models were used to assess the association between DFS, OS, and DSS and age, gender, disease subsite, tumor grade (low, intermediate, high), adjuvant therapy, T stage, nodal status, and margin status.
Results
Clinical and Pathologic Characteristics
Patient and tumor characteristics of the entire cohort are shown in Table 1 . There were 53 women and 48 men, with a median age at diagnosis of 49.8 (range, 7-82). Eighty-eight patients (87.1%) presented to our institution who were previously untreated or had residual tumors, while 13 patients (12.9%) presented with recurrent tumors. All head and neck sites were included, with the parotid gland being the most common primary tumor site (38/101; 37.6%). Original histological grade consisted of 64 of 101 (63.4%) low-grade, 24 of 101 (23.8%) intermediate-grade, and 12 of 101 (11.9%) high-grade tumors. For 1 patient, histological grade could not be determined definitively. A predominance of males compared to females was seen in the high-grade group (9:3), which was not noted in the intermediate-grade (10:14) and low-grade (28:36) cohorts. The majority of patients presented without regional neck metastases (92/101; 91.1%). Positive nodal disease was directly associated with higher histological grade being identified in 4.7% of the patients in the low-grade group, 12.5% in the intermediate-grade group, and 25% in the high-grade group. A fairly even distribution of T1/T2 (42.2%) and more advanced T3/T4 stage tumors (46.9%) was seen in the low-grade group. The majority of the intermediate and high-grade cohorts were comprised of advanced T stage (62.5% and 41.6%, respectively) as shown in Table 2 .
Clinical/pathologic characteristics in MEC retrospective cohort.
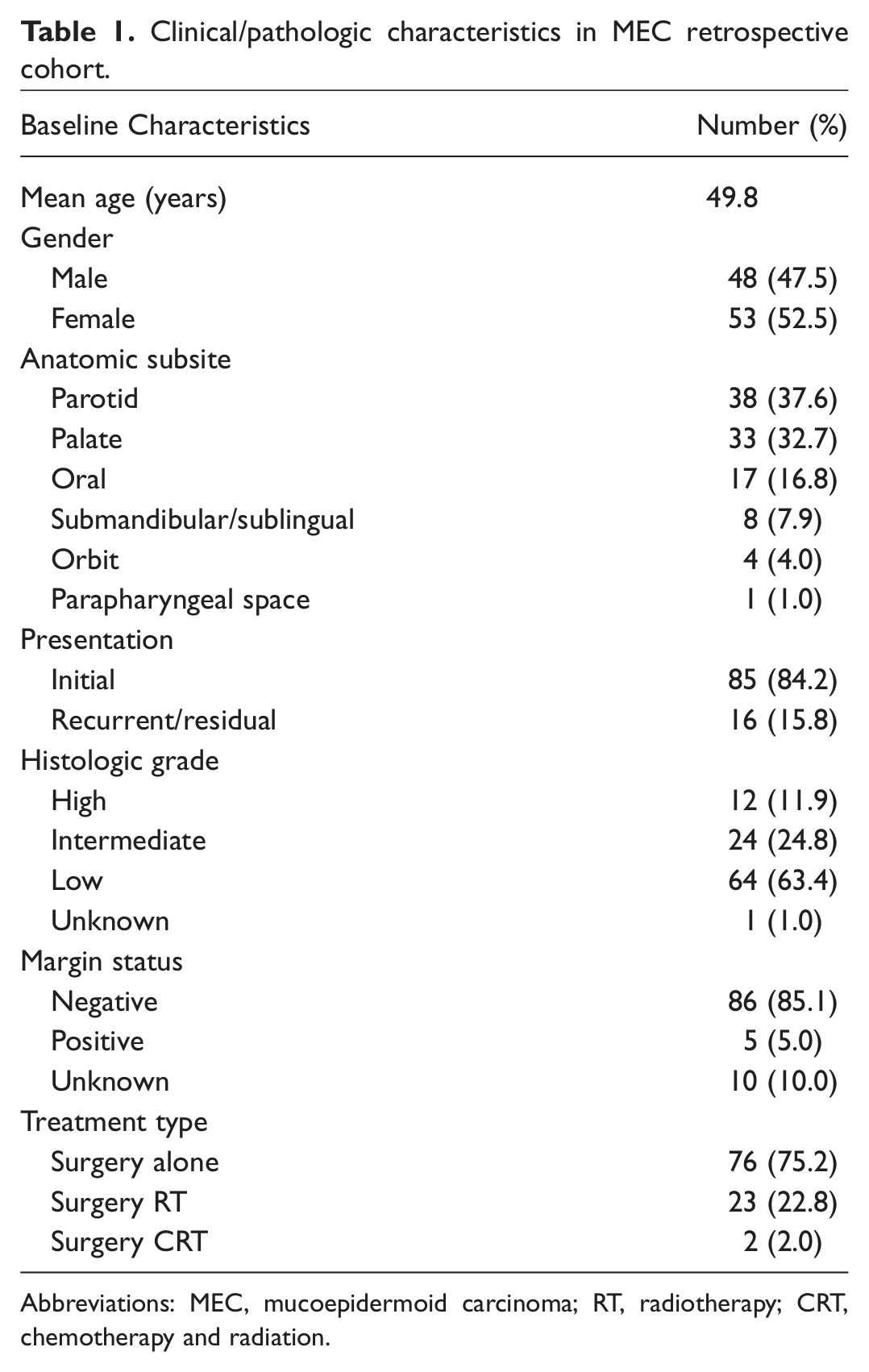
Abbreviations: MEC, mucoepidermoid carcinoma; RT, radiotherapy; CRT, chemotherapy and radiation.
Tumor and nodal characteristics based on histological grade.
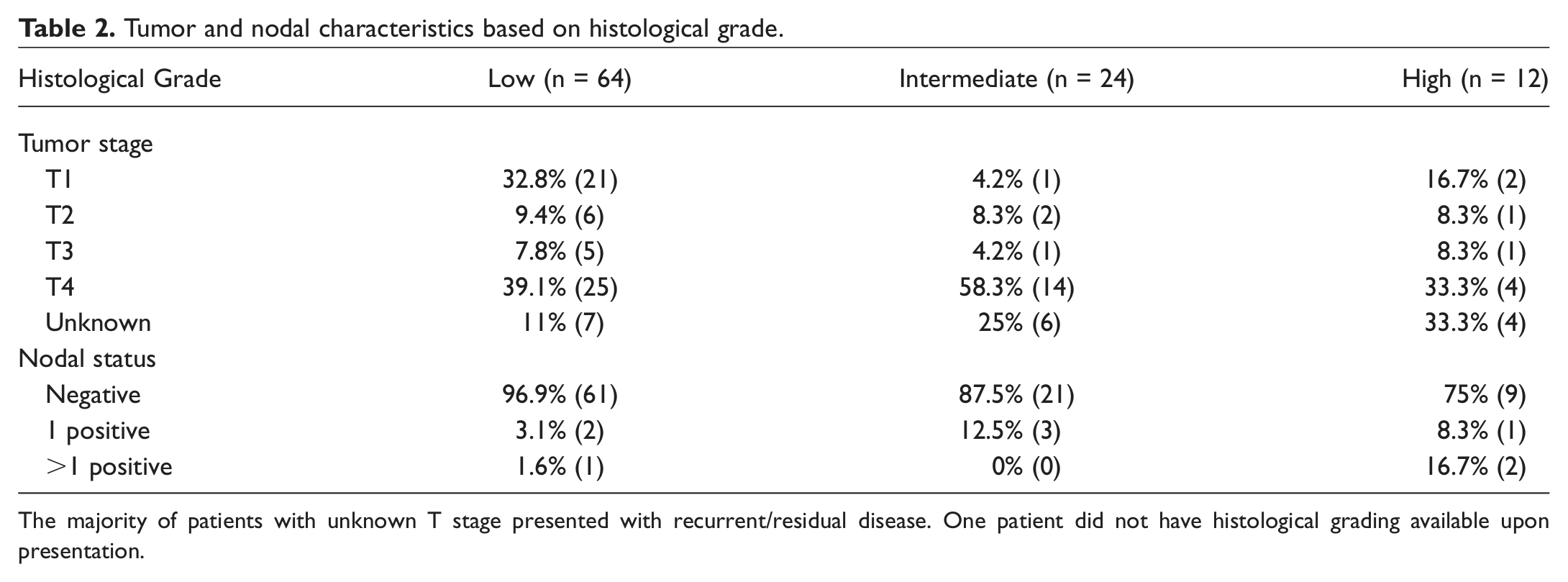
The majority of patients with unknown T stage presented with recurrent/residual disease. One patient did not have histological grading available upon presentation.
Tumor Recurrence and Clinical Outcomes
Clinical and pathologic characteristics of all patients with disease recurrence (either local [L], regional [R], local and regional [LR], or distant metastasis [DM]) are shown in Table 3 . There were 12 (11.9%) patients who experienced a recurrence following treatment at our institution: 5 of which were local recurrences, 4 regional, 2 local and regional, and 1 distant metastasis. Seven of 12 (58.3%) originally underwent resection of their disease, 5 of 12 (41.7%) underwent resection plus radiation, and 8 of 12 (66.7%) underwent unilateral/bilateral neck dissection (selective, modified, or radical) at the time of presentation. Three of 12 (25%) of the recurrences were low-grade tumors, 4 of 12 (33.3%) were intermediate, and 5 of 12 (41.7%) were of high histological grade. Four of the 12 (33.3%) patients who experienced a recurrence had positive nodal disease. Six of the 12 patients (50%) initially presented to our institution with recurrent disease and developed another recurrence after undergoing successful treatment at our institution. Five of 12 patients who developed a recurrence died of their disease—1 patient with a low-grade tumor, 2 patients with intermediate tumors, and 2 patients with high-grade primary tumors. Three were without nodal disease at presentation. Three of the 5 that died of their disease originally presented to our institution with recurrent disease. One patient is currently alive with intermediate-grade, nodal positive disease.
Clinical and pathologic characteristics of all patients who developed disease recurrence (L, R, LR, or DM) while undergoing treatment/surveillance at University of Michigan.
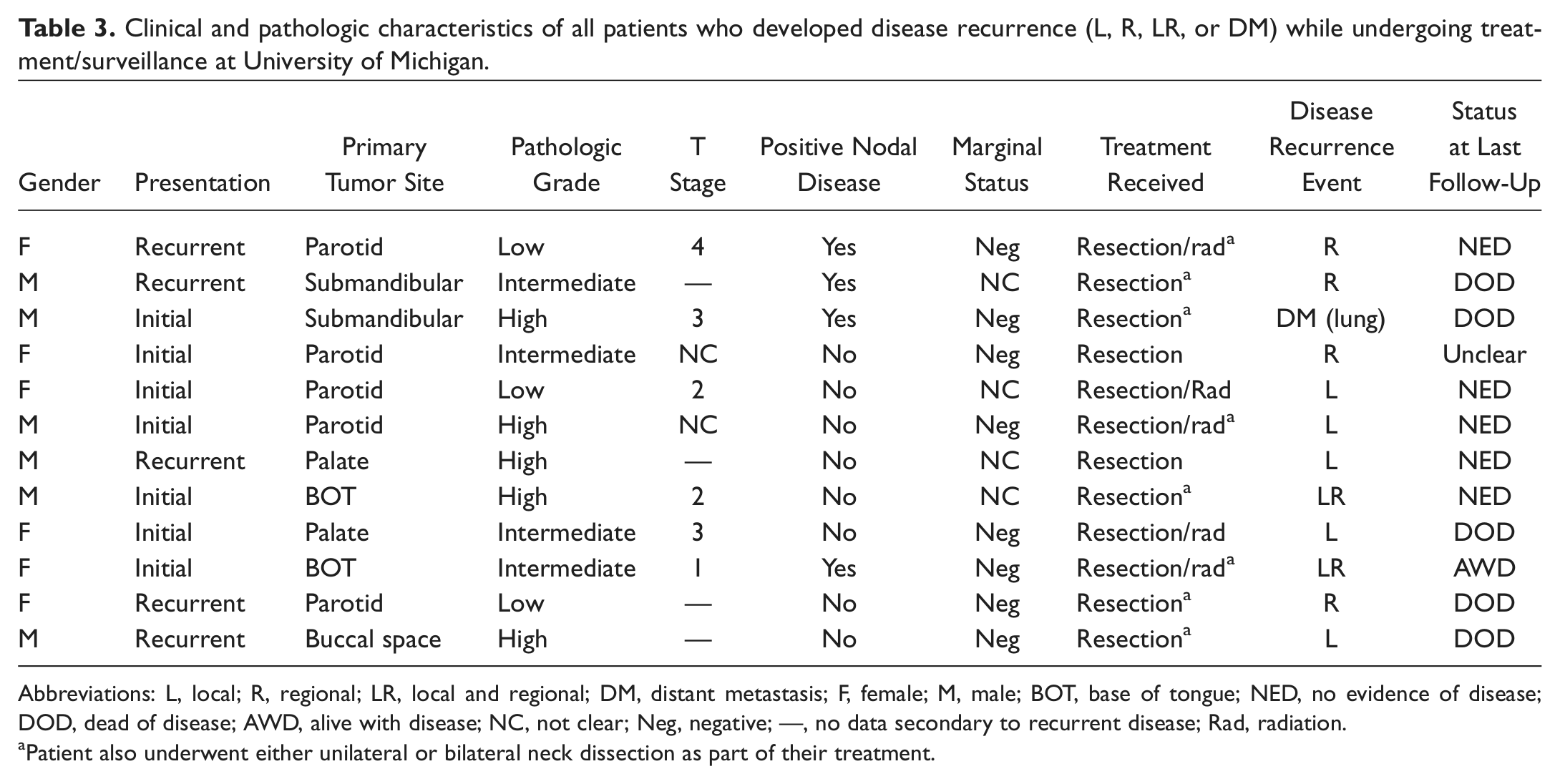
Abbreviations: L, local; R, regional; LR, local and regional; DM, distant metastasis; F, female; M, male; BOT, base of tongue; NED, no evidence of disease; DOD, dead of disease; AWD, alive with disease; NC, not clear; Neg, negative; —, no data secondary to recurrent disease; Rad, radiation.
Patient also underwent either unilateral or bilateral neck dissection as part of their treatment.
Sixteen of 101 (15.8%) patients were lost to follow-up. Of the 16 patients who were lost to follow-up, 11 of 16 patients had a follow-up of greater than 1 year and 7 of 16 had follow-up greater than 2 years since completing their treatment. Of these 16 patients, 13 had low-grade tumors. In addition, we were able to calculate overall survival without knowing their disease status by cross-checking the social security death index. When taking this into consideration, 16 of 16 patients had greater than 3 years without death after completing treatment.
Discrepancies in the Diagnosis of Mucoepidermoid Carcinoma
Of the 113 originally diagnosed MEC of the head and neck, 12 were changed to a diagnosis of salivary duct carcinoma upon further pathologic evaluation. The majority of these patients (9/12, or 75%) were male and had their primary malignancy affecting the parotid gland (75%). Seven of 12 (58.3%) were originally diagnosed as high-grade MEC, 3 of 12 (25%) intermediate-grade, 1 of 12 (8.3%) low-grade, and 1 of 12 (8.3%) unknown. Five of 12 (41.7%) had no nodal involvement, while 7 of 12 (58.3%) had 1 or more positive nodes on presentation.
Survival Analysis
The 5-year OS and DSS for the entire cohort was 79% and 95%, respectively, with a median follow-up of 72 and 45 months. The 5-year DFS was 76% with 12 patients developing recurrence. Univariate analysis showed that histological grade was a statistically significant predictor of DFS (P = .001) and OS (P = .04) but was not a predictor of DSS (P = .09) ( Figure 2 ). No statistically significant difference was seen in DFS, DSS, or OS when comparing low- and intermediate-grade cohorts as well as intermediate- and high-grade cohorts. Positive nodal status was a significant predictor of DSS (P = .004). No statistically significant difference was seen in OS in patients with involved lymph node(s) (P = .056) ( Figure 3 ). Due to the small number of patients presenting with nodal disease, there was insufficient data to conclude whether positive nodal status was predictive of DFS.
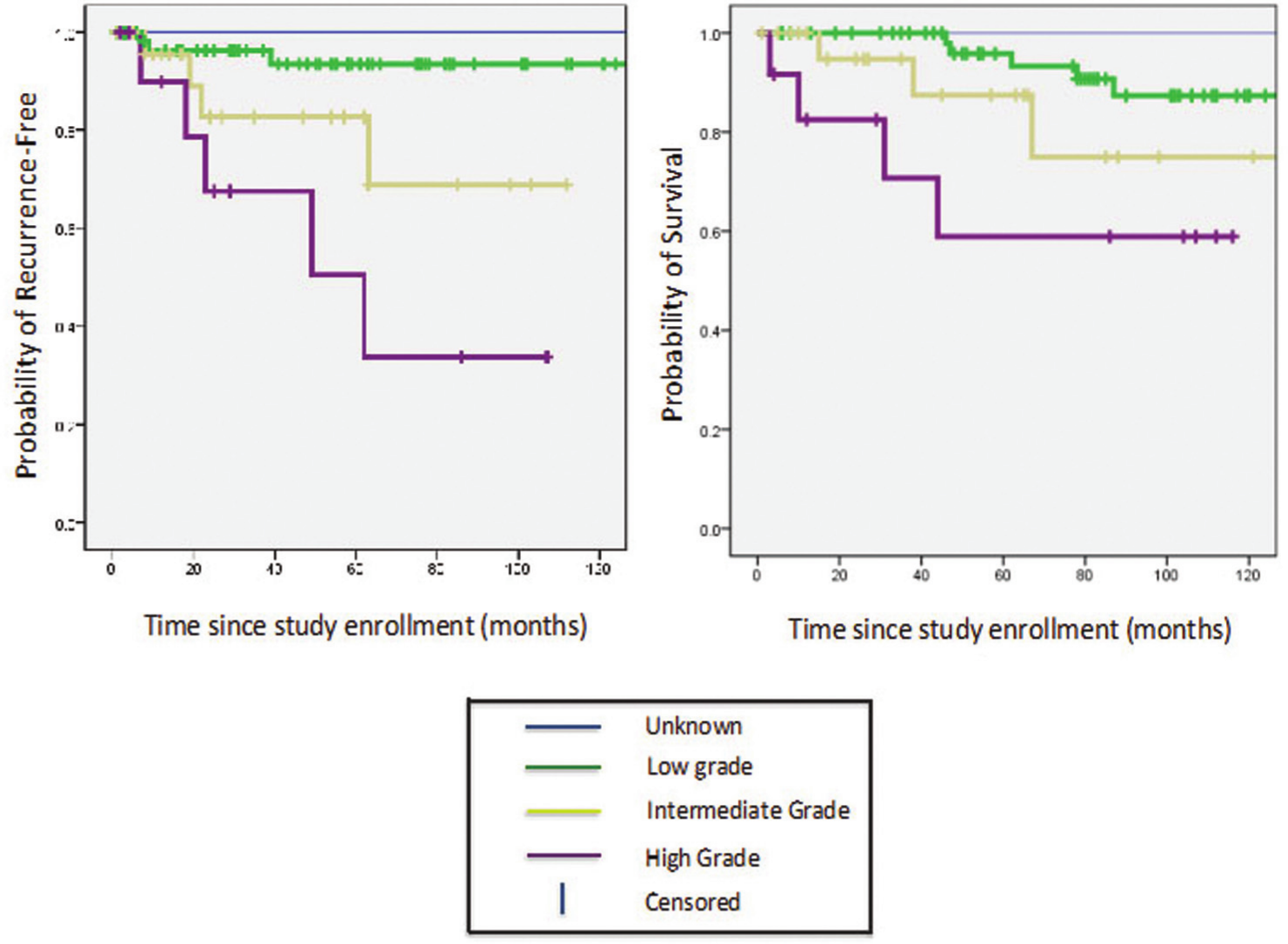
Recurrence-free survival (RFS) and overall survival (OS) stratified by histologic grade.
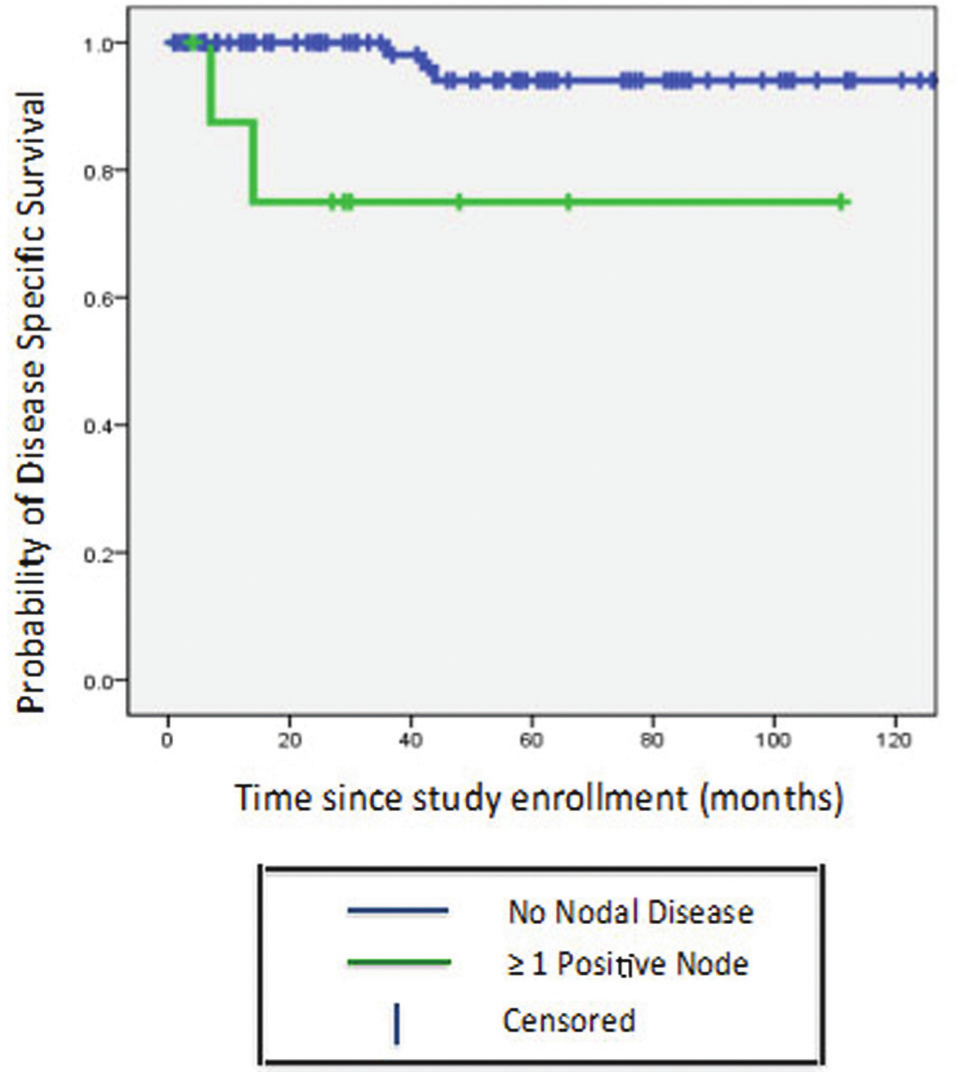
Disease-specific survival (DSS) stratified by nodal status.
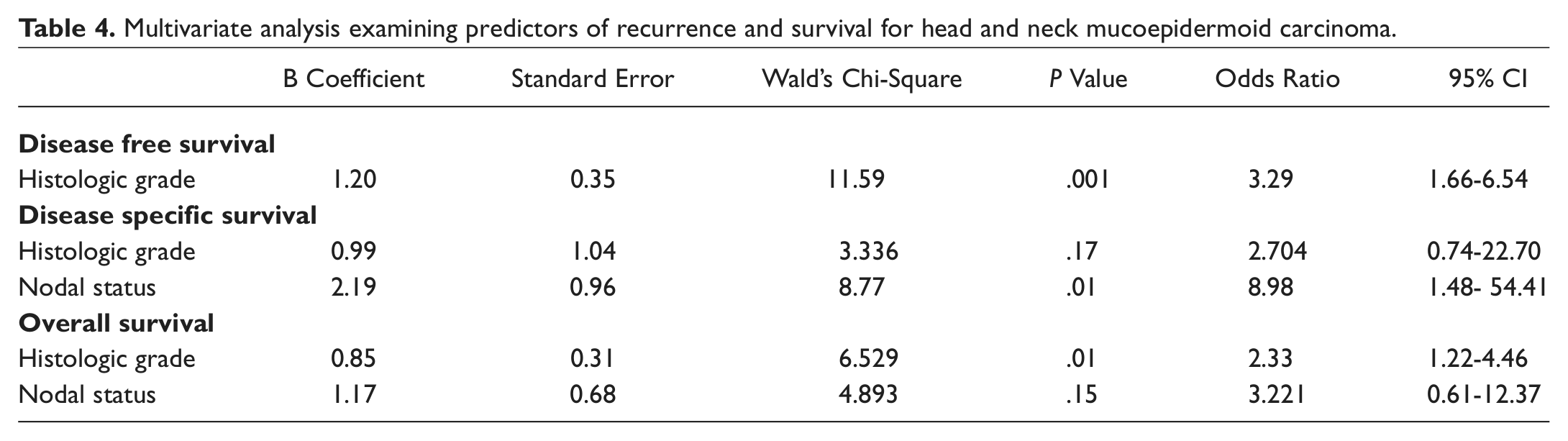
A multivariable analysis was performed with univariate predictors that had a P value of <.10. Histologic grade remained an independent predictor of OS (Hazard ratio 2.33, 95% CI, 1.22-4.46, P = .01) and DFS (Hazard ratio 3.29, 95% CI, 1.66-6.54, P = .01). Positive nodal status remained an independent predictor of DSS (Hazard ratio 8.98, 95% CI, 1.48-54.41, P = .01). A more detailed description of the analyses is shown in Table 4 .
Multivariate analysis examining predictors of recurrence and survival for head and neck mucoepidermoid carcinoma.
There was no statistically significant difference in DFS, DSS, or OS based on sex, age, anatomic subsite, T stage, adjuvant therapy, and margin status. Analysis of extracapsular spread, another known prognostic factor, was limited by small sample size (n = 3).
Discussion
In this cohort, advanced histological grade and positive nodal status are the strongest independent predictors of prognosis in head and neck MEC patients. Although there is not a uniformly accepted grading system for MEC, histological grade has been found to be predictive of recurrence and survival and dictates treatment paradigms for these tumors.8,11,16,17 Because low-grade tumors characteristically have a less aggressive clinical course, they are typically treated with surgical excision alone. High-grade tumors are generally treated with surgical excision, ipsilateral neck dissection, and adjuvant external beam radiotherapy. 12 The clinical behavior of intermediate-grade tumors is not well established and elucidating an optimal treatment protocol is much more challenging.
Studies have demonstrated that there is no significant difference in DSS and OS between low- and intermediate-grade MEC but note a significant difference in DSS and OS between the intermediate- and high-grade groups. 7 This suggests that the clinical behavior of intermediate-grade MEC of the head and neck is more similar to low-grade MEC. However, our data did not show a significant difference in DSS or OS when comparing the low-grade and intermediate-grade groups or the intermediate-grade and high-grade cohorts. This may be explained by the addition of more advanced treatment, such as radiotherapy, predominantly to the high-grade group compared to the intermediate- and low-grade cohorts (58.3% vs 29.2 and 17.2, respectively). It is also possible that more aggressive tumor biology may be better explained by molecular marker analysis.
According to the literature, advanced tumor stage positively correlates with advanced histological grade and poor prognosis.7,11 However, in our study advanced T stage tumors accounted for a significant number of patients among all histological grade cohorts (T3/T4 low-grades: 46.9%; intermediate-grade: 62.5%; high-grade: 41.6%). Despite having 49.5% of our head and neck MEC patients present with advanced T stage (T3, T4) and 12.9% present with recurrent disease, our 5-year OS and DSS for the entire cohort was excellent (79% and 95%, respectively). Advanced T stage within all histological grade cohorts could also explain why no significant difference in DSS or OS was seen when comparing the low-grade and intermediate-grade groups as well as the intermediate-grade and high-grade cohorts.
Our study, which was comprised of a large cohort of head and neck MEC (n = 101), is somewhat unique in that our larger sample size adds strength to our conclusions. Except for the McHugh group, a fairly extensive literature search demonstrates few prior studies with such large sample size. In this study, clinicopathologic analysis was limited secondary to the excellent disease-specific survival (95%). Further pathologic examination of our original head and neck MEC patients (n = 113) revealed that 12 originally diagnosed MEC cases (7/12 high-grade, 3/12 intermediate, 1/12 low, and 1/12 unknown) were in fact salivary duct carcinomas. Eliminating these misdiagnosed MEC from our analysis reduced the high-grade population from 19 to 12, further limiting our statistical analysis. Recent data have also demonstrated similar discrepancies in the morphologic diagnosis of MEC, particularly in the high-grade malignancies.18 -20 These findings highlight the importance of accurate histological diagnosis in managing and studying patients with salivary gland carcinoma.
In conclusion, our clinicopathologic study of MEC suggests that advanced histological grade and positive nodal disease continue to be the strongest independent predictors of overall and disease-specific survival, respectively. Further understanding of the tumor biology may shed light on the highly variable clinicopathologic features associated with the disease. Molecular marker studies are currently in progress to help us better understand tumor behavior and optimal treatment strategies for MEC of the head and neck.
Author Contributions
Disclosures
Footnotes
Acknowledgements
The authors gratefully acknowledge the following individuals in the preparation of this manuscript: Mark Prince, Douglas Chepeha, Gregory Wolf, and Jeffrey Moyer.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.