
Abstract

Cowden’s disease (CD), or multiple hamartoma syndrome, is characterized by various ecto-, meso-, and endodermal benign and malignant tumors. It is inherited in an autosomal dominant manner with 80% of patients having a germ-line mutation of the PTEN tumor suppressor gene. The estimated incidence is 1/200,000. 1
We present herein a rare case of CD with sinonasal and laryngeal manifestations. To our knowledge, this is the second reported case of CD involving the vocal folds. This study has been approved by the Ethics Committee of the General and University Hospital of Valencia, Spain.
Case Report
A 52-year-old woman presented with unilateral nasal obstruction and dysphonia for the past 20 months. She had been diagnosed with CD in her youth and had experienced multiple tissue involvement over the past 30 years. Verrucoid papules on the face and hands, gum hyperplasia, intestinal polyps, fibrocystic breast disease, hip synovial cysts, thyroid cysts, and vaginal fibroids were part of the disease. A mutation of the PTEN gene was confirmed. The genetic study was performed using PCR-SSCP (polymerase chain reaction–single-strand conformation polymorphism from cutaneous lesions cells DNA). No malignant neoplasms had been found to date. Her family history included 1 brother and 1 sister with CD. Nasal endoscopy revealed a white fibrous mass with cobblestone appearance blocking the right nostril. Flexible laryngoscopy showed a nodular, irregular white lesion of the posterior third of the right vocal cord ( Figure 1A ).
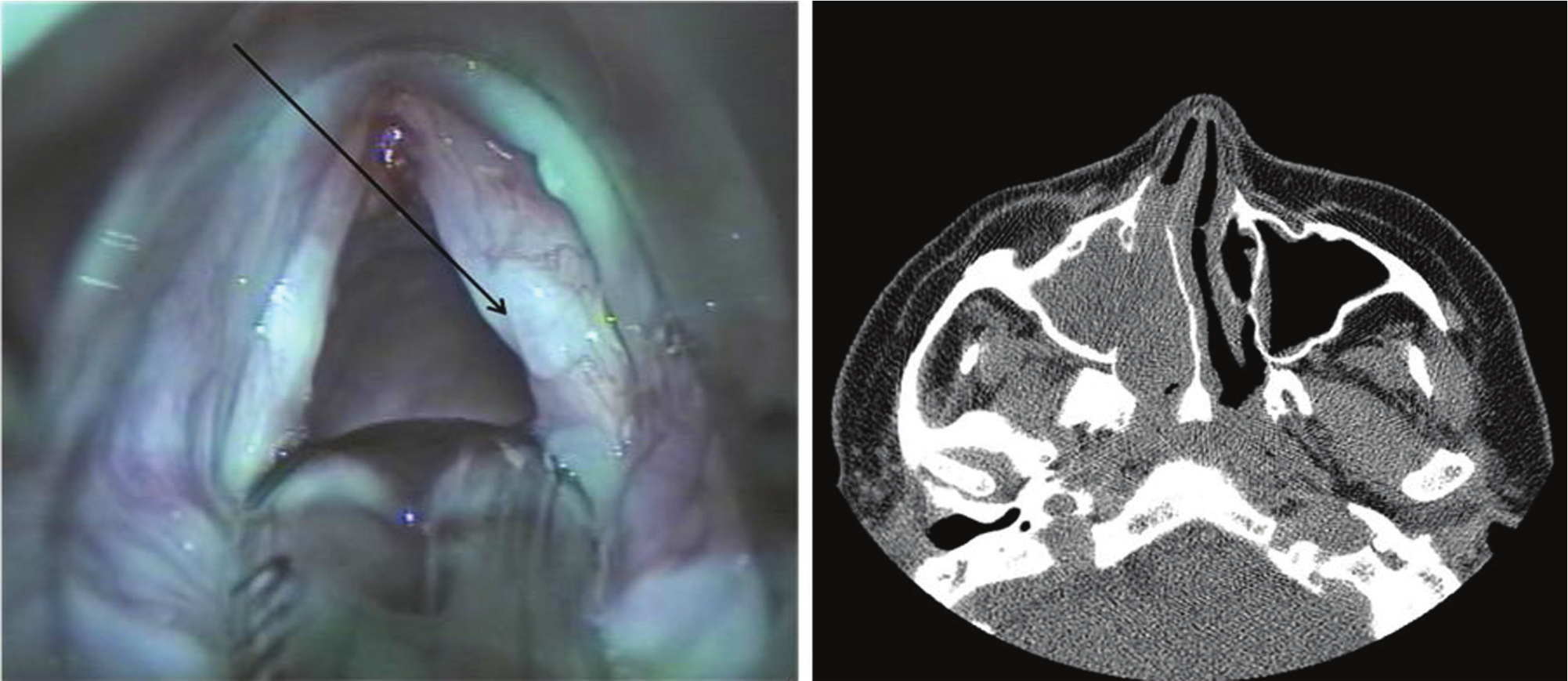
(A) A fibromatous nodular lesion on the right vocal cord (arrow). (B) Maxillofacial computed tomography views show a mass occupying the right maxillary sinus and nostril, with disruption of the left maxillary sinus medial wall.
Computed tomography revealed a large mass in the maxillary sinus destroying its medial wall and filling the entire right nasal cavity ( Figure 1B ).
Given the high risk of malignancies in patients with this syndrome, 2 we decided to perform a transnasal endoscopic medial maxillectomy and direct laryngoscopy. The sinonasal and laryngeal lesions were completely removed.
Pathology report described a fibrous tissue embedded in fibrinoid material with necrotic debris. No atypia or mitotic activity was seen in any of the specimens. There were no signs of inflammatory polyp as interstitial edema or eosinophilic infiltration. These features were consistent with a fibrous lesion of hamartomatous origin ( Figure 2 ).
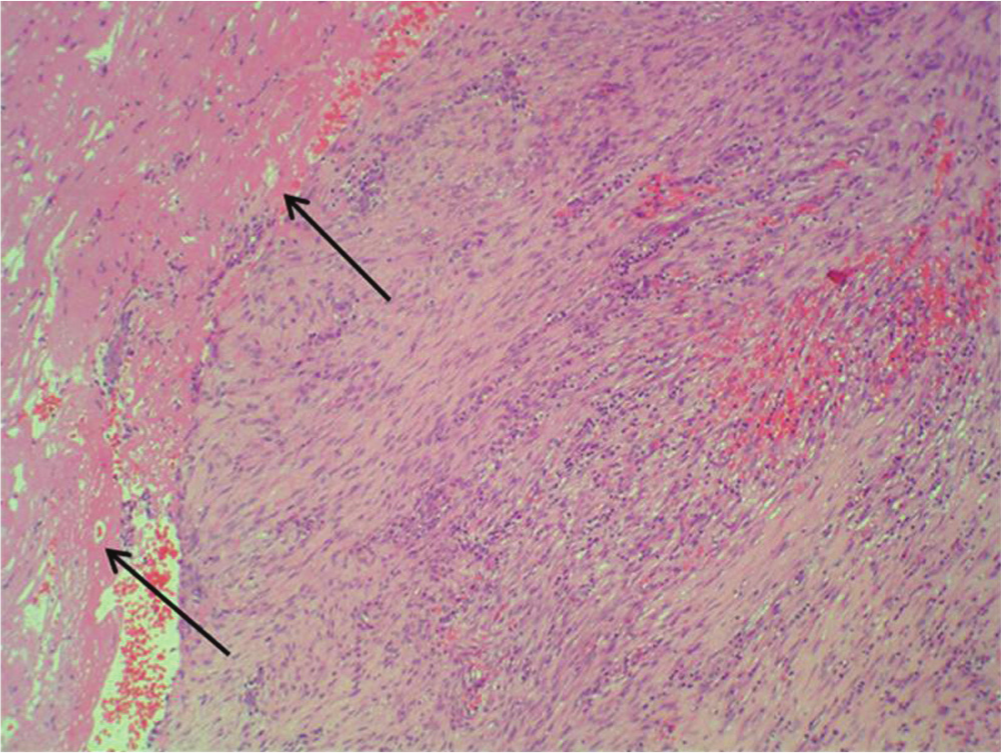
The proliferation of spindle eosinophilic cells with an elongated core and loose chromatin without atypia or mitosis. Necrosis can be seen in the upper left corner (arrows).
The patient had recurrence of her sinonasal and vocal cord masses 1 year postoperatively, and we elected a nonsurgical approach.
Discussion
Cowden’s disease is a hereditary multiple hamartoma syndrome very commonly affecting the head and neck regions. Mucocutaneous hamartomas of the buccal, gingival, and pharyngeal spaces are found in almost 100% of cases, and they have a cobblestone appearance.2,3
Thyroid cancer, following breast cancer, is the second most common malignancy associated with CD. In addition, benign multinodular goiter, adenomatous nodules, and follicular adenomas appear in up to 75% of patients. The genitourinary and gastrointestinal tracts are also frequently affected. 3
As previously mentioned, to our knowledge this is the second reported case of CD involving a vocal fold 2 and one of the few described cases of CD involving the maxillary sinus and nasal cavity. These cases have been described as respiratory epithelial adenomatoid hamartoma: this is a subgroup of hamartomas that more often involves the nasal cavity or nasopharynx and is not part of CD but appears in isolation with no other hamartomatous lesions. 4
Definitive diagnosis depends on recognizing the pattern of the clinical features and the histology of the corresponding lesions. In our case, the predominant tissue was of fibrous origin. This is also observed in hamartomatous polyps in colon CD, in which the glands exhibit dilatation of the lumen and stromal predominance. 5 Therefore, the changes seen, although not pathognomonic, are within the range of lesions described in patients with CD ( Figure 2 ).
The treatment of the head and neck manifestations of CD remains primarily surgical despite the risk of recurrences. 5-Fluorouracil has been used to treat selected mucocutaneous lesions. 3 In this case, surgical excision was selected to clear the patient’s nasal cavity, improve her voice, and enable a histopathologic examination with the purpose of ruling out malignancy. However, the rapid recurrence of the lesions in this patient suggests that surgical treatment of CD in these locations should be primarily directed to discard malignancy. The genetic basis of this disease probably determines its specific evolution.
The diagnosis of CD remains a challenge because of its paucity, and the otolaryngologist should be familiar with this entity and its head and neck manifestations.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.