
Abstract
Objective
To describe and evaluate a novel technique for the implantation of bone conduction hearing devices as compared with a common, conventional technique.
Study Design
Case series with chart review.
Setting
Tertiary referral otology and neurotology practice.
Methods
Individuals who underwent the implantation of bone-anchored hearing devices between January 1, 2004, and December 31, 2011, were identified. Demographic data, surgical indications, surgical technique used, surgical time, and complications were recorded. Soft tissue complications were graded on the Holgers classification scheme. Group 1 was defined as those undergoing a traditional technique using a dermatome with subcutaneous tissue reduction. Group 2 was defined as those undergoing the described technique for implantation of the coupling hardware with minimal subcutaneous soft tissue reduction.
Results
Forty patients underwent the procedure, with 11 patients comprising group 1 and 29 patients comprising group 2. Group 2 required a shorter operative time (32.3 vs 56.1 minutes, P < .0001). Of patients in group 1, 2 of 11 developed soft tissue complications, whereas 5 of 29 in group 2 developed soft tissue complications (P = 1.000). Most soft tissue complications were reversed with conservative wound care.
Conclusion
Surgery was performed faster with similar postoperative outcomes in individuals undergoing implantation of bone-anchored hearing devices using the described technique that necessitated minimal soft tissue reduction.
Bone-anchored hearing aids (BAHAs) are indicated for individuals with single-sided deafness and in situations of mixed or conductive hearing loss where conventional hearing aids are either contraindicated or difficult. This includes cases of chronic otitis media, chronic otitis externa, or atresia or stenosis of the ear canal.1,2 Bone-anchored hearing aids are composed of a processor that is coupled to a transducer that is present percutaneously and implanted into the skull. This percutaneous transducer or coupling post comprises 2 parts. The portion that is implanted in the skull is called the titanium implant, and the portion extending percutaneously from the titanium implant is called the abutment. It is to the abutment that the processor attaches.
As compared with bone conduction hearing aids, BAHAs result in an increased auditory gain of 10 to 25 dB depending on frequency. 3 The technique that has been commonly employed for the implantation of the percutaneous coupling post for BAHAs includes the use of a dermatome to produce a U-shaped skin flap with subcutaneous tissue reduction at the implant site. 4 This technique was used to allow clearance of a relatively short abutment over the surrounding skin. 5 Unfortunately, this technique has been accompanied by a significant rate of soft tissue complications, including flap loss and skin overgrowth.5-7
The relatively recent availability of longer abutment lengths has called into question the necessity of aggressive subcutaneous tissue reduction at the implant site. Currently, both the Oticon Medical (Askim, Sweden) and Cochlear Corporation (Macquarie, Australia) osseointegrated auditory implant systems offer a 9.0-mm abutment length in addition to the 6.0-mm abutment length. Previously, only a 5.5-mm abutment length was available. Preliminary studies by Pelosi and Chandresekhar 8 indicated that an 8.5-mm abutment remedied cases of soft tissue overgrowth over the shorter 5.5-mm abutment.
The senior author (DFW) thus has investigated the feasibility and safety of a technique in the implantation of osseointegrated auditory implants with minimal subcutaneous tissue reduction with the hypothesis that this would shorten surgical time while potentially reducing the rate of soft tissue complications.
Methods
Surgical Technique
Anesthesia is performed according to patient and anesthesiologist preference. Once anesthesia is attained, the implant site is marked 5.5 to 6.0 cm posterior to the external auditory meatus along the temporal line. The proposed implant site is then infiltrated with local anesthesia. A 4-mm diameter biopsy punch is used with a blade length of 6 mm ( Figure 1 ). This biopsy punch is then used to remove skin and underlying soft tissue at the proposed implant site to the skull surface ( Figure 2 ). The immediate surrounding subcutaneous tissue and periosteum are removed in a conical shape from the scalp surface toward the skull to allow adequate visualization of the proposed implant site ( Figure 3 ). Care is taken to remove a greater amount of subcutaneous tissue on the superior aspect to guard against gravity-induced scalp migration onto the abutment. Once hemostasis is obtained, the guide drill is used to establish the skull depth, and either a 3-mm or 4-mm counter-sink is used to drill the recipient site for the titanium implant.
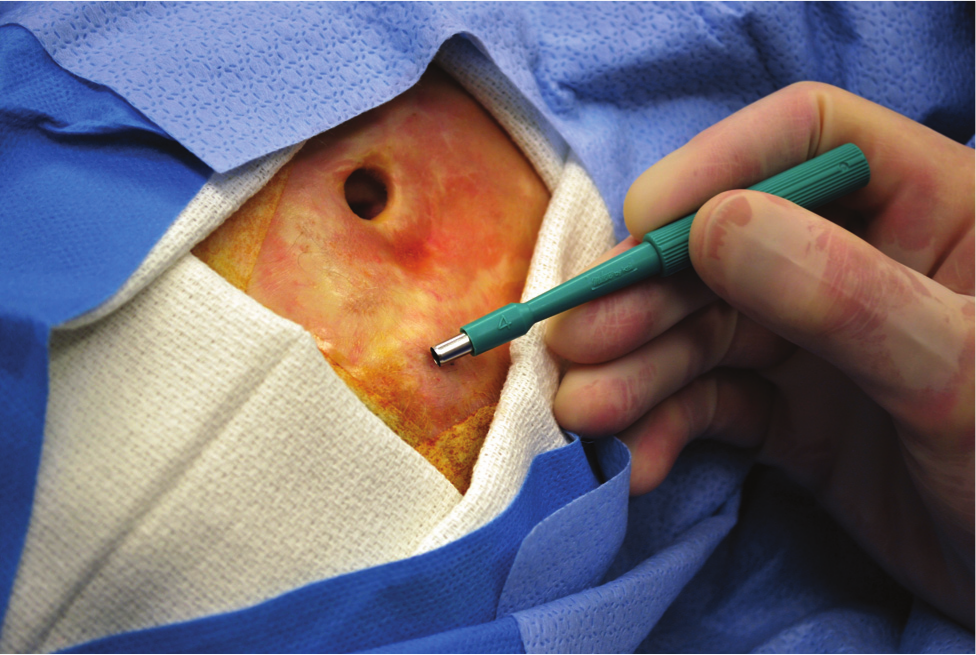
A 4-mm biopsy punch used at the implant site to facilitate removal of soft tissue to the periosteum. Once used, further soft tissue removal is performed in an inverted conical fashion to the skull, including removal of the periosteum.

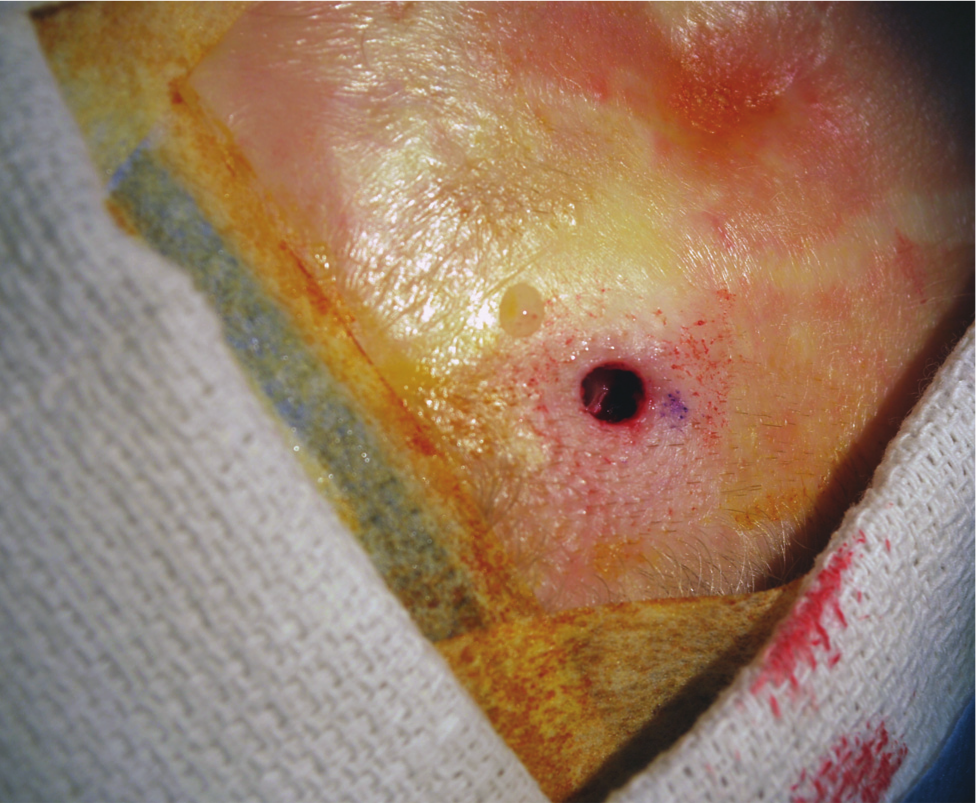
Biopsy punch being used to remove the soft tissue at the implant site.
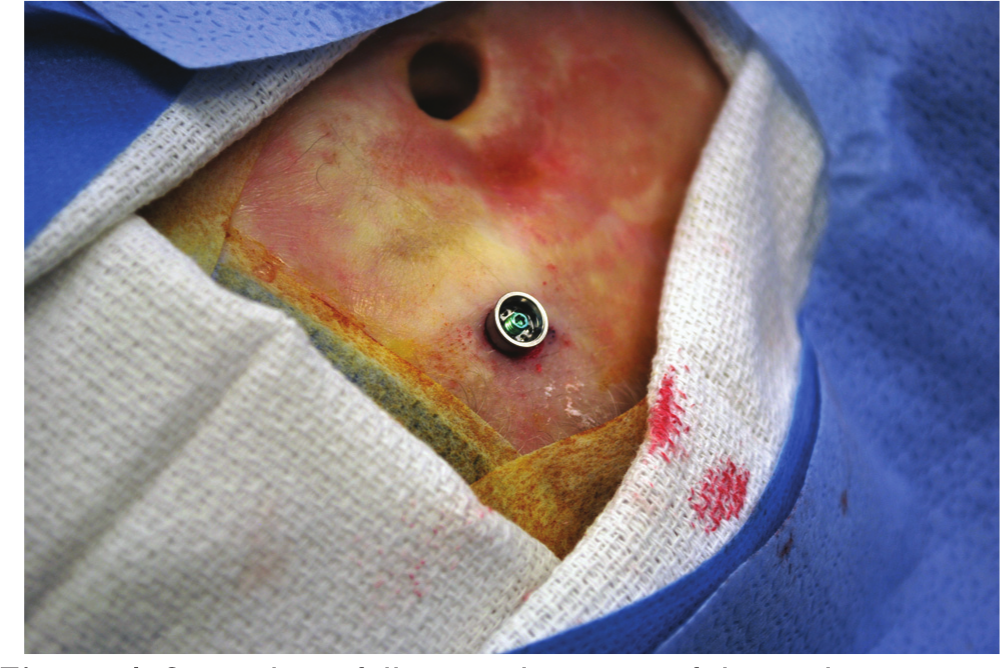
Implant site following removal of soft tissue down to the bone.
The thickness of the scalp is measured using a measuring probe. The abutment size chosen is at least 3 mm longer than the thickness of the scalp. In the senior author’s experience, the 9-mm abutment length is the most frequently used size. Based on the scalp thickness and the skull depth, the appropriate titanium implant-abutment coupling is used. Figure 4 shows the implant-abutment couple in place. Once the implant is placed, a Xeroform gauze is rolled and placed around the abutment and buttressed with a healing cap. This dressing is then removed 3 to 5 days postoperatively. The appearance of the implant after 6 weeks is shown in Figure 5 . Activation of the processor is then performed 6 or 7 weeks after surgery.
Surgical site following placement of the implant.

Surgical site at 6 weeks after surgery.
The Cohort
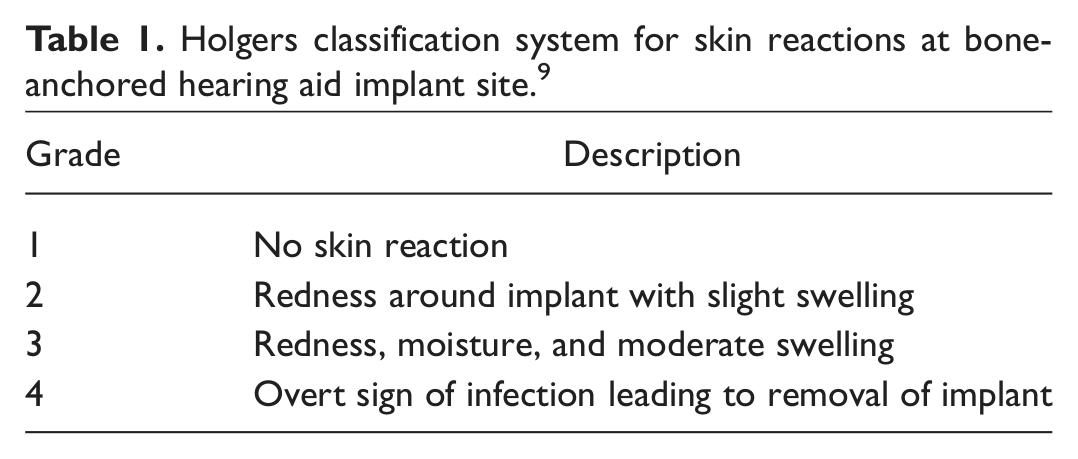
After institutional review board (IRB) approval was received by the Legacy Health Systems IRB, a retrospective study was conducted identifying all patients who underwent the implantation of a BAHA between January 1, 2004, and December 31, 2011. The medical records were attained with note of age at time of surgery, sex, surgical indication, technique used (dermatome skin flap with soft tissue reduction vs biopsy punch technique), type of anesthesia administered, surgical procedure time, total time in the operating room, and the presence of any perioperative or postoperative complications. A complication was defined as an instance that would require additional postoperative care, including local wound care, antibiotics therapy, and return to the operating room. A minor complication was defined as one that necessitated care that could be provided in a postoperative clinic visit. A major complication was defined as revision surgery necessitating an operating suite. Soft tissue complications were classified according to the Holgers classification system ( Table 1 ). 9 Those patients who underwent the procedure using the dermatome for the elevation of a skin graft with associated soft tissue reduction were designated group 1. Those who underwent the procedure using the biopsy punch and minimal subcutaneous reduction as previously described were designated group 2.
Holgers classification system for skin reactions at bone-anchored hearing aid implant site. 9
Statistical Analysis
Particular attention was given to the surgical procedure time, total time in the operating room, and the incidence of complications. A 2-tailed Student t test was used to determine statistical significance in the surgical time and total time in the operating room for the 2 treatment techniques. A 2-tailed Fisher exact test was used to determine a difference in the observed complication rates in the 2 groups. Duration of follow-up was at least 12 months.
Results
Forty patients underwent BAHA implantation during the study period. Eleven patients underwent the procedure using the dermatome (group 1), whereas 29 patients underwent the procedure using the biopsy punch technique (group 2). Table 2 illustrates the study cohort. There was no significant difference in mean age between the 2 groups, although the sex distribution did differ, with slightly more women comprising group 1 (5 men vs 6 women), whereas men outnumbered women in group 2 (17 men vs 12 women).
Study cohort characteristics.
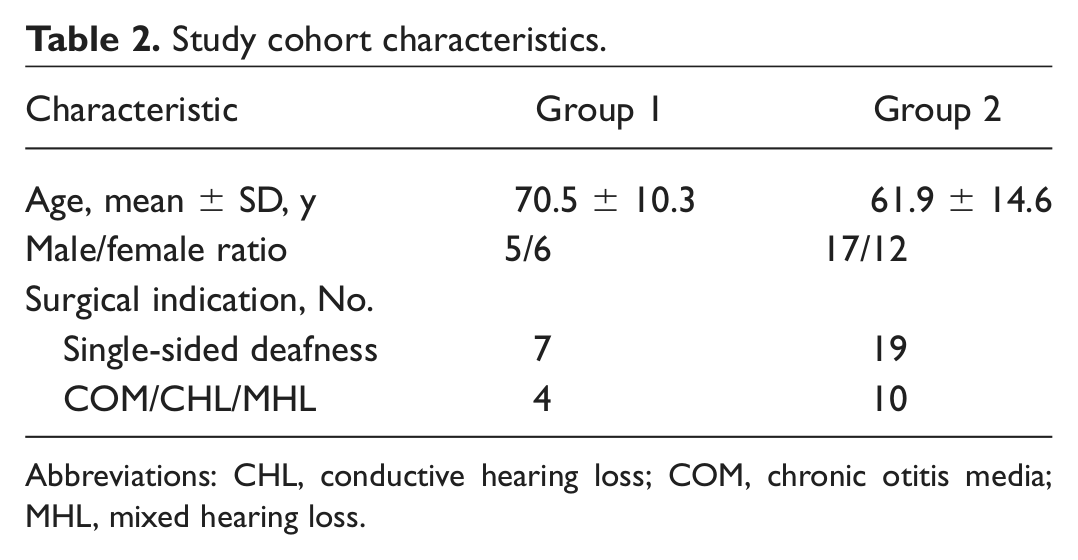
Abbreviations: CHL, conductive hearing loss; COM, chronic otitis media; MHL, mixed hearing loss.
In examining the surgical times, it became evident that the relatively simple technique used in group 2 resulted in a statistically significant shorter mean surgical time (32.3 ± 9.6 minutes vs 56.1 ± 12.9 minutes, P < .0001). Mean total time in the operating room was also significantly reduced in group 2 (73.7 ± 14.4 minutes vs 96.4 ± 11.5 minutes, P = .0033). Further examination shows that those in group 2 were more likely to undergo surgery with local anesthesia with sedation as opposed to general anesthesia (15/27 vs 2/11), which would also be expected to reduce total time in the operating room.
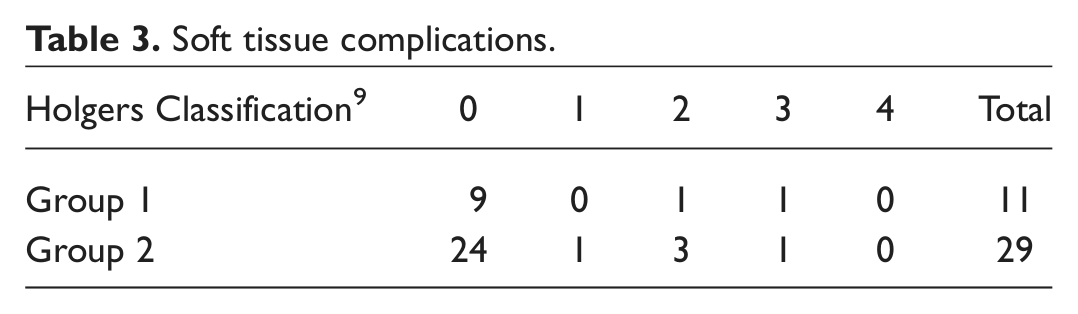
The complication rate did not differ between the 2 groups, with 2 patients in group 1 needing office intervention and 5 patients in group 2 requiring additional intervention (P = 1.000, 2-tailed Fisher exact test). Table 3 delineates the postoperative skin reactions seen according to the Holgers scheme. No patients in group 1 required a return to the operating room to address their complication. By contrast, 1 patient in group 2 returned to the operating room for soft tissue reduction for tissue that had grown over the abutment. In this patient, a 5.5-mm abutment originally had been placed. At the secondary procedure, a longer 8.5-mm abutment was placed following soft tissue reduction. The incidence of major complications did not differ significantly between the 2 groups (0/11 vs 1/29, P = 1.000, 2-tailed Fisher exact test). Furthermore, there were no instances of implant extrusion in either group during the follow-up period.
Soft tissue complications.
Discussion
The advent of the bone-anchored hearing aid has offered improved auditory performance for those who are not ideal candidates for conventional hearing aids. These individuals include those with aural atresia, unilateral deafness, or chronically draining ears with hearing loss.1,2 A bone conduction hearing device coupled to the skull through a percutaneous transducer is preferred to the standard bone conduction hearing aid for the relatively superior auditory benefit these devices provide. 3 Furthermore, BAHAs are preferred on an aesthetic basis when compared with most bone conduction hearing aids.
Various techniques for BAHA implantation have been described.4-6,10-12 Most of these techniques include significant soft tissue reduction to minimize scalp mobility and ensure clearance of the abutment. This technique was recommended because scalp mobility around the implant was thought to cause soft tissue irritation leading to overgrowth. Variability in soft tissue complication rates seemed to rely on the extent of thinning of the subcutaneous tissue surrounding the abutment. For instance, a full-thickness skin flap resulted in a lesser incidence of postoperative soft tissue complications when compared with a split-thickness skin graft. 7 Wilkinson et al 10 and de Wolf et al 11 took this a step further using a linear incision with soft tissue reduction rather than employing any U-shaped flap. Subsequently, Hulcrantz 12 showed that no soft tissue reduction did not compromise implant stability or surrounding soft tissue status following BAHA implantation. This has been further validated by the histologic findings of Larrson et al, 13 who found limited or no signs of inflammation in the soft tissue surrounding the abutment when no soft tissue reduction was performed with BAHA implantation in sheep. Our technique takes a further step with even less manipulation of the soft tissue surrounding the implant. Whereas Hulcrantz employed a linear incision that incorporated a separate hole to accommodate the abutment, we explored and confirmed the feasibility of a procedure necessitating, in most cases, a hole produced by a biopsy punch.
As noted previously, soft tissue reduction was first employed by Stalfors and Tjellström 5 to allow the abutment to clear the surrounding skin. Until recently, abutment length was limited to 5.5 mm since implant stability within the skull limited the torque force that could be tolerated. Unfortunately, the technique using the dermatome was accompanied by radical soft tissue reduction surrounding the abutment, leading to local inflammatory reactions in up to 36.6% of individuals. 6 As such, authors have sought improved techniques.
The introduction of wider implants has allowed for greater surface area of osseointegration in the skull. This results in greater distribution of cantilever forces from placement and removal of the processor off the abutment. This has allowed longer abutment lengths without greater vulnerability to the extrusion, as confirmed by D’Eredita et al. 14 As a result, soft tissue reduction has become mostly unnecessary. It has also allowed earlier loading of the processor, with McLarnon et al 15 finding implant stability as early as 3 weeks following implantation.
The relatively simplified technique described in this article has shown greater ease in achieving adequate local anesthesia. This has been indicated by the relatively greater proportion of our patients who underwent the surgery under local anesthesia when the punch biopsy technique was used. This has also allowed the performance of surgery in a shorter period with similar complication rates. We hypothesize this is due to the relatively reduced area that needs to be anesthetized through this technique. Although total time in the operating room was also reduced in group 2 as compared with group 1, this comparison is complicated by the relative greater frequency by which general anesthesia using an endotracheal tube or laryngeal mask airway was employed in group 1.
The technique described in this article is quite similar to the technique described by Goldman et al. 16 They also use a biopsy punch and proceed with the drilling and placement of the implant through the hole derived from the biopsy punch. Our technique differs in that we use a 4-mm punch as opposed to a 12-mm punch but make up for the reduced visibility by using an operative microscope. Furthermore, we compensate for the inevitable gravity-induced migration of the scalp cephalad to the abutment onto the abutment. Clinically, our findings are similar in that we found a shorter operative time with this technique and a higher incidence of the procedure being performed through local anesthesia. 16
This study does suffer from the weaknesses inherent in retrospective studies. Furthermore, this study includes a relatively small cohort that underwent the procedure with the use of a dermatome accompanied by substantial soft tissue reduction. Despite this, though, the relatively larger group that received minimal soft tissue manipulation during the procedure clearly did not have a substantially higher rate of soft tissue complications.
Conclusion
Successful implantation of BAHAs can be performed with shorter surgical and operating room time with similar safety using a biopsy punch technique with minimal soft tissue reduction.
Author Contributions
Disclosures
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.