
Abstract

Introduction
Since its introduction, robotic-assisted transaxillary thyroidectomy (RATT) has been proven to be a feasible and safe surgical technique and is gaining wide popularity. 1
Tracheal injury is a rare complication of thyroidectomy 2 and can be repaired immediately, if promptly recognized during the operation. Delayed tracheal leakage after thyroidectomy is described only in sporadic reports. In the largest case series of RATTs, Chung et al 1 reported 2 patients with tracheal injury, both recognized during the operation. To the best of our knowledge, this is the first report of a delayed tracheal leakage after an apparently uneventful RATT.
Case Presentation
A 39-year-old woman with a benign 5 cm nodule in the left thyroid lobe underwent transaxillary robot-assisted left hemi-thyroidectomy. Surgery was uneventful and the operative time was 110 minutes.
The patient was discharged on the second postoperative day after an uneventful course. In particular, there was no report of cough or swelling while in the hospital, neither during the following days.
After 38 days, she was readmitted presenting subcutaneous emphysema that suddenly arose after a sneeze, concurrently with a popping sound. The patient was asymptomatic except for the emphysema, which consisted of a 10 cm area in the anterior part of the neck, extending to the clavicle. Chest and neck CT scan excluded pneumomediastinum or pneumothorax. In particular, presence of air in the axilla, under the great pectoralis muscle, was excluded and the tracheal wall appeared intact ( Figure 1 ). Blood tests were normal.
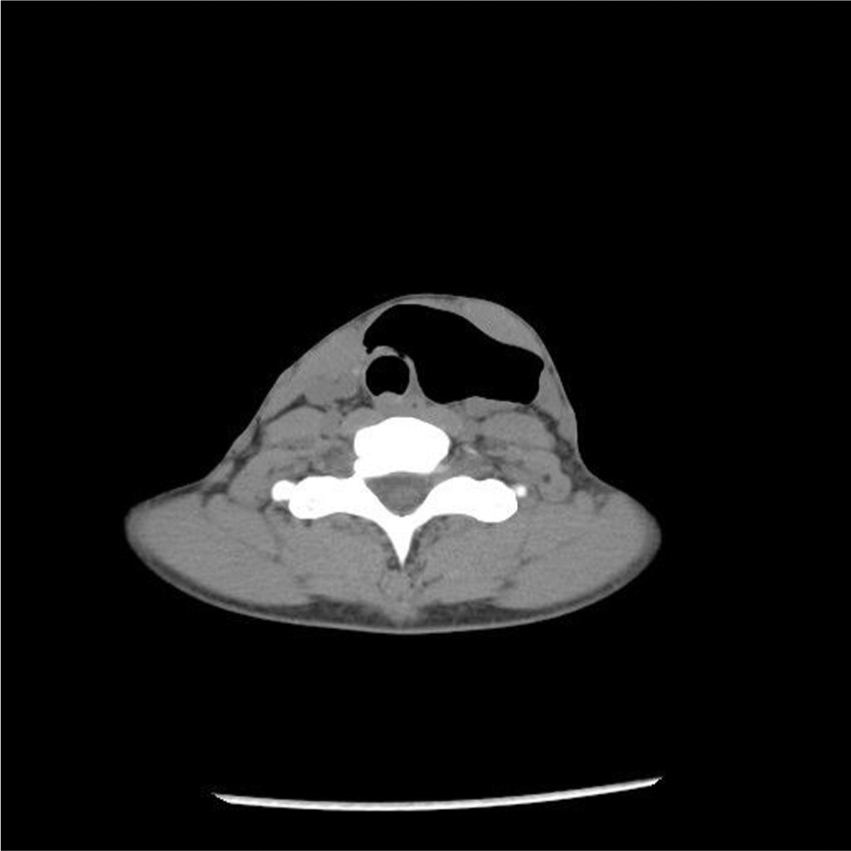
Neck and chest CT scan showing subcutaneous emphysema, with an apparently intact tracheal wall.
Close observation was chosen as treatment option, with prophylactic antibiotic administration. A bronchoscopy performed immediately after admission revealed a 2-mm rounded hole in the anterior wall of the trachea, between the first and the second tracheal rings ( Figure 2A ). The day after, a curettage of the edges was performed, and fibrin glue was applied. Patient was discharged after 3 days. After 8 days, a third bronchoscopy showed complete resolution of the leakage ( Figure 2B ). Follow-up at 2 months showed patient’s definitive recovery.
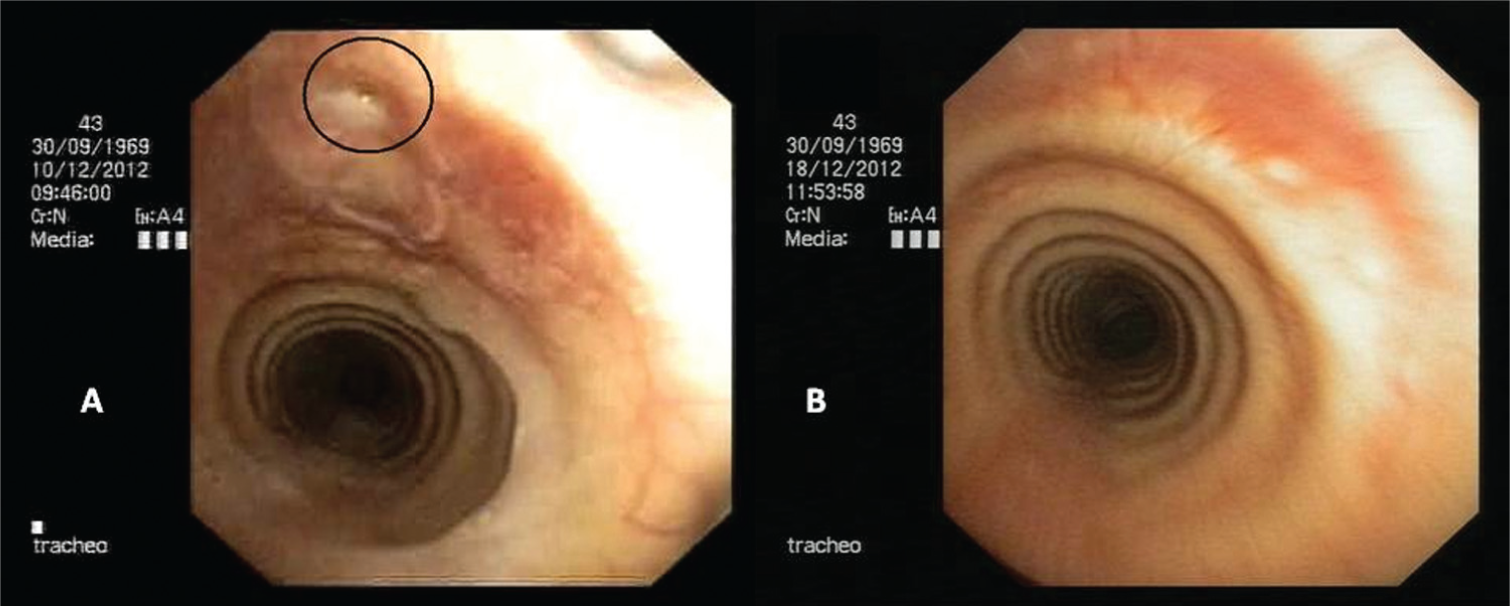
(a) Bronchoscopy: a 2-mm rounded hole in the anterior wall of the trachea is well visible between the first and second tracheal rings. The edges are irregular and partially covered by eschar and present only a few signs of necrosis. (b) Broncoscopy: complete healing of the tracheal injury after 8 days.
This case report was reviewed and approved by the Ethics Committee of the Faculty of Medicine, University of Pisa, Italy.
Discussion
Delayed tracheal ruptures after thyroidectomy are extremely rare and have only been described in sporadic reports. 3 Risk factors include female gender, thyrotoxic goiter, prolonged intubation, use of diathermy, and persistent cough in the postoperative period. Tracheal injury at the time of surgery may not be noticed, or the trachea may undergo necrosis in the early postoperative period, due to devascularization of the tracheal wall through thermal injury from coagulation. Wound infection and weakening of the tracheal wall due to inflammation in Graves disease may also be complicating factors. 3 Symptoms include wound infection; subcutaneous emphysema, sometimes with neck and facial swelling; or progressive respiratory distress. Retrosternal pain and respiratory distress are signs of pneumomediastinum or pneumothorax. Crepitus during palpation of the neck is important for the differential diagnosis with hematoma.
Chest x-ray and chest and neck CT scan are strongly suggested in order to investigate the presence of pneumomediastinum or pneumothorax and identify the site of the injury. Bronchoscopy may also be useful in recognizing the perforation and for treating the leakage with fibrin glue.
The current case differs from previous reports mainly because this is definitely the first report describing a delayed iatrogenic tracheal injury after RATT. Most likely, the delayed tracheal leakage was consequent to a very small injury on the anterior tracheal surface, due to the inadvertent touch with the active blade of the harmonic scalpel, which caused a minimal (not full-thickness) interruption of continuity in the tracheal wall, which was responsible for a slow, progressive, ischemic damage. The treatment strategy in this patient was necessarily influenced by the lack of a cervical incision. In fact, a cervical exploration would have led to the presence of a scar in the neck, nullifying the only major advantage of the RATT, even if the surgical exploration reduces the hospitalization time. 4,5 Until recently, current opinion was to operate on delayed tracheal injuries as soon as the diagnosis was obtained, but recent studies have proven that patients with no respiratory distress, no infection of the surgical site, and stable symptoms should be managed with close observation and prophylactic administration of antibiotics. 4
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.