
Abstract
Objective
To assess the diagnostic value of fever and facial and dental pain in adults suspected of acute bacterial rhinosinusitis.
Data Sources
PubMed, EMBASE, and the Cochrane Library.
Review Methods
A comprehensive systematic search was performed on March 18, 2013. We included articles reporting studies on the diagnostic value of fever or facial and dental pain in patients suspected of acute bacterial rhinosinusitis. For included articles, the reported study design was assessed for directness of evidence and risk of bias. Prevalences, positive predictive values, and negative predictive values were extracted.
Results
Of 3171 unique records, we included 1 study with a high directness of evidence and a moderate risk of bias. The prior probability of bacterial rhinosinusitis was 0.29 (95% confidence interval: 0.24 to 0.35). We could not extract posterior probabilities with accompanying positive and negative predictive values. The study reported an odds ratio from univariate analysis for fever of 1.02 (0.52 to 2.00) and 1.65 (0.83 to 3.28) for facial and dental pain. In subsequent multivariate analysis, the odds ratio of facial and dental pain was 1.86 (1.06 to 3.29).
Conclusion and Recommendation
There is 1 study with moderate risk of bias, reporting data in such a manner that we could not assess the value of fever and facial and dental pain in adults suspected of an acute bacterial rhinosinusitis. Therefore, these symptoms should not be used in clinical practice to distinguish between a bacterial and viral source of acute rhinosinusitis or for decision making about prescribing antibiotic treatment.
Keywords
Clinical Scenario
A 58-year-old woman visits your ear-nose-throat (ENT) outpatient clinic with complaints of nasal congestion, purulent discharge, and both facial and dental pain for 5 days, accompanied by fever (≥38.0°C) since yesterday. You wonder whether the presence of fever and facial and dental pain helps to distinguish between a bacterial and a viral source of acute rhinosinusitis. If so, such simple, fast, and cheap triage could help you to accurately prescribe antibiotics to this patient.
Background
General practitioners and ENT physicians are frequently consulted by patients presenting with signs and symptoms that are suggestive for acute rhinosinusitis. 1 In most patients, acute rhinosinusitis has a viral source and is self-limiting (ie, complaints disappear between 1 to 4 weeks).1,2 However, in about 2% of all cases of viral rhinosinusitis, a superimposed bacterial infection occurs. 2 For acute bacterial rhinosinusitis (ABRS), antibiotics might shorten the duration of symptoms and prevent complications.3-6 Antibiotic treatment in patients presenting with acute viral rhinosinusitis is considered redundant and carries the risk of increasing antibiotic resistance.3-7 Accurate differentiation between a viral and bacterial source of acute rhinosinusitis can help to avoid unnecessary prescription of antibiotics. The current reference test to distinguish between bacterial and viral rhinosinusitis is a culture from either sinus puncture or endoscopically obtained antral aspirate. 4 The feasibility of this approach is low in daily practice, because of the invasive nature of this procedure and the waiting time for culture results. Instead, available practice guidelines recommend diagnostic triage based on fever (≥38.0°C) and facial and dental pain.3,4,8 The evidence base on the diagnostic value of these symptoms remains uncertain.
Searching for Evidence
We evaluated the evidence base on the diagnostic value of the fever (≥38.0°C) and facial and dental pain in adults suspected of ABRS.
Retrieving Studies
Through a comprehensive systematic search (up to March 18, 2013), assisted by our clinical librarian, we retrieved records from PubMed, Embase, and the Cochrane library. The full search syntax with combined relevant search terms and synonyms is displayed in Appendix 1 (available at otojournal.org). Four authors (A.J.H., E.L.L., N.F.E., and P.E.B.) independently removed duplicate publications and screened on title and abstract, selecting studies that assessed the diagnostic value of clinical signs and symptoms in patients with acute rhinosinusitis. Animal or laboratory studies, therapy studies, studies in children, case reports, systematic reviews, and opinion papers were excluded. For final selection, the same 4 authors independently screened full texts of eligible titles in depth and with more detail ( Figure 1 ).
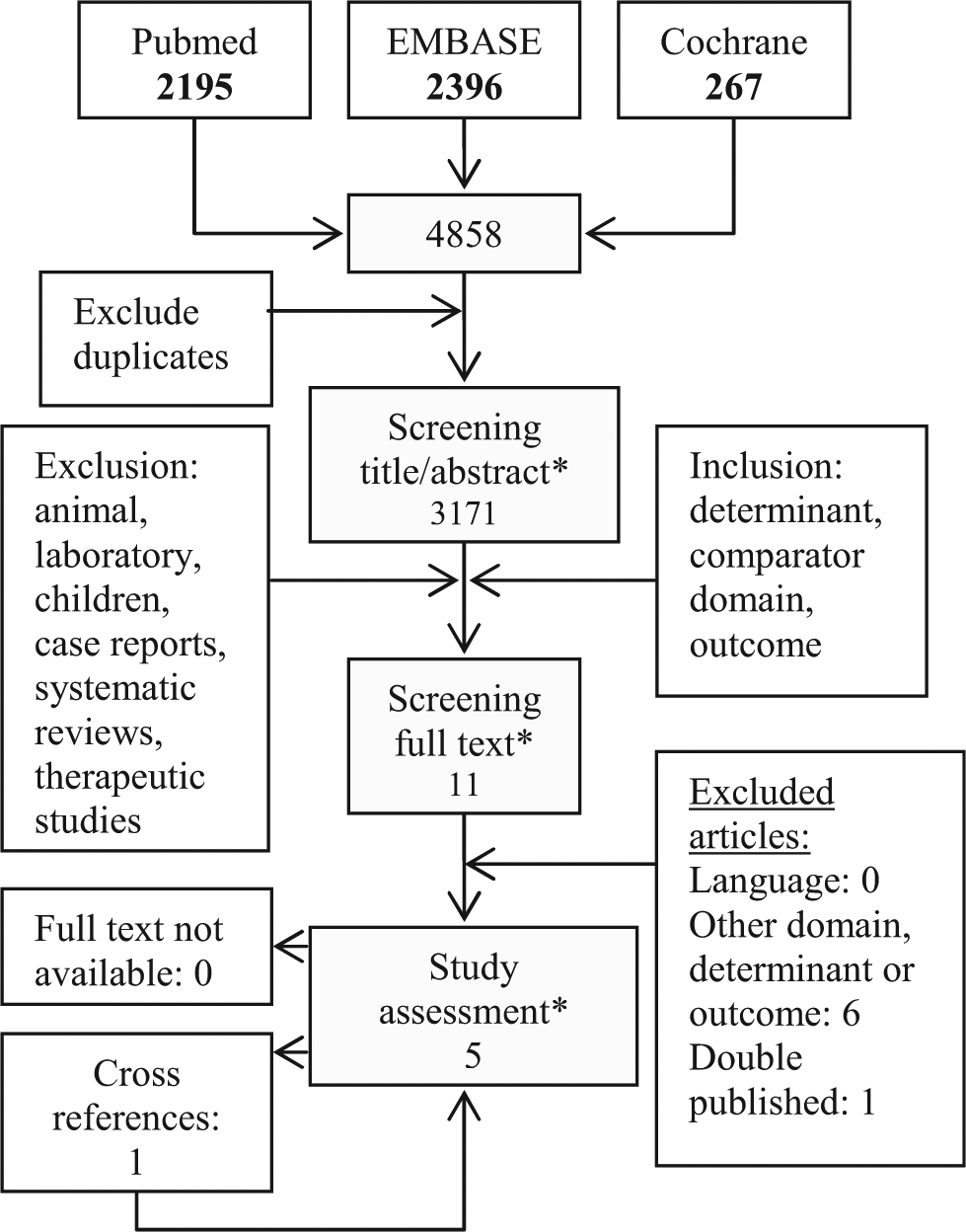
Flowchart of the search and selection of articles. *Based on agreement among 4 independent authors.
The article retrieval was completed by cross-reference checking in Scopus and Web of Science for selected articles, while citations of retrieved reviews, meta-analyses, and guidelines on rhinosinusitis were screened for omitted studies. A similar procedure was followed to check for eligibility of articles that were thereby retrieved. Initial disagreements on eligibility and selection of articles were resolved by discussion, and therefore the inclusion is based on a full consensus.
Assessing Studies
Using predefined criteria, 4 independent authors (A.J.H., E.L.L., N.F.E., and P.E.B.) assessed the design of studies reported in the included articles on their directness of evidence (DoE) and risk of bias (RoB). When item information for the assessment of a DoE or RoB item was not reported or not clearly reported, we rated it as insufficient and considered it as not satisfied. When the reporting allowed assessment, we rated it as either satisfied or not satisfied. Reviewers resolved their initial disagreements by discussion.
Assessment of the DoE involved evaluation of study design characteristics for appropriateness of patients, notably (1) adults suspected of ABRS; index test(s), notably (2) either or both fever (≥38.0°C) and (facial and dental) pain; and the outcome, notably (3) bacterial rhinosinusitis confirmed by culture. Studies were classified as high DoE if they satisfied all aspects of our 3-part question, moderate DoE if they satisfied 2, and low DoE if they satisfied only 1.
Assessment of the RoB involved evaluation of the study design characteristics for selection bias, notably (1) inclusion of an inception cohort, (2) the use of an adequate reference standard; and information bias, notably (3) mutual blinding of assessment of index and reference test(s), standardization of (4) index test(s) and (5) outcome (reference test) and (6) completeness of reported data. Studies were classified as low RoB if they satisfied criteria 1 and 2 plus all other study design features, moderate RoB if they satisfied criteria 1 and 2 but failed on 1 or 2 of the other 4 features, and the remainder were classified as high RoB. We aimed to include studies for data extraction with a high and moderate DoE and low and moderate RoB.
Extraction and Analysis of Study Data
For the included articles, 2 authors (A.J.H., P.E.B.) independently extracted data. We aimed to extract and recalculate the reported true- and false-positive and -negative results for the index test(s). From this, we (re)calculated the prior probability (or prevalence) and the predictive values for a positive (or PPV) and a negative (or NPV) index test, with accompanying 95% confidence intervals (CIs). By comparing prior probabilities with the PPVs and NPVs for fever and facial and dental pain, we evaluated whether these clinical signs were of added value for ruling in or ruling out a bacterial source of acute rhinosinusitis. We excluded papers from our analysis if there were no such data reported, while we present the findings as originally reported if the necessary data could not be (re)calculated.
Results
Retrieving Studies
Our initial search yielded 4858 records. After removing duplicates, 3171 unique publications remained for title and abstract screening ( Figure 1 ). Of these, 11 articles were identified as potentially eligible for study assessment during screening of title and abstract, and their full texts were retrieved.
Based on the full-text evaluation, eventually 4 studies were included for study assessment.9-12 Cross-reference checking yielded 1 additional article for study assessment that was not included in the databases searched. 13 Citations of the 7 excluded articles can be found in Appendix 2 (available at otojournal.org), while the reasons for exclusion of these studies are provided in Appendix 3 (available at otojournal.org).
Assessing Studies
The assessment of studies showed that all studies provided high DoE ( Table 1 ).9-13 We excluded 4 studies because they carried a high RoB.10-13 As such, only 1 study with high DoE and moderate RoB remains for extraction and analysis of data. 9
Characteristics of studies on the diagnostic value of fever and facial and/or dental pain for patients suspected for acute bacterial rhinosinusitis. a

Abbreviations: DoE, directness of evidence; RoB, risk of bias; M, moderate; H, high.
•, satisfied; ○, not satisfied; ⊠, insufficient information/unclear.
Extraction and Analysis of Study Data
Lacroix et al 9 included 265 patients (138 female, median age 35 years, range = 18-93 years) in an outpatient ENT clinic with nasal obstruction and rhinorrhea lasting for less than 4 weeks in duration, suggestive for acute rhinosinusitis. While they excluded patients with a temperature greater than 38.5°C, they documented routine signs and symptoms, including presence of fever and facial and dental pain, and obtained material for culture by a nasopharyngeal aspiration under endoscopic control. A positive culture (Streptococcus pneumoniae, Haemophilus influenza, and Moraxella catarrhalis) was found for 77 of 265 patients (ie, a population prevalence of ABRS or prior probability of 0.29 [95% CI: 0.24 to 0.35]). 9 The true- and false-positive and -negative results for the index test(s) could, however, not be extracted. The first author was contacted to obtain the necessary information but could not provide the requested data. The reported odds ratio from univariate analysis was 1.02 (0.52 to 2.00) for fever and 1.65 (0.83 to 3.28) for facial and dental pain. Subsequent multivariate analysis yielded an odds ratio of 1.86 (1.06 to 3.29) for facial and dental pain ( Table 2 ).
Results. a
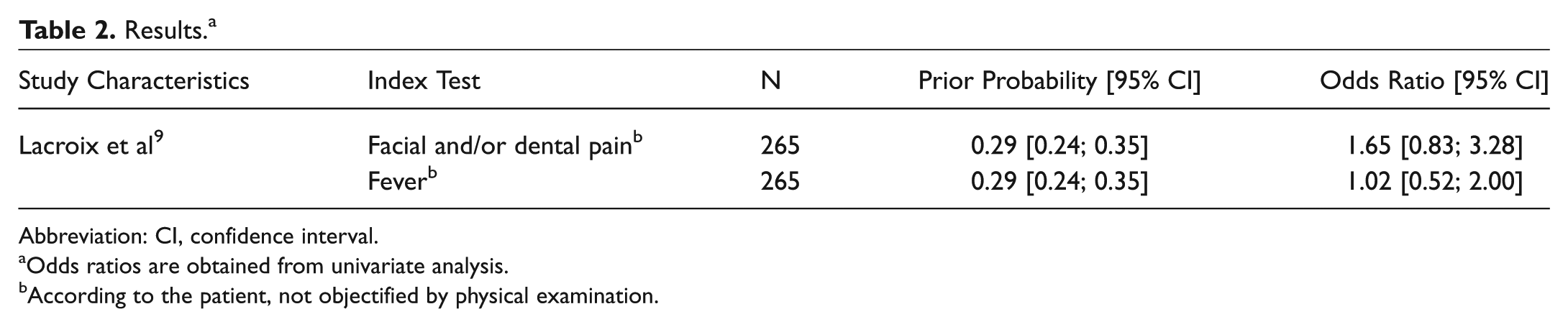
Abbreviation: CI, confidence interval.
Odds ratios are obtained from univariate analysis.
According to the patient, not objectified by physical examination.
Comment
With our comprehensive search on the diagnostic value of fever and facial and dental pain for confirming a bacterial source in patients suspected of ABRS, we identified 1 study with a high DoE and moderate RoB. This study reports odds ratios, which indicate that facial and dental pain was an independent symptom associated with ABRS. However, this study does not report data on the value of fever and facial and dental pain in either ruling in or ruling out ABRS and therefore does not answer our research question. Some aspects need further consideration.
First, we selected studies using cultures of sinus puncture or antral aspirate as a reference test. Different reference tests for the diagnosis of ABRS have been reported in the literature, including radiographic imaging.14-18 Mucosal abnormalities are also common in patients with viral rhinosinusitis, even up to several weeks after resolution of complaints.19-21 Therefore, we considered cultures to be a more adequate reference standard than imaging.
Second, we performed a broad and comprehensive search to identify studies. Still, through cross-reference checking, we retrieved 1 omitted publication. 13 We missed this study because it was not present in the searched databases. However, we believe that because of extensive cross-reference checking in Scopus and Web of Science for selected articles and citation screening of retrieved reviews, meta-analyses, and guidelines, it is not likely that we have missed other potentially relevant studies.
Third, Lacroix et al 9 excluded patients with a temperature greater than 38.5°C, so the data provided on the symptom of fever do not contain much information for patient care, since 38.0°C or 38.5°C is considered to the cutoff point for fever.
Finally, we have to consider the benefits and harms of antibiotic treatment. For ABRS, antibiotics might shorten the duration of symptoms and prevent complications.3-6 However, complications (ie, orbital, intracranial, and soft-tissue involvement due to acute rhinosinusitis) are rare, with annual incidence rates that vary from 2.5 to 4.3 per million patients. 8 Further, antibiotic treatment carries a high risk of adverse effects 7 and of antimicrobial resistance, when antibiotics are unnecessarily prescribed or if the type or dosage is not adequate.22,23
Conclusion and Recommendation
Recommendations to differentiate between an acute viral and bacterial rhinosinusitis based on fever and facial and dental pain are currently not supported by evidence. The decision to prescribe antibiotics in adults suspected of ABRS should therefore not be based on the presence of 1 or 2 of these symptoms. For the design and reporting of future diagnostic accuracy studies, researchers should adhere to the STARD reporting standards. 24
Translation into Clinical Practice
You informed the patient presenting to your clinic with complaints suggestive for ABRS that we cannot distinguish between a viral or bacterial pathogen based on her symptoms of fever and facial and dental pain, because this is not supported by evidence. You explain that given the low risk of complications of acute rhinosinusitis, the limited effect of antibiotic treatment for her complaints, and the risk of side effects and antimicrobial resistance, you will not prescribe antibiotics for her episode of uncomplicated acute rhinosinusitis.
Author Contributions
Disclosures
Footnotes
Acknowledgements
We gratefully thank Bianca Kramer, medical information specialist at the library of the Utrecht University and clinical librarian at the University Medical Center Utrecht, for her assistance and advice in searching and retrieval of studies.
No sponsorships or competing interests have been disclosed for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.