
Abstract
Reinke’s edema is a benign lesion of the vocal folds affecting the subepithelial space. As part of a study of the management of Reinke’s edema, we aimed to determine the prevalence of dysplasia and malignancy in histologically proven Reinke’s edema. A retrospective analysis of all laryngeal biopsies performed in north Glasgow, United Kingdom, between 2001 and 2010 was carried out. Clinical and pathological data from patients with histologically confirmed Reinke’s edema were recorded with specific respect to the reporting of dysplasia and malignancy. From the 10-year cohort, a total of 3902 laryngeal biopsies were performed. In total, 189 patients (18 males and 171 females) had histologically proven Reinke’s edema. Of this cohort, 170 (90%) had no dysplasia, 16 (8%) had mild dysplasia, 2 (1%) had moderate dysplasia, and 1 (<1%) had severe dysplasia. There was no malignancy reported. In our predominantly female smoking population, the epithelium appears to differentiate to benign Reinke’s edema rather than malignancy. Patients can be reassured with regard to the low risk of malignancy in classic Reinke’s edema.
Reinke’s edema is a benign lesion of the vocal cords affecting the subepithelial space. Typically, the vocal cords are swollen bilaterally and are mobile during phonation. Patients usually present with persistent hoarseness and a low-pitched voice.
Reinke’s edema occurs almost exclusively in moderate to heavy smokers. Other risk factors include voice abuse and gastroesophageal reflux. Patients usually present between 40 and 60 years of age, and women are more often affected than men.
Given the almost universal prevalence of smoking in patients with Reinke’s edema, the coexistence of invasive squamous cell carcinoma or dysplastic changes might be expected in a significant proportion of these patients. To date, it has been reported in several populations that the prevalence of coexistent dysplastic or malignant changes is low. It is important to quantify the risk of malignancy in patients with Reinke’s edema as part of the informed consent for microlaryngeal surgery.
The aim of the study was to determine the prevalence of dysplasia and malignancy in histologically proven Reinke’s edema in north Glasgow, western Scotland, United Kingdom.
Methods
This study has been carried out in accordance with the protocols for the Clinical Governance for Greater Glasgow and Clyde Health Board. We have satisfied the criteria laid down by ENT Scotland.
All patients had flexible laryngoscopy carried out preoperatively to confirm the clinical diagnosis of Reinke’s edema. Excisional microsurgical mucosal biopsies or Hirano procedure were performed depending on the microlaryngeal findings and the surgeon’s preference. The indication for surgery was to improve voice and exclude malignancy.
A retrospective analysis of laryngeal biopsies performed in north Glasgow between January 2001 and December 2010 was carried out using the north Glasgow pathology database. Clinical and pathological data from patients, with histologically confirmed Reinke’s edema, were recorded with specific respect to the reporting of dysplasia and malignancy.
The data were categorized under 4 classifications: no malignancy, severe dysplasia and carcinoma in situ (CIS), mild to moderate dysplasia, and malignancy according to the UK consensus statement on the management of laryngeal dysplasia. 1 Mild dysplasia is diagnosed when cytological and architectural atypia is confined to the basal/parabasal region of the epithelium. Moderate dysplasia is characterized by the atypia involving the middle third of the epithelium, and severe dysplasia sees the atypia involving the upper third. This progression from mild to severe dysplasia is usually accompanied by a worsening degree of cytological atypia (see Figure 1 ).
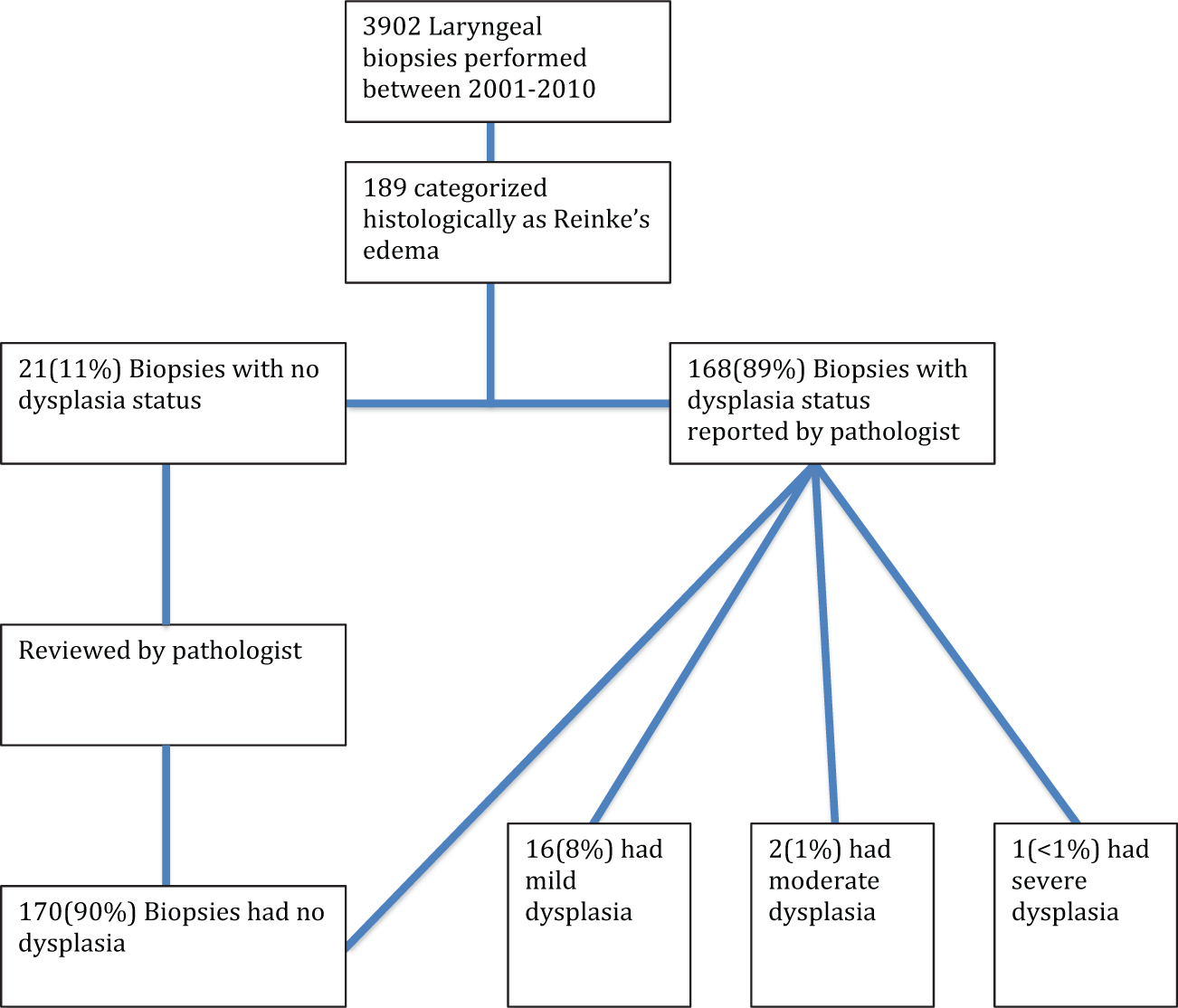
Audit pathway of Reinke’s edema histopathology review.
Results
A total of 3902 laryngeal biopsies were performed between January 2001 and December 2010 in north Glasgow. In that cohort, 189 laryngeal biopsies were categorized histologically as Reinke’s edema. In total, 171 (90.4%) were women with a mean age of 61 years (range, 39-84 years), and 18 (9.6%) were men with a mean age of 63 years (range, 43-87 years).
In our cohort, the histopathologist had explicitly reported the dysplasia status in 168 (89%) patients. Twenty-one patients without dysplasia status subsequently had their laryngeal specimens reviewed by the pathologist (A.M.).
Of the 189 patients, 170 (90%) had no dysplasia changes, 16(8%) had mild dysplasia, 2 (1%) had moderate dysplasia, and 1 (<1%) had severe dysplasia. There was no malignancy reported in our cohort.
Discussion
The clinical diagnosis of Reinke’s edema is confirmed by histological characteristics. The laryngeal squamous mucosa shows changes in the subepithelial connective tissue and surface epithelium, with prominent subepithelial edema accompanied by thin vascular channels and patchy thickening of the epithelial basement membrane. A patchy nonspecific chronic inflammatory infiltrate may also be seen. The squamous epithelium can be thickened and often shows the formation of a thin layer of surface keratin. 2 It has been demonstrated that the edema of subepithelial tissue in general is more frequent in women than in men, which is a potential reason why women are more affected than men. 3
Reinke’s edema has a strong etiological association with smoking. In our cohort, all patients were smokers. Given the high prevalence of smoking, there is an expectation that there may be premalignant or malignant changes in conjunction with the Reinke’s edema. To date, there are very few cases of laryngeal cancer reported in patients diagnosed with histologically confirmed Reinke’s edema. Nielsen et al 4 analyzed histopathologic results in 120 patients treated for Reinke’s edema and found 1 case of invasive carcinoma from a patient who had moderate dysplasia on previous biopsy, 30 (25%) patients had mild dysplasia, and the remainder of the group (75%) had no dysplasia. Garcia et al 5 examined 41 cases of Reinke’s edema and only found 1 case with mild dysplasia. Goswami and Patra 6 reported no dysplasia in 92 patients with Reinke’s edema. In our study, 90% of patients did not exhibit any evidence of dysplastic changes. Less than 10% had mild/moderate dysplasia, with only 1 patient having severe dysplasia. There was no reported malignancy in this cohort. The population differences in premalignant changes could be associated with different smoking habits and lifestyle, environmental, and genetic factors. It could be that the case selection, clinical diagnosis, or histological interpretation is different in these reports; nevertheless, it can be concluded that the prevalence of dysplasia and invasive malignancy is extremely low.
The relative low risk of dysplasia in Reinke’s edema is an important factor. When patients consent to have endolaryngeal surgery, they should be counseled with regard to the low risk of malignancy in classic Reinke’s edema. We would advocate that the principal indication for surgical intervention in this group of patients should be the patient’s desire to improve his or her voice while achieving the secondary aim of confirming the lack of malignant change.
Conclusion
In classic Reinke’s edema, patients may be reassured by the low risk of malignancy. Although there is a high prevalence of smoking in patients with Reinke’s edema, the epithelium appears to differentiate to benign changes rather than malignancy. Patients should be advised that the main aim of endolaryngeal surgery is to improve their voice, not exclude malignancy.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.
This article was presented at the 2013 AAO-HNSF Annual Meeting & OTO EXPO; September 29–October 3, 2013; Vancouver, British Columbia, Canada, and at the ENT Scotland Summer Meeting; May 10–11, 2012; Dunkeld, Scotland.