
Abstract
Nasal vestibular stenosis can result in a challenging cosmetic deformity, for which a variety of techniques have been described, including scar excision and replacement with local flaps, composite or cartilage grafts, with or without stents. We describe the Z-plasty technique to widen the alar base and assess patient satisfaction from the surgery. A retrospective review of patients who underwent Z-plasty to the alar subunit for nasal vestibular stenosis over a 4-year period was conducted. Demographic data and patient satisfaction were evaluated using pre- and postoperative visual analog scores and Rhinoplasty Outcome Evaluation questionnaires. Eight patients underwent the procedure, and all confirmed significant improvement in their esthetic outcome. We describe our Z-plasty technique to the alar base and review patient satisfaction.
Alar stenosis is a challenging deformity causing both cosmetic and functional effects. A range of surgeries are described for this and mostly involve excising scar tissue and replacing with healthy tissue. Local flaps and composite or cartilage grafts, with or without stents, have all been used. We describe a Z-plasty technique to correct the deformity associated with nasal vestibular stenosis and describe our experience in managing a series of patients with this challenging deformity.
Surgical Technique for Z-plasty Alar Subunit
Two percent lignocaine with 1:80,000 adrenaline was infiltrated into the lateral alar margin ( Figure 1 ). A Z-plasty incision is centered around the lateral ala ( Figure 1A ), and soft tissue is elevated ( Figure 1B ). Two triangular flaps are transposed ( Figure 1C ) and secured with 4/0 Vicryl to vestibular skin and 5/0 Prolene to cutaneous skin ( Figure 1D ). Postoperatively, topical neomycin (Naseptin) is prescribed for 1 week.
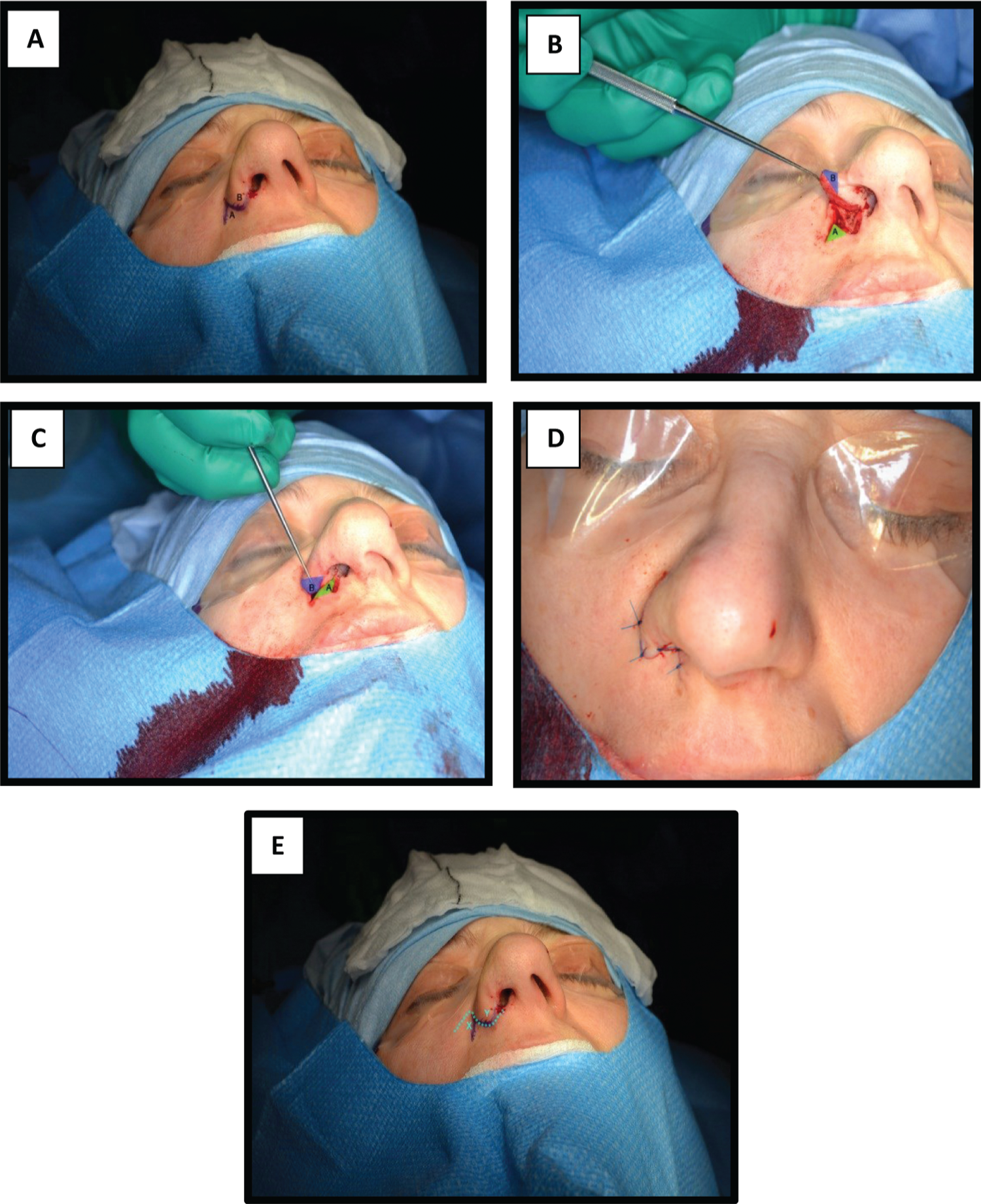
Surgical steps of Z-plasty to the right alar base. (A) Marked out surgical incision lines, demarcating 2 triangular flaps labeled A and B, centered around the right lateral alar margin. (B) Elevation of both triangular soft tissue flaps. (C) Transposition of the 2 triangular soft-tissue flaps. (D) Final skin closure with 5/0 Prolene. (E) Direction of movement of the alar subunit can be varied by changing the axis of flap rotation, as illustrated with alternative skin markings, resulting in flaps X and Y.
Methods
A retrospective review of patients who underwent Z-plasty of the alar subunit by the senior author was conducted. Demographic and clinical data were reviewed. Changes in cosmetic deformity were documented with pre- and postoperative high-resolution medical photographs. Subjective changes were recorded using the visual analog score (VAS) and Rhinoplasty Outcome Evaluation (ROE) questionnaire, before and after surgery. The VAS has not been validated for cosmetic rhinoplasty surgery, but the ROE is already validated for this surgery. 1
This study was reviewed by the Imperial College Joint Research Compliance Office and Imperial College Research Ethics Committee; study and ethics approval was not required.
Results
Eight patients (6 women and 2 men) underwent alar Z-plasty from 2009 to 2013, with a mean age of 33.88 ± 10.18 years (range, 21-51 years). The follow-up period averaged 11.7 ± 13.7 months (range, 3-43 months). One patient was lost to follow-up, as the patient had emigrated following surgery.
All cases of alar scarring were trauma related, including burns (1 case), shrapnel injury (1 case), blunt trauma (2 cases), postseptorhinoplasty surgery (2 cases), tumor excision (1 case), and following skull base surgery resulting in facial palsy, causing failure of nasal dilator muscles (1 case). All patients underwent Z-plasty to the alar subunit without any perioperative complications.
All 8 patients were satisfied with their cosmetic outcomes and said that they would undergo the same procedure again.
Each patient scored their esthetics with respect to the nose on a VAS scale (0 to 10) before and after surgery, with 10 representing their ideal cosmetic appearance ( Figure 2 ). The mean preoperative VAS score was 2.6 and the postoperative VAS score was 6.9, and this difference was statistically significant (Mann-Whitney test: P = .0083).
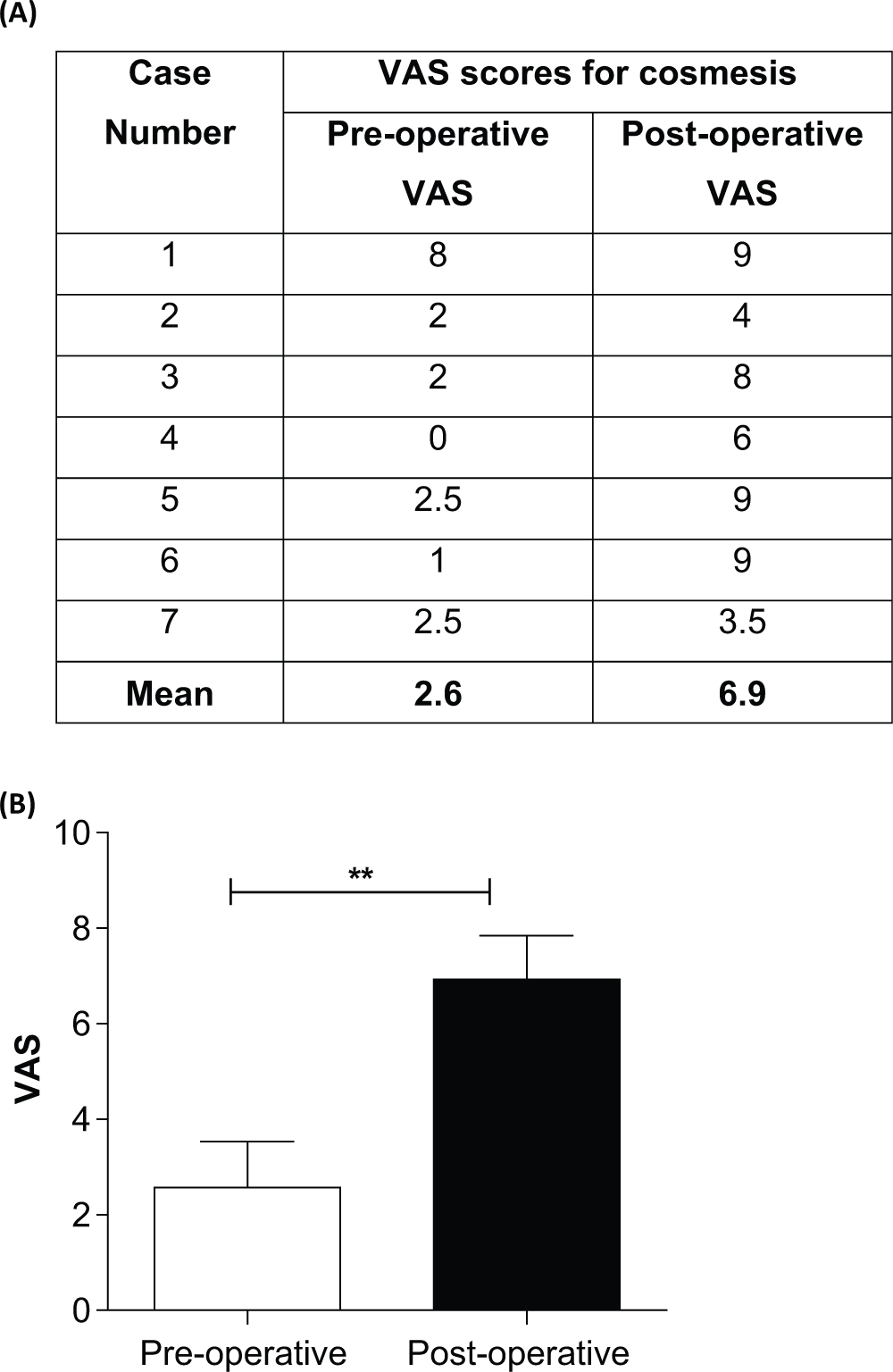
(A). Comparison of pre- and postoperative visual analog scale (VAS) scores for patients who underwent Z-plasty of the alar subunit to correct nasal vestibular stenosis. VAS scores ranged from 0 to 10, where 10 is the ideal cosmesis. (B) Statistical analysis with Mann-Whitney test confirmed a statistical difference in VAS scores. (**P < .01).
Each patient was also asked to evaluate his or her cosmetic outcome using the ROE questionnaire ( Table 1 ). This showed that, overall, patients were satisfied with their outcomes; the first question asked, “Do you like the appearance of your nose,” to which all patients except 1 scored of 3 out of 4. Only patient 2 scored 2 out of 4. This patient had extensive facial injuries following shrapnel injury. Therefore, despite improvement following surgery, this patient’s injuries were far greater than could be corrected. This score reflected residual scarring, which the patient did not think could be further corrected. Overall responses to all other questions gave a positive outcome ( Table 1 ).
Patient Satisfaction Outcome Using the Rhinoplasty Outcome Evaluation (ROE) Questionnaire. a
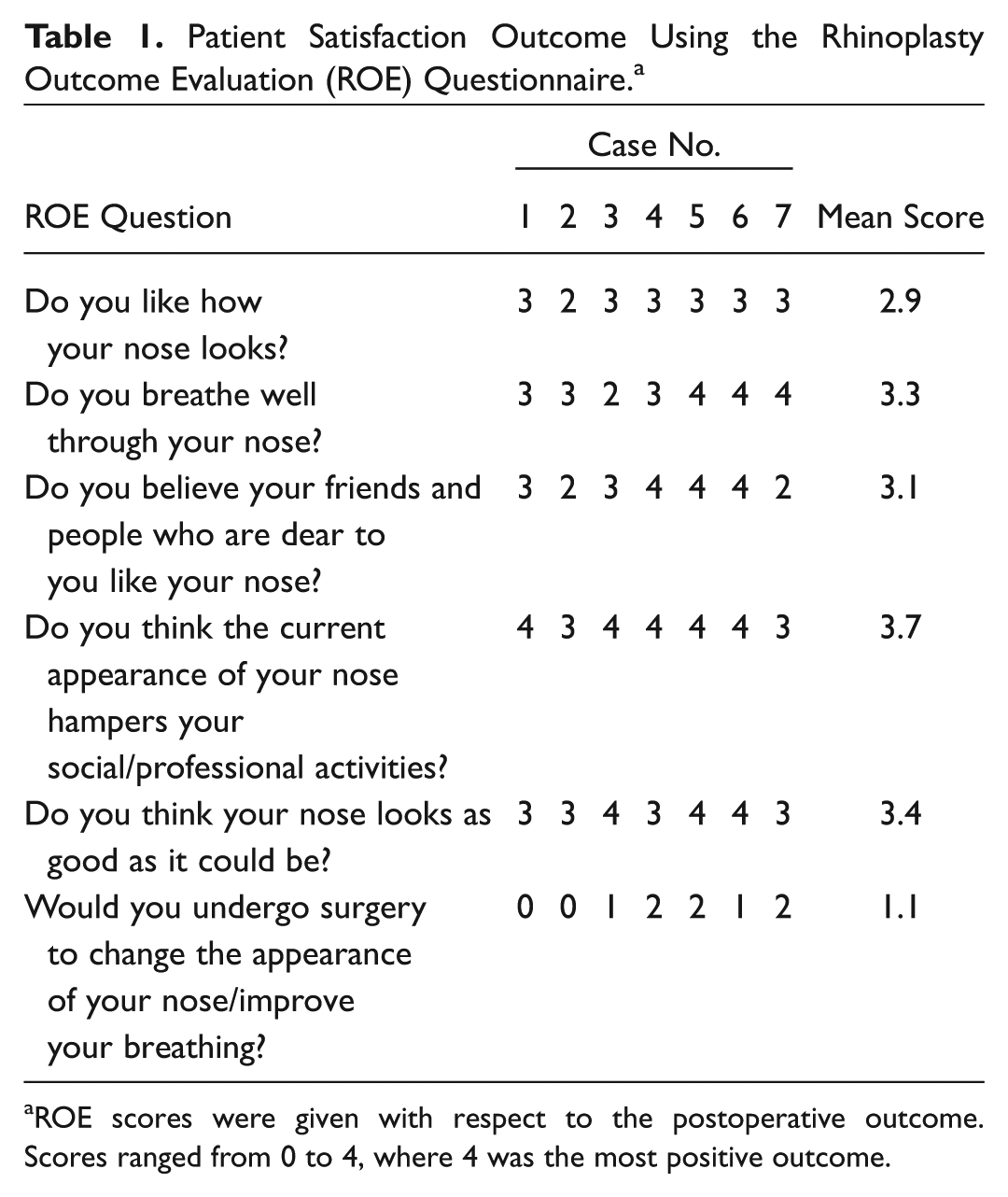
ROE scores were given with respect to the postoperative outcome. Scores ranged from 0 to 4, where 4 was the most positive outcome.
Discussion
Nasal vestibular stenosis resulting from alar scarring is surgically challenging. Most techniques excise scar tissue, but this has the potential for new scar formation, with further contracture. Earlier descriptions involve excising the scarred segment and replacing with a split-thickness skin graft. 2 Some authors introduced the concept of using stents for structural support. 2 However, stents can be uncomfortable and may require cleaning or exchanging. Therefore, other techniques using conchal cartilage or auricular composite grafts have been described. 3
Alternatively, local flaps have also been used, 3 including the alar transposition flap, upper lip flaps, and labial mucosal flap. Although local flaps use healthy, vascularized tissue, they often yield bulky tissue to fill a small defect. Alternatively, the triplanar W-plasty 4 and double-cross plasty 5 have been used where scar tissue is excised in a W or cross shape before stenting.
We have developed a simple Z-plasty technique and believe this is the first report of Z-plasty for the alar subunit. This day-case procedure can be performed under local or general anesthesia. It involves simple incision lines, which can easily be interdigitated to lateralize the alar subunit. It does not involve excising scar tissue but instead repositions the scarred alar subunit to a more lateral position. It also does not require any grafts or stents.
Our Z-plasty technique is suitable for the scarred alar margin, where we have used it to achieve very satisfactory results ( Figure 3 ). It is unsuitable for scarring of the nasal sill or columella or for reconstruction of alar notching. We have used the technique in a select patient group with nasal vestibular stenosis from alar scarring, in which all patients were satisfied with their surgical outcome, showing a statistically significant improvement in the deformity.

Twenty-one-year-old female who was referred with left alar retraction following facial palsy resulting from skull base surgery. Z-plasty of the left alar subunit was performed.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.
This article was presented at the 2013 AAO-HNSF Annual Meeting & OTO EXPO; September 29–October 3, 2013; Vancouver, British Columbia, Canada.