
Abstract
Objective
To examine the role of intratympanic Dexamethasone (ITD) in the prevention of Cisplatin-induced hearing loss.
Study Design
Prospective randomized controlled clinical trial.
Setting
Tertiary referral center.
Subjects and Methods
Twenty-six patients suffering from a neoplastic disease for which the treatment protocol included Cisplatin were recruited. Prior to each Cisplatin treatment session ITD was injected to the baseline randomly assigned ear while the other ear of the same patient served as the control. Audiometry and Distortion Product Otoacoustic Emissions (DPOAEs) test results of the baseline and follow-up examinations were compared within and between the study and control ears.
Results
The cumulative dose of Cisplatin was greater than 400 mg for the 15 subjects who completed the study. The pure tone threshold at 8000 Hz and pure tone average threshold at 4000 to 8000 Hz significantly increased in both the study (P < .005, P < .03, respectively) and control ears (P < .01, P < .005, respectively). Significant increase in the pure tone threshold for 6000 Hz was observed in the control (P < .02) but not in the study group. Within the groups comparison also revealed significant decrease in the DPOAE average signal-to-noise ratio (SNR) for the f2 frequencies 7031 (P < .04) and 8391 Hz (P < .04) and SNR average for 4000 to 8000 Hz in the control (P < .04) but not in the study ears.
Conclusions
ITD significantly attenuated hearing loss at 6000 Hz and decreased the outer hair dysfunction in the DPOAE f2 range of 4000 to 8000 Hz. ITD might have potential in the reduction of Cisplatin-induced hearing loss.
Introduction
Cisplatin is a widely used chemotherapy for the treatment of various malignant neoplasms.1-4 Nephrotoxicity, neurotoxicity, and ototoxicity are the main dose-limiting side effects of Cisplatin. While nephrotoxicity can be controlled with hydration therapy, there are no known preventive treatments available for neurotoxicity or ototoxicity.2,4
Cisplatin-induced hearing loss (CIHL) is characterized by bilateral, symmetric, progressive, and irreversible sensorineural hearing loss. Hearing impairment is dose related, cumulative, and takes place within hours to days from the administration of Cisplatin.1-4 The reported rate of CIHL ranges between 11% and 97%, with an average incidence of 62%.5-7 When the cumulative dose of Cisplatin is greater than 300 mg, the risk of hearing loss is directly correlated with the increase in its dosage. 8 Other risk factors for the development of CIHL include hypoalbuminemia, anemia, very young or very old age, renal failure, usage of loop diuretics, and radiotherapy field, which includes the inner ear organs. 9
The pathogenesis of CIHL is attributed to the creation of reactive oxygen species (ROS) and depletion of antioxidant enzymes. This results in lipid, protein, and nucleic acids peroxidation with Caspase system activation and apoptosis of inner ear cells.4,10-12 The outer hair cells at the basal turn of the cochlea are initially lost to be followed by the remaining outer hair cells, inner hair cells, supporting cells, and spiral gangalion neurons. 13 Advanced ototoxicity damages the stria vascularis and decreases the cochlear blood supply, resulting in reduced endocochlear potential. 14
Various chemoprotectants have been suggested to ameliorate CIHL. These include sodium thiosulfate, amifostine, diethyldithiocarbamate, 4-methylthiobenzoic acid, D- and L-methionine, N-acetylcysteine, and glutathione ester. The mechanisms of action include direct antioxidant activity and maintenance of glutathione levels, which is the main natural ingredient protecting against ROS.1,2,4 Unfortunately, many of these compounds fail to cross the blood–inner ear barrier and the systemic administration resulted in significant side effects including the reduction of Cisplatin anti-neoplastic effect. 1 Therefore, these drugs are currently considered not suitable for human clinical use.1,2,9,15 Recently, gene therapy for Cisplatin ototoxicity has been studied in cell cultures and experimental animal models using different viral vectors, plasmids, or Si-RNA. This potentially promising approach requires further investigation regarding safety, immunogenicity, and consequences of genetic manipulation in the inner ear tissues.16,17
Abundant corticosteroids receptors were demonstrated within the critical inner ear structures suggesting active role of these compounds in inner ear homeostasis.18-20 Corticosteroids have been reported to up-regulate cochlear anti-ROS enzymes activity, reduce the formation of inflammatory molecules, and decrease ototoxicity-induced inner ear cellular apoptosis.2,3,21-23 Currently, systemic steroids treatment is practiced for various inner ear pathologies in which ROS are involved. These include sudden sensorineural hearing loss, noise-induced hearing loss, autoimmune inner ear disease, Ménière’s disease, salicylate and aminoglycoside ototoxicity.2,3,19 Since Cisplatin ototoxicity involves ROS production and depletion of antioxidant enzymes, a rationale for its prevention by corticosteroid is suggested. However, previous studies reported that systemic steroid treatment might result in reduced tumoricidal activity of chemotherapy, which might worsen patient prognosis.24,25
Intratympanic (IT) delivery of drugs is a contemporary method based on the diffusion of the active remedy across the round window into the inner ear where it exerts its therapeutic effects. Higher inner ear concentrations are gained when compared to oral or parenteral administration while avoiding the undesirable systemic side effects, including the potential reduced efficacy of chemotherapeutic agents.24-28
IT administration of steroids, especially Dexamethasone, has been vastly used over the past decades for the treatment of sudden sensorineural hearing loss and Ménière’s disease.26,28,29
The purpose of the present study was to examine the possible role of intratympanic Dexamethasone (ITD) in the prevention of CIHL in a clinical setup.
Methods
Twenty-six patients suffering from a neoplastic disease for which the primary curative-intent treatment protocol included Cisplatin were recruited to a prospective randomized controlled study. Most subjects received additional cytotoxic agents in combination with Cisplatin. These included Bevacizumab, Capecitabine, Docetaxel, Doxorubicin, 5-FU, Gemcitabine, Pemetrexed, Topotecan, Vinorelbine, and VP16. Ototoxicity is not a reported side effect in any of these chemotherapeutic agents.
After signing an informed consent the patients had a baseline evaluation that included detailed history with emphasis on previous or existing ear disease, microscopic otoscopy, pure tone, speech and impedance audiometry, and Distortion Product Otoacoustic Emissions (DPOAEs) testing. The latter was reported to be particularly useful in monitoring early injury to outer hair cells resulting from various etiologies including Cisplatin ototoxicity.7,12,30-32
Exclusion criteria were (1) age <18 years; (2) pathological findings on otoscopy that did not allow safe IT drug delivery and reliable DPOAEs testing; (3) lack of stapedial reflex and type A tympanometry on impedance audiometry; (4) previous inner ear disease that might result in sensorineural hearing loss; (5) conductive hearing loss >5 dBHL; (6) pure tone thresholds average (PTA) >40 dBHL for the frequencies 500 to 3000 Hz or 4000 to 8000 Hz; (7) asymmetry of PTA between the ears >10 dBHL for the frequencies 500 to 3000 Hz or 4000 to 8000 Hz; (8) previous treatment with Cisplatin; and (9) history of radiation therapy to the head and neck regions.
The ears of patients that matched the inclusion criteria for the study were randomly assigned employing a computerized “randomizer” 33 to the study or control groups.
Prior to each Cisplatin treatment session, ITD was injected to the baseline randomly assigned ear while the other ear of the same patient served as the control. The treatment was performed under local anesthesia using a cotton wool soaked with Xylocaine 10%, which was attached to the ear drum for 15 minutes. Between 0.7 and 1.0 ml Dexamethasone Phosphate 10 mg/ml solution, prewarmed to body temperature, was injected to the middle ear using 25 gauge spinal needle via the tympanic membrane posterior inferior quadrant facing the round window niche. The volume of the solution injected aimed to fill the tympanic cavity and varied according to individual anatomy. After the ITD injection, the patient was instructed to lie down for 20 minutes with the treated side up and to avoid swallowing or coughing. These measures were taken to allow maximal contact of the Dexamethasone solution with the round window membrane while minimizing its loss via the Eustachian tube.
Follow-up audiometry and DPOAEs testing were carried by 1 of 2 clinical audiologists who were blinded to the side treated. These were performed 1 week after the cumulative dosage of Cisplatin reached at least 400 mg, a level at which a maximal ototoxic effect is anticipated.1-4,8
The study protocol and procedures were approved by the committee for human experiments, Meir Medical Center, Kfar Saba, Israel, and were registered in ClinicalTrials.gov Internet site (study ID - NCT01372904).
Statistical Analysis
Clinically significant CIHL was defined according to the guidelines of the American Speech-Language-Hearing Association (ASHA) as hearing loss of 20 dBHL or more in a single-frequency or hearing loss of at least 10 dBHL in 2 or more adjacent frequencies. 34
The incidence of clinically significant hearing loss between the study and control ears was compared by the Fisher exact test.
Normal distribution of the audiometry and DPOAEs test results in the baseline and follow-up evaluations was approved by the Shapiro-Wilk test.
The following variables were compared between and within groups: pure tone thresholds (PTT) at 500, 1000, 2000, 3000, 4000, 6000, and 8000 Hz; pure tone averages (PTA) at the frequency range 500 to 3000 and 4000 to 8000 Hz; DPOAEs signal to noise ratios (SNR) for the f2 frequencies 1031, 2063, 2953, 4172, 4969, 5953, 7031, and 8391 Hz; and average DPOAEs SNRs at the f2 frequencies of 1000 to 3000 Hz and 4000 to 8000 Hz.
Comparison between groups was carried out by the unpaired 2-tailed t test and within groups by the paired 2-tailed t test. Bonferroni correction was employed to compensate for multiple comparisons.
Sample size calculation determined that 16 ears in each group were required to complete the study. The calculation was based on the following parameters: α = .05, β = .20, power = 80%, estimated difference = 10, and standard deviation = 10. Statistical analysis was done using SPSS.
Results
Eleven of the 26 patients recruited dropped out from the study. Three patients died of their disease, 2 had cerebro-vascular accident that might have added confound parameter of central hearing loss, in 3 patients the treatment protocol was changed by the attending oncologist before a cumulative dose of 400 mg Cisplatin was reached, and 3 have opted to withdraw their consent for participation in the study ( Figure 1 ).
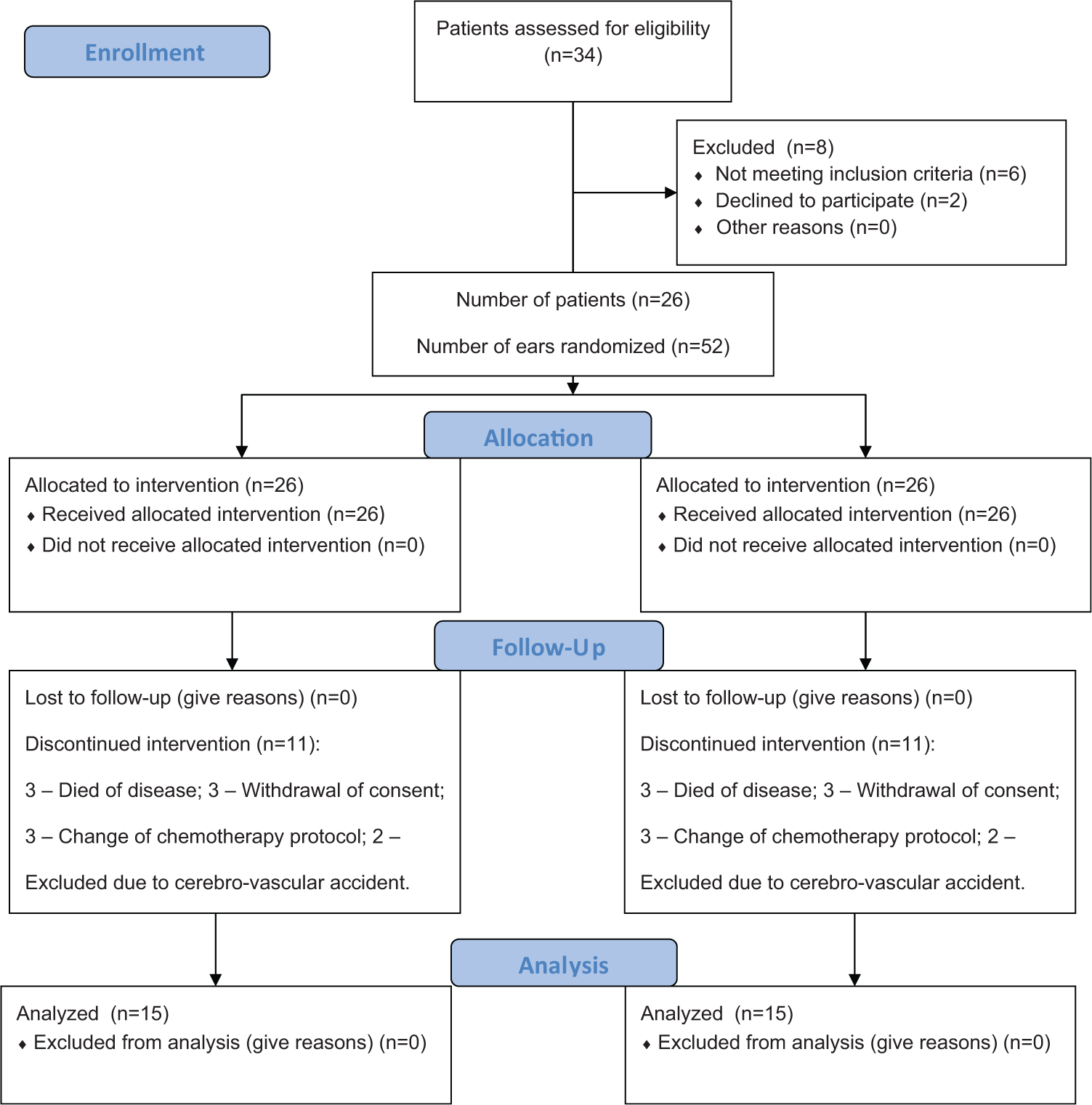
Patient flow diagram.
Nine women and 6 men have completed the study. Their average age ± standard deviation was 61.5 ± 9.8 years (range, 38-80 years). ITD was injected to the right and left ears in 8 and 7 subjects, respectively.
Except for slight pain during injection and short mild vertigo secondary to the uneven caloric stimulation, no side effects were recorded.
The average cumulative dose of Cisplatin was 517 ± 184 mg (mean ± standard deviation; range, 410-1165 mg), and the average number of Cisplatin treatment sessions 5.6 ± 2.5 (mean ± standard deviation; range, 3-11 sessions) spanned over 2 to 6 months. The time elapsed from ITD injection to Cisplatin treatment was 150 ± 59 minutes (mean ± standard deviation; range, 105-315 minutes).
No differences were found between the study and control ears in the baseline audiometric and DPOAEs evaluations.
Significant CIHL as defined by ASHA criteria 34 was diagnosed in 6 (40%) ears of the control and 5 ears (33.3%) of the study group. Intention to treat analysis revealed significant CIHL in 17 control ears (65%) and 16 study ears (62%). The differences between the groups in both “as treated” and “intention to treat” analyses did not reach statistical significance.
Significant increases in the average PTTs at 8000 Hz were found in both the study and control groups: 7.3 ± 9.2 dBHL and 11.3 ± 11.7 dBHL, respectively (P < .005, 95% confidence interval, 2.2-12.5; P < .01, 95% confidence interval, 4.8-17.8, respectively; paired t test).
Significant increase in the PTT for 6000 Hz of 8.7 ± 11.4 dBHL was observed in the control group (P < .02, 95% confidence interval, 2.3-15; paired t test). For the ITD treated group, nonsignificant threshold increase of 2.3 ± 8.8 dBHL was found ( Figure 2 ).
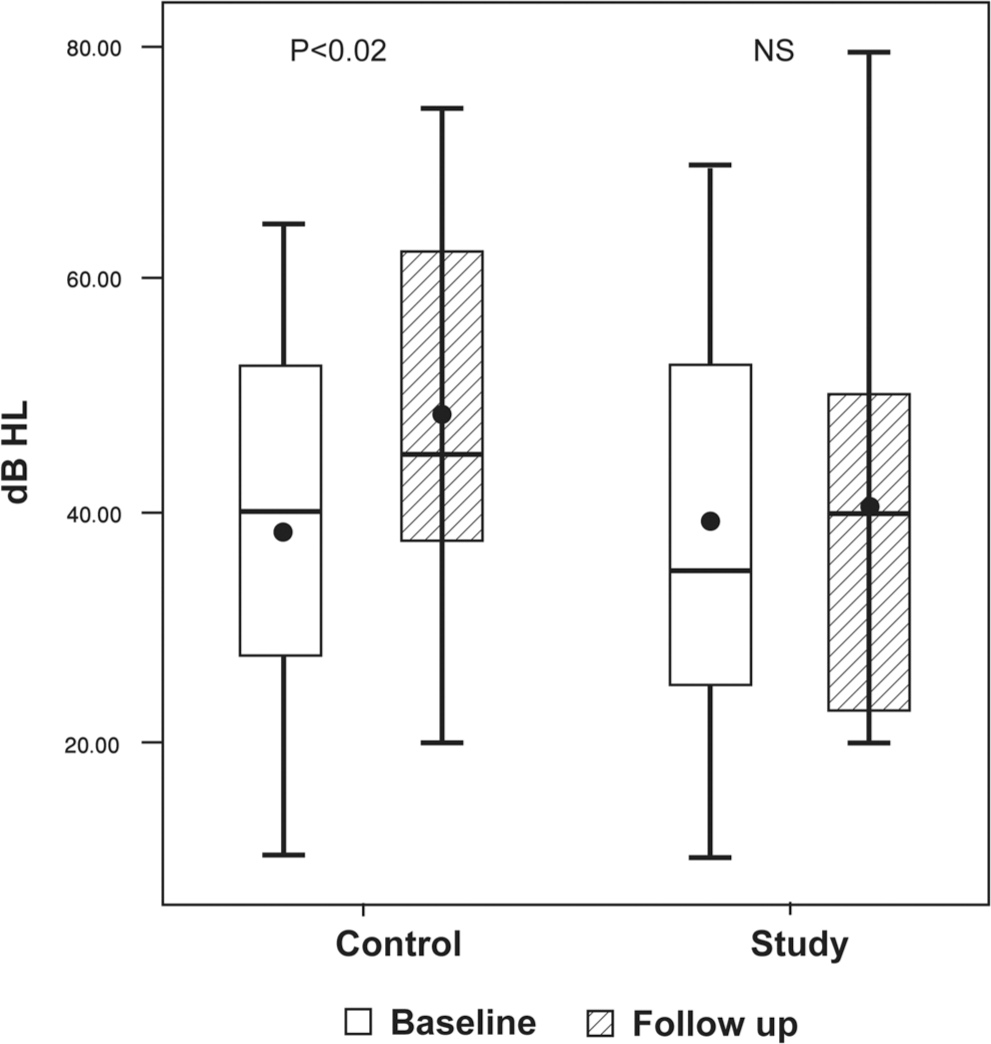
Whiskers plots of the pure tone thresholds at 6 kHz (dBHL), on the baseline and follow-up evaluations in the control and research groups. The threshold increase in the control group was statistically significant (P < .02). NS, not significant.
On the completion of the study, 5 (33.3%) ears of the study group had PTTs for both 6000 and 8000 Hz that were at least 10dBHL lower when compared to those of the contralateral matched ears.
Within the groups, comparison of the PTA for 4000 to 8000 Hz showed significant average increases of 3.9 ± 5.8 and 7.2 ± 7.9 dBHL in the study and control groups, respectively (P < .03, 95% confidence interval, 0.68-7.1; P < .005, 95% confidence interval, 2.8-11.6, respectively; paired t test).
Significant decrease in the DPOAE SNR for 8391 Hz and 7031 Hz of 4.2 ± 1.7 and 2.4 ± 3.9 dBSPL, respectively, were found only in the control group (P < .04, 95% confidence interval, 0.13-4; P < .04, 95% confidence interval, 0.16-4.7, respectively; paired t test).
Significant decrease of 2.6 ± 4.4 dBSPL in the DPOAEs average SNR for the f2 frequencies of 4000 to 8000 Hz was found in the control group (P < .04, 95% confidence interval, 0.16-5; paired t test). The SNR decrease of 1.35 ± 4.1 dBSPL in the study group was not of statistical significance ( Figure 3 ).
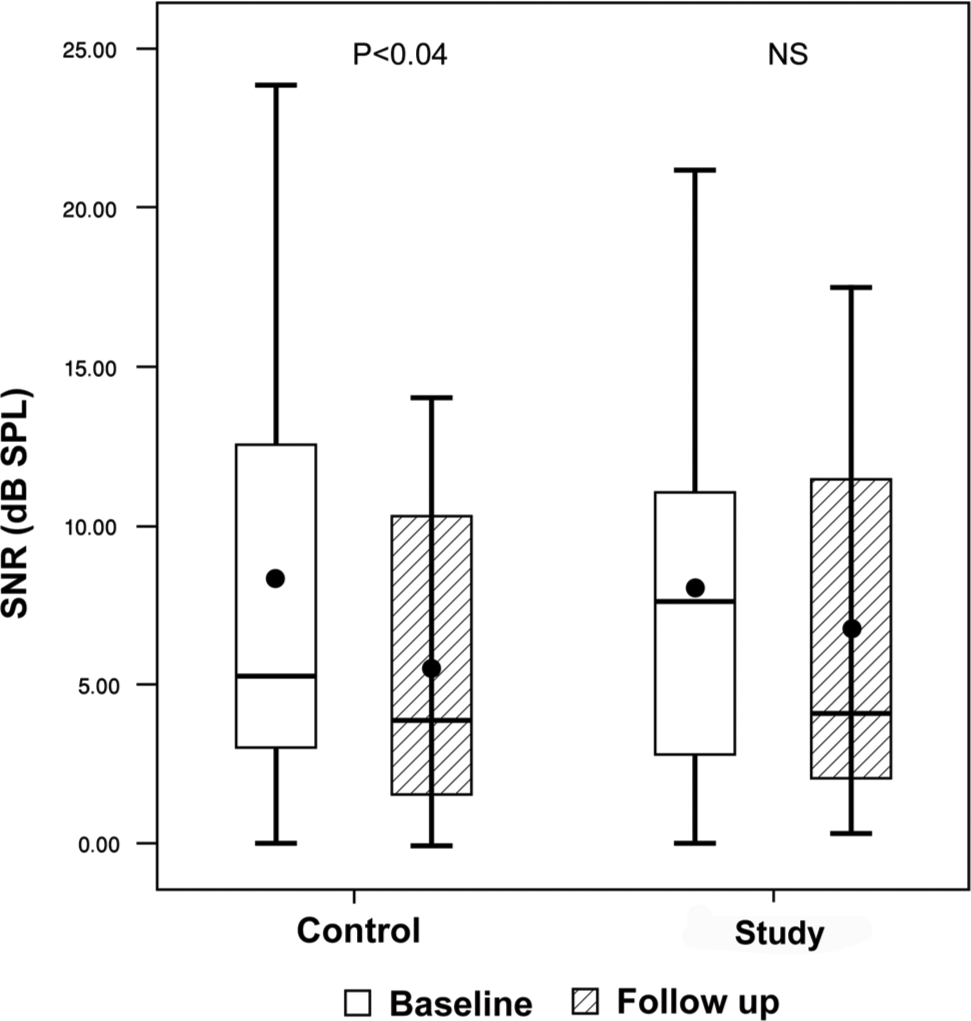
Whiskers plots of the DPOAEs SNR averages (dBSPL) over 4 to 8 kHz, on the baseline and follow-up evaluations in the control and research groups. The SNR decrement in the control group was statistically significant (P < .04). NS, not significant; DPOAEs, Distortion Product Otoacoustic Emissions; SNR, signal-to-noise ratio.
Between the groups, comparisons for the PTTs increase at 6000 and 8000 Hz, PTA for 4000 to 8000 Hz, DPOAEs SNR decrease for the f2 frequencies 7031 and 8391 Hz, and average DPOAEs SNR decrease for the f2 frequencies 4000 to 8000 Hz did not show significant differences. Also, within and between the groups comparisons for the PTTs at 500, 1000, 2000, 3000, and 4000 Hz; PTA at the frequency range 500 to 3000; speech reception thresholds and word recognition scores, DPOAEs SNR at the f2 frequencies 1031, 2063, 2953, 4172, 4969, and 5953 Hz, and average SNR for the DPOAEs at the f2 frequencies of 1000 to 3000 Hz did not reveal any statistically significant differences ( Table 1 , Table 2 ).
Results of Pure Tone and Speech Audiometry on the Baseline and Follow-up Evaluations for Study and Control Groups.
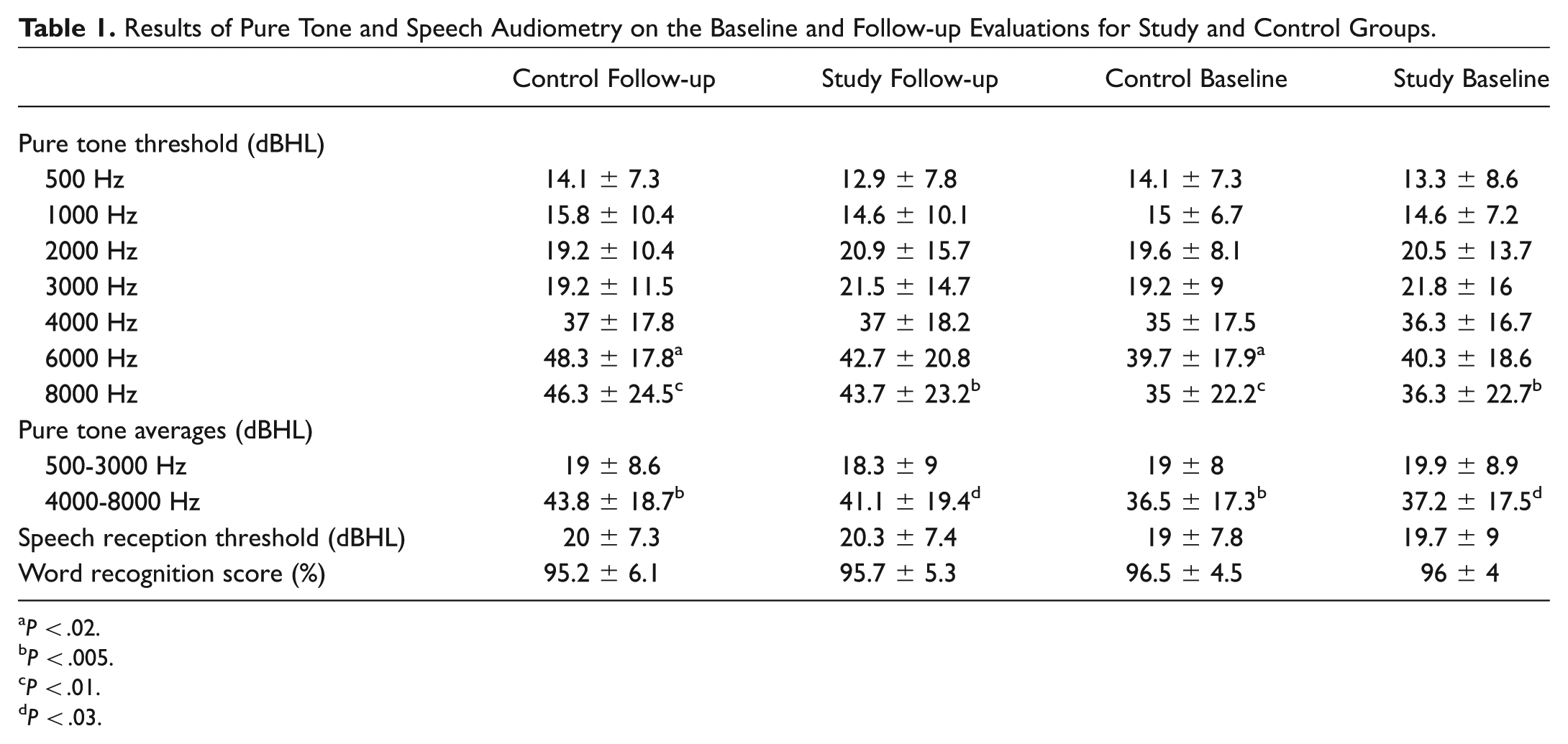
P < .02.
P < .005.
P < .01.
P < .03.
Results of Distortion Product Otoacoustic Emissions (DPOAEs) Tests on the Baseline and Follow-up Evaluations for Study and Control Groups.
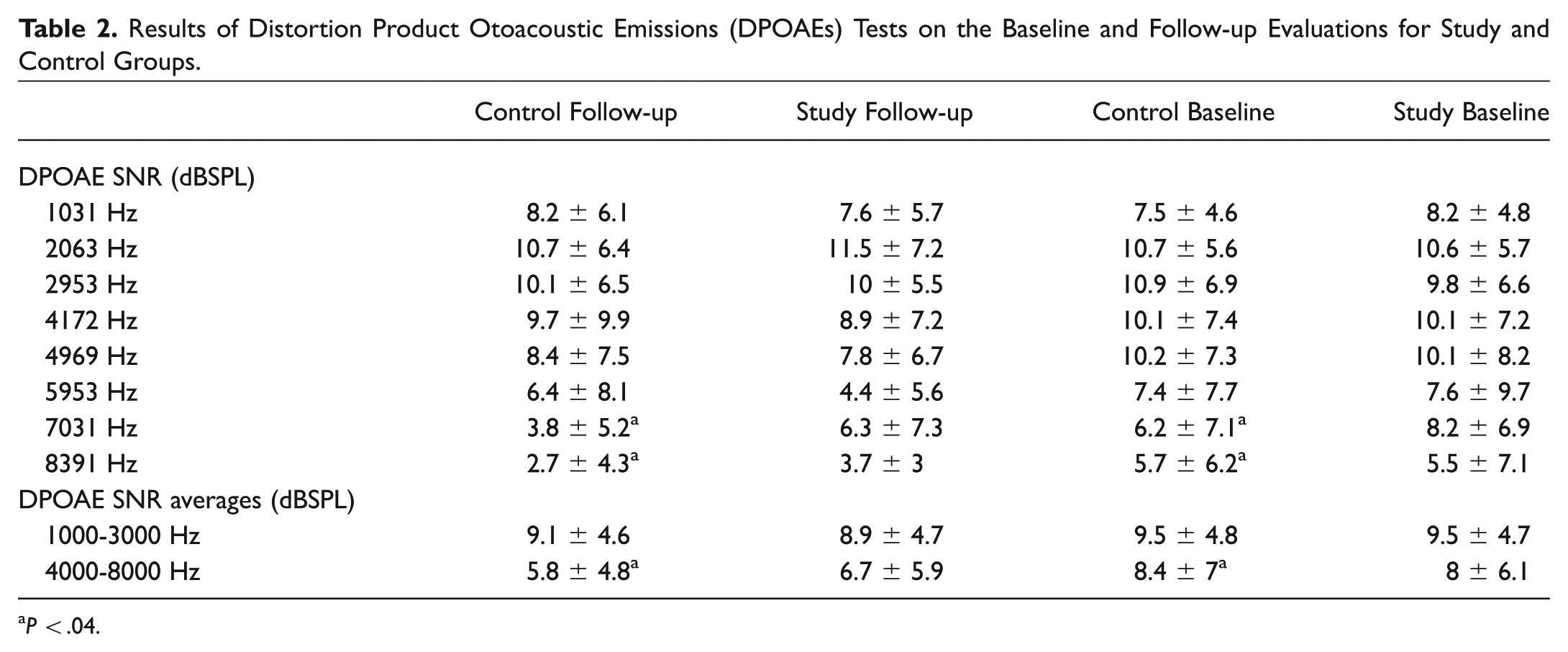
P < .04.
Discussion
The main finding of the study is that ITD delivered shortly before each Cisplatin session provided only minimal protection against CIHL. Although significant threshold increase was observed in both the study and control groups for 8000 Hz, and the PTA of 4000 to 8000 Hz, the increase at 6000 Hz and reduced DPOAE’s SNR for the f2 frequencies 7031 and 8391 Hz and SNR average of 4000 to 8000 Hz was significant only in the control group. Also, on the completion of the study third of the study group ears had at least 10 dBHL better hearing thresholds in both 6000 and 8000 Hz when compared to the contralateral control ears.
The finding that early ototoxic effects caused hearing loss at 6000 and 8000 Hz corroborates with previous reports. 35 The increase in high frequencies pure tone thresholds was accompanied by significant decrease in the DPOAEs average SNR for 4000 to 8000 Hz in the control group confirming previous observations pointing to the organ of Corti outer hair cells as the primary target for Cisplatin ototoxicity.31,32
The specific mechanisms involved in the attenuation of CIHL by Dexamethasone are not known yet. However, recent studies suggest the relevance of various cellular processes that might explain this otoprotection.
High presence of mineralocorticoid and glucocorticoid receptors was observed in the outer and inner hair cells, spiral ganglion neurons, and spiral ligament.18,20,36
The mineralocorticoid receptors demonstrate higher affinity to steroidal hormones, which points to the significant role of steroids in maintaining fluid regime and homeostasis of the inner ear.18,19 The blood-labyrinthine barrier is composed of capillary endothelial cells with tight junctions that inhibit absorption of chemicals from the systemic circulation into the inner ear. Rising level of ROS operates the vascular endothelial cells to secreting of different cytokines that damage the tight junctions, cause violation of the inner ear fluid homeostasis, damaging the endocochlear potential, and hence lead to apoptosis of cell lines in the organ of Corti. 37 Glucocorticosteroids were reported to bring a new creation of the tight junctions between endothelial cells, thus restoring endothelial function in the stria-vascularis. 38
We could not find any previous study that examined ITD in the prevention of CIHL in humans. Yet, beneficial role of ITD has been documented in several small mammals studies. Guinea pigs treated by ITD prior to the intraperitoneal administration of Cisplatin suffered no decrements in DPOAEs SNR or amplitude over 1 to 6 kHz while the untreated control group demonstrated significant derangement of their outer hair cells function. 21 In the young mouse model, ITD before and after Cisplatin delivery provided significant protection from elevation of the auditory brainstem response (ABR) threshold to click and tone-bursts of 8 and 16 kHz but not for the response to 32 kHz. 3 In another guinea pig study employing ABR, ITD attenuated threshold increase to 8 kHz tone burst but not to the 16 and 25 kHz stimuli. 39 It is of interest that in our study significant threshold elevation in 6000 Hz was found only in the non-ITD treated group, while the pure tone threshold at 8000 Hz increased significantly in both groups. Higher vulnerability of the most basal areas of the cochlea to ototoxicity might explain the unfavorable results of ITD in the protection against CIHL in the highest frequency range both in our study and the animal models.3,39 This observation is supported by a guinea pig tissue culture study demonstrating lower levels of glutathione in the base of the cochlea when compared to the apex, thus reflecting intrinsic higher susceptibility to ROS. 40 In rats ITD prevented CIHL as evaluated by ABR to click and tone bursts of 4.8, 12, and 16 kHz. 2 A recent guinea pig study reported that ITD could provide significant otoprotection if performed 1 hour before intraperioneal administration of Cisplatin. However, when ITD treatment preceded Cisplatin administration by 24 hours no preventive effect on CIHL was observed. 41
The inner ear pharmacokinetics of Dexamethasone following intratympanic injection on one hand and that of Cisplatin after intravenous administration on the other hand indicate that ITD in a controlled timing may provide effective protection against Cisplatin ototoxicity. Maximal concentration of Cisplatin in the perilymph was measured 20 minutes after intravenous delivery, declined to about half from its peak after 40 minutes and was below detection after 90 minutes. 42 For Dexamethasone, maximal perilymph level was recorded 1 hour following intratympanic injection. 43 Employing high pressure liquid chromatography and mass spectrometry significant perilymph levels of Dexamethasone were measured within 1 hour from intratympanic injection, which decreased 50- to 100-fold within 12 hours. 44
The advantages of the present study include its prospective randomized design and selection of 1 ear for ITD injection while the second ear of the same subject was the control. As Cisplatin ototoxicity affects both ears equally 45 and patients with significant baseline hearing asymmetry were excluded from the study, this matching procedure avoided many confounding parameters related to the known large inter-individuals variability in the susceptibility to Cisplatin ototoxicity. 9
The main disadvantage of ITD injection technique is the uncertainty about the actual amount of Dexamethasone that reaches the cochlea. Loss of some of the injected solution via the Eustachian tube could not be avoided despite the lying position and avoidance of swallowing and coughing post-injection. Also, no measure was taken to clear obstructing membranes that were reported to cover the round window niche in a significant number of patients. 46
Most study participants had high tone hearing loss on enrollment prior to Cisplatin treatment ( Table 1 ). Since preexisting hearing loss is a risk factor for CIHL and Cisplatin ototoxicity initially affects the higher frequencies, the study results might be biased and larger otoprotection effects of ITD could be demonstrated in a younger population. 45
Maximal therapeutic effects of Dexamethasone are anticipated when its peak concentration in the perilymph correspondences that of the intravenously administered Cisplatin. Animal studies indicate that the optimal timing for ITD would be about 40 minutes before Cisplatin delivery.10,18,42,43 In the clinical realm we found it difficult to follow the ideal timing for ITD injection prior to Cisplatin treatment. This might decrease the potential maximal protective effect of Dexamethasone. Also, larger therapeutic effect might be reached by higher concentration of the drug.
In conclusion, the study shows minimal effect of ITD toward the reduction of Cisplatin ototoxicity. A larger scale research, employing various concentrations to be delivered in precise timing, is required to further investigate the potential role of ITD in the prevention of Cisplatin induced hearing loss.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.
This article was presented at the 2012 AAO-HNSF Annual Meeting & OTO EXPO; September 9-12, 2012; Washington, DC.